ORIGINAL ARTICLE
ALMEIDA, Roberta Ferraz [1], FECURY, Amanda Alves [2], DENDASCK, Carla Viana [3], DIAS, Claudio Alberto Gellis de Mattos [4]
ALMEIDA, Roberta Ferraz et al. Effectiveness of an indigenous Amazonian regional kit in neonatal auditory screening in Belém do Pará. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 09, Ed. 03, Vol. 02, pp. 25-40. March 2024. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/amazonian-regional-kit, DOI: 10.32749/nucleodoconhecimento.com.br/health/amazonian-regional-kit
ABSTRACT
Hearing loss can occur at different physiological levels and degrees, primarily affecting children. Law No. 12,303/2010, known as the ‘Otoacoustic Emissions Test Law,’ requires newborns to undergo auditory screening. Different non-calibrated sound instruments can be used to perform behavioral auditory screening: plastic harmonica, spoon tapping on a cup, rubber toys, drums, straw maracas, and gourd maracas, with the latter three being of indigenous origin. The objective of this study is to verify the effectiveness of an indigenous Amazonian regional kit in neonatal behavioral auditory screening in Belém do Pará. A quantitative descriptive study was conducted for this purpose. The evaluated auditory kit with regional instruments proved to be effective, assessing the newborn’s main reflexes. It also demonstrated the simplicity of a detection method and the feasibility of its inclusion in routine neonatal screening methods, enabling the early diagnosis and monitoring of deafness in newborns, which can be presented as an alternative, especially in locations that do not have traditional equipment.
Keywords: Neonatal auditory screening, NIAS, Indigenous, Amazon.
1. INTRODUCION
Hearing is the sense used by the human body for cognitive learning, speech, and language, resulting in the complete socialization of the individual. These processes can be impaired in case of hearing loss, which can occur at different physiological levels and degrees, primarily affecting children (Valadares, 2023).
Through Law No. 12,303/2010, known as the “Otoacoustic Emissions Test Law,” the procedure of conducting auditory screening in newborns became mandatory. This test, recognized nationally and internationally (Universal Neonatal Screening – UNS), is the first diagnostic mode, aiming for early intervention in the treatment of hearing loss (Pimentel; Figueiredo; Lima, 2020).
The screening is recommended to be performed within 48 hours after birth, in the maternity ward, and can be postponed up to 30 days after delivery. Early diagnosis provides immediate care for rehabilitation attempts (Casol and Mendes, 2020).
According to the World Health Organization (WHO), hearing loss is a public health challenge, affecting approximately 34 million people worldwide (Dutra; Cavalvanti; Ferreira, 2022). In children, this amounts to one in 300 to 1,000 (Botelho et al., 2022). According to Brazilian data, the prevalence of hearing loss in childhood is one to six per 1,000 live births (Vieira and Duarte, 2020).
The northern and northeastern regions showed an increase in UNS coverage after Federal Law No. 12,303/2010, but coverage rates are still lower compared to other regions of the country. A larger number of hospitals cannot offer this screening due to biases such as extensive territorial expanse and social inequalities, hindering access to healthcare (Paschoal; Cavalcanti; Ferreira, 2017).
In the maternity wards of the Unified Health System (SUS) in the northern and northeastern regions of the country, there is lower efficiency in the implementation of the UNS protocol. There are several reasons for this, including the lack of infrastructure, specific equipment, specialized workforce, and awareness among newborns’ caregivers (Rodrigues, 2020).
There are two ways to assess hearing in neonates. The objective way includes testing the elasticity of the eardrum, the presence or absence of hearing, and the brain’s interpretation of sound. These tests are performed with electroacoustic equipment. The subjective screening method tests the existence of a reaction to sound, based on the behavior presented, the association between a visual stimulus and the response to sound, and the physical response to the presented sound stimulus. Sound instruments (Valadares, 2023), with different sound intensities, are used for this purpose, offered rapidly for loud sounds and continuously and for a long duration for medium and weak sounds (Lewis, 1996; Basseto, 1998; Botasso, 2022).
The instruments that can be used to elucidate a reflex in the child are non-calibrated sound instruments (the bell; agogo; black-black; rattle, among others), and calibrated sound instruments (pure tones and narrowband noise). Non-calibrated instruments are capable of providing frequent auditory responses. In 1996, a commercial sound kit was developed with non-calibrated instruments of high, medium, and low intensity for such evaluation (Lewis, 1996; Botasso, 2022), available for purchase to this day (Cta, 2024).
