REVIEW ARTICLE
FARIA, Laís Figueiredo [1], COSTA, Thalles Ferreira [2], SIMONATO, Luciana Estevam [3], PAIVA, Gabriel Pina [4]
FARIA, Laís Figueiredo. Et al. Tolosa-Hunt Syndrome: Case Report. Multidisciplinary Scientific Journal Núcleo do Conhecimento. Year 05, Ed. 11, Vol. 03, pp. 23-28. November 2020. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/hunt-syndrome
ABSTRACT
Tolosa-Hunt Syndrome (THS), described as a painful ophthalmoplegia, is a rare, idiopathic disease that can affect one or more pairs of cranial nerves, especially the oculomotor, abducens and trochlear nerves. The case report is intended to facilitate the diagnosis of the clinical situation and treatment, made on the basis of corticosteroids and which has a wide response. For this purpose, imaging exams such as Computed Tomography and Magnetic Arterial and Venous Angioresonance, both of the skull, were used to detect possible abnormalities that could be related to THS. The conduct to perform the exams occurred due to signs and symptoms presented by the patient after recurrent episodes. Since the description of the case added to the photographic records can provide references to the characteristics pertinent to THS, in addition to the prognosis, we seek to contribute to the medical community with the possible aspects present in patients, which seem to have some complexity as a result of the unusual occurrence of pathology.
Keywords: Tolosa-Hunt, diagnosis, ophthalmoplegia, imaging tests.
INTRODUCTION
Originally described by Tolosa (1954) and Hunt (1961), Tolosa-Hunt Syndrome (TSH) is a pathology that is difficult to diagnose, this being by exclusion. Studying according to Buscacio (2016) due to periorbital or hemicranial pain associated with ophthalmoplegia of one or more cranial nerves. The pain can be described by the patient as excruciating, stinging, severe. Still according to Monzillo (2005), little scientific knowledge has been added to this disease, with regard to the probable pathophysiological mechanisms, which are still obscure.
Although its etiopathogenesis is unknown, Carrilho (1997) reports that this relatively rare entity is related to a nonspecific granulomatous inflammatory process in the cavernous sinus that tends to undergo spontaneous resolution. Such an evolution would be dramatically shortened by corticosteroids. Imaging exams are essential to diagnose aneurysms and other intracranial vascular malformations, in addition to tumors that may affect cranial pairs.
Based on the International Headache Classification 2014 (ICHD-3, 2014), the study aims to describe the evolution, characteristics and resolution of THS in relation to the clinical case presented.
CASE REPORT
LFF, 20 years old, female, Caucasian, showing no underlying disease, arrived at the Emergency Department (ED) with an apparent eyelid ptosis affecting the right eye, reporting binocular diplopia in upper views and periorbital headache on the injured side, with progressive evolution in 2 days. . The patient said that the episodes had been occurring for 6 years, always at the same time, with failure in diagnosing the pathology, but knowing that it was responsive to treatment with corticosteroids.
She described that she had already undergone several imaging tests such as computed tomography (CT) of the skull, arterial and venous antiresonance of the skull, echo Doppler of the carotid arteries and laboratory tests to detect the presence of autoimmune pathologies, problems in coagulation, among others. However, the only finding was the presence of secretion in the maxillary sinuses on CT performed in a previous episode.
On physical examination, palpebral ptosis was observed on the right, associated with paresis of the medial rectus and superior rectus muscle, deficit in adduction and elevation of the eye bulb, inferring impairment of the oculomotor nerve. The patient did not have ocular hyperemia, tearing, nasal congestion or other signs that could suggest autonomic impairment. Disorders of the neuromuscular junction were also ruled out due to the lack of fatigue in the eye muscles.
The following exams were performed: Magnetic antiresonance artery and venous cranium, complete blood count, anti-HIV, fasting blood glucose, coagulogram, FAN, ESR, CRP and lipid profile. Such analyzes did not show any significant alteration, only left maxillary sinus disease (figure 1).
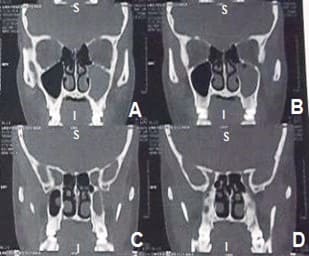
The patient was then medicated with corticosteroid, Prednisone, 1 mg / kg / day with complete remission of the condition in 5 days and referred to a specialist in otorhinolaryngology. The CT requested by the patient showed secretion in the left maxillary sinus obliterating an ethmoidal infundibulum, a slight thickening of the mucous lining of the right maxillary sinus with polyps and cysts (figure 2).
Figure 1: Magnetic arterial and venous antiresonance contrasted in sagittal section revealing left maxillary sinus disease (A to D).
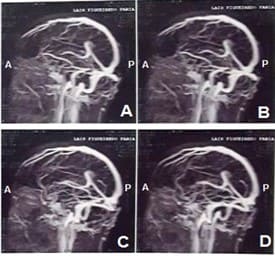
Figure 2: Computed tomography in frontal view showing findings in maxillary sinuses (A to D).
DISCUSSION
Although THS is an uncommon pathology, from the description of the clinical case, it can be seen that the characteristics are congruent with several reports described since its discovery more than 60 years ago. It affects both sexes, with a higher incidence according to Monzillo (2005) between 27 and 58 years of age (average 39.5 years). In the case presented, however, the patient was below the expected age range, demonstrating that it can occur in younger individuals or even children.