According to Almeida e Silva (2001) and Botasso (2022), several different non-calibrated sound instruments can be used to perform behavioral auditory screening: plastic harmonica, spoon tapping on a cup, rubber toys, drums, straw maracas, and gourd maracas, with the latter three being of indigenous origin.
The North region of Brazil, like others, is below the target set by the Multiprofessional Committee on Auditory Health in Brazil (COMUSA) for the application of this screening (UNS). This seems to be based on the historically manifested social inequality, both inter- and intraregionally, among SUS users. Access to healthcare services and inadequate actions reflect the disparity in the country’s levels of economic and social development. We also have to consider the lack of the professional responsible for UNS, the speech therapist, and of adequate equipment in this region (Cruz and Ferrite, 2014).
2. OBJECTIVE
To verify the effectiveness of an indigenous Amazonian regional kit in neonatal behavioral auditory screening in Belém do Pará.
3. METHOD
A descriptive quantitative study was conducted. Quantitative research, according to Almeida (2021), “considers that everything can be quantified, treats data as numbers, using statistical resources such as percentage, mean, mode, standard deviation, median, among others.” Descriptive research “aims to describe the characteristics of a particular population or phenomenon. They can also be elaborated with the purpose of identifying possible relationships between variables” (Moitinho; Gonsalves; Pilenghy, 2023).
The first evaluated the efficiency of the acoustically treated regional auditory kit, as well as verified the hearing of the newborn, through the observation of the presence or absence of reflexes. The descriptive quantitative approach was developed at the end of this research, based on the results obtained.
The screening was conducted in two maternity hospitals, between February and November 2001, one from a public hospital and the other from a private hospital in the municipality of Belém, State of Pará, namely: Fundação Hospital Das Clínicas Gaspar Viana and Ordem Terceira respectively. The research time at Hospital das Clínicas was 15 days, during which 45 Newborns (NB) were screened, with 19 females and 26 males. At Ordem Terceira, the research time was 30 days, and 100 NBs were screened, with 45 females and 55 males. The necessary information was obtained to verify whether the NB is predisposed to hearing impairment (through anamnesis). The testing itself was performed with the newborn, through observation of the NB’s reflex behavior after a sound stimulus.
3.1 INDIGENOUS INSTRUMENTS USED
In this screening, instruments with non-calibrated broad-spectrum sound signals, called Drum, Straw Maraca, and Gourd Maraca, were used, obtained from the National Indian Foundation.
3.2 ACOUSTIC ANALYSIS OF THE INSTRUMENTS
The instruments with non-calibrated broad-spectrum sound signals used in this study were acoustically tested at the Experimental Laboratory of Acoustic Physics at the University of Amazonia (UNAMA – Belém do Pará), where the intensities were measured using a Precision Sound Level Meter, NA-27 (Sound Level Meter 1/3 Octave Band Analyzer), manufactured by Riom. This equipment is capable of reaching frequency ranges from 12.5 Hz to 125,000 Hz or 12 kHz. It is also able to measure decibels.
First, the background noise of the room was checked, i.e., noise from two different points in the environment, so that it would not interfere with the measured intensities of each instrument.
All instruments were played at a distance of 50 cm from the microphone of the device, first with a strong intensity and then with a weak intensity, within a 1-minute interval. This analysis was conducted to verify the acoustic characteristics of each instrument, i.e., whether when played they would reach low, medium, and high frequencies.
3.3 STAGES OF THE NB EVALUATION IN THE SCREENING WITH THE KIT
The data collection was carried out in two stages: In the first stage, the completion of identification forms and authorization for testing by the parents or guardians of the NB with or without indication of the presence of early or late risk factors for deafness was conducted; brief anamnesis directed in the form of a questionnaire. In the second stage, the screening itself was performed, that is, the observation of the NB’s behavioral reflex responses to sound stimuli, where the researcher (competent and trained for this purpose) sought to observe and describe the response patterns to sound stimuli. The behavioral evaluation procedure during the work followed the proposal of Andrade (1996), which in turn is based on the proposal of Northern and Downs (1989), corroborated by Botasso (2022).
The NBs in the rooming-in were tested in the presence of the mother, always 2 hours after feedings, with the child preferably in light sleep, in a closed room, with few people, adequate artificial and/or natural lighting, and pleasant temperature, so that the NB feels comfortable. A sound stimulus of increasing intensity was presented, laterally, at a distance of 20 cm from the child’s auricle, lasting 2 seconds, with a 30-second interval between manipulations.