According to Kline (2001) the evidences of the imaging exams consist of inflammatory processes, alterations evidenced in the CT of the reported case, which confirm the premise that one of the possible pathophysiological mechanisms of the disease is the presence of nonspecific inflammatory processes, however, in this case. case, not affecting cavernous sinus, but maxillary sinuses.
The affected nerve, oculomotor, in the case presented is in accordance with the literature, because, as stated by Sanvito (1997), the oculomotor nerve is the most affected, followed by the abducent. Trochlear nerve involvement is less frequent. Rarely, the optic nerve may be involved.
The evolution and consequent regression of the pathology after administration of corticosteroids shows the criteria established for diagnosis and treatment described by ICHD-3 beta (2014) (Table 1) and ISH 2004.
| Diagnostic criteria according to ICHD-3 beta |
| A. Unilateral pain fulfilling criterion C |
| B. Both of the following:
1. Granulomatous inflammation of the cavernous sinus, upper orbital fissure or orbit, demonstrated by NMR or biopsy 2. Paresis of one or more of the III, IV and / or VI ipsilateral cranial nerves |
| C. Evidence of causality demonstrated by both of the following
1. Headache that preceded the paresis of the III, IV and / or VI nerves for ≤ 2 weeks or developed with it 2. Headache located around the eye and ipsilateral eyebrow |
| D. Not best explained by another diagnosis of ICHD-3 beta |
In most cases, THS has complete remission, however, occasionally it can leave sequelae. The differential diagnosis according to Beraldin (2013) involves several other pathologies that cause painful ophthalmoplegia, such as diabetic neuropathy, cavernous sinus thrombophlebitis, ophthalmoplegic migraine, tumor lesions. The previously reported patient obtained excellent results and after several episodes it was possible to reach a diagnostic conclusion.
CONCLUSION
Tolosa-Hunt Syndrome is a complex disease, requiring clinical reasoning from the doctor, extensive experience and knowledge. Because it is done from the exclusion, it takes time and the need to perform several exams. The use of surgical methods for cavernous sinus exploration has already been described in the literature, however, as in the case in question, it is not always affected and there is a need for such a procedure, requiring much more than just paying attention to what is most common.
REFERENCES
BERALDIN, B.S. et al. Tolosa-Hunt syndrome mimicking cavernous sinus tumor. Braz. j. otorhinolaryngol., São Paulo, v. 79, n. 2, p. 256, 2013. Disponível em: http://www.scielo.br/pdf/bjorl/v79n2/v79n2a20.pdf
BUSCACIO, E.S. et al. Síndrome de Tolosa-Hunt. Rev. bras.oftalmol., Rio de Janeiro, v. 75, n. 1, p. 64-66, 2016. Disponível em: http://www.scielo.br/pdf/rbof/v75n1/0034-7280-rbof-75-01-0064.pdf
CARRILHO, P.E.M. et al. Síndrome de Tolosa-Hunt: dificuldades no diagnóstico e padrão de resposta à prednisona. Arq. Neuro-Psiquiatr., São Paulo, v. 55, n. 1, p. 101-105, 1997. Disponível em: http://www.scielo.br/pdf/anp/v55n1/16.pdf
HUNT, W.E. et al. Painful ophthalmoplegia. Its relation to indolent inflammation of the cavernous sinus. Neurology.11: p.56–62, 1961. Disponível em: http://www.scielo.br/pdf/rbof/v75n1/0034-7280-rbof-75-01-0064.pdf
KLINE, L. et al. The Tolosa-Hunt syndrome. Journal of Neurology, Neurosurgery, and Psychiatry, 71(5), p.577–582, 2001. Disponível em: http://www.scielo.br/pdf/rbof/v77n5/0034-7280-rbof-77-05-0289.pdf
MONZILLO, P.L. et al. Síndrome de Tolosa-Hunt: análise de seis casos. Arq. Neuro-Psiquiatr., São Paulo, v. 63, n. 3a, p. 648-651, 2005. Disponível em: http://www.scielo.br/pdf/anp/v63n3a/a17v633a.pdf
SANVITO, W.L. Síndromes neurológicas. 2.Ed. São Paulo: Atheneu, 1997.
Subcomitê de Classificação das Cefaleias da Sociedade Internacional de Cefaleia. Classificação Internacional das Cefaleias. 3.Ed. Trad. Sociedade Brasileira de Cefaleia. São Paulo, p. 138-139, 2014. Disponível em: https://www.ihs-headache.org/binary_data/2086_ichd-3-beta-versao-pt-portuguese.pdf
TOLOSA, E. Periarteritic lesions of the carotid siphon with the clinical features of a carotid infraclinoidal aneurysm. Journal of Neurology, Neurosurgery, and Psychiatry, 17(4), p.300–302, 1954. Disponível em: http://www.scielo.br/pdf/anp/v55n1/16.pdf
[1] Medical student.
[2] Medical student.
[3] PhD in Biomedical Engineering. Master in Dentistry. Ongoing specialization in Dental Radiology and Imaging. Improvement in Qualification in Lasertherapy. Improvement in current and multidisciplinary aspects in oncology. Improvement in minor oral surgery. Improvement in minor oral surgery. Graduation in Dentistry – Araçatuba.
[4] Advisor. Ongoing master’s degree in Health Sciences. Specialization – Medical residency. Specialization in Internship in training in Neuromuscular Diseases. Graduation in Medicine.
Submitted: September, 2020.
Approved: November, 2020.