4. RESULTS AND DISCUSSION
Figures 1, 2, and 3 show the acoustic analysis, in Hertz (Hz) and Decibels (dB), of each of the indigenous instruments.
The analysis in Figure 1 shows that the frequencies used to verify the intensities of the indigenous drum were 250, 500, 1000, 2000, 3000, 4000, 6000, 8000 Hz.
Figure 1. Shows the frequency (Hz) and decibels (dB) of the indigenous drum
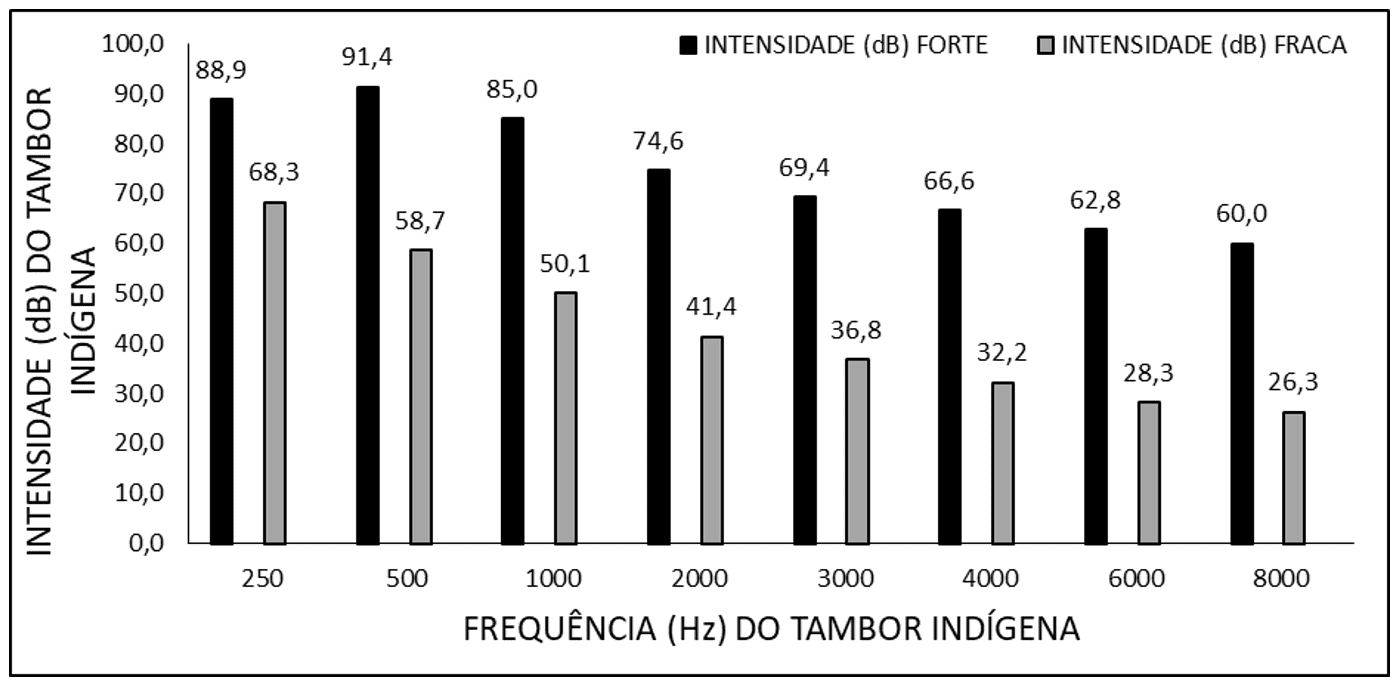
This instrument presented a variable from 60 to 91.4 dB, with a peak at the frequency of 500 Hz when played with strong intensity and a variable from 26.3 to 68.3 Hz, with a peak at 250 Hz when played with weak intensity. This acoustic characteristic is similar to the standardized auditory drum, being considered a low-pitched instrument (Simonek and Lemos, 1996; Botasso, 2022).
The analysis in Figure 2 shows that the frequencies used to verify the intensities of the indigenous straw maraca were 250, 500, 1000, 2000, 3000, 4000, 6000, 8000 Hz.
Figure 2. Shows the frequency (Hz) and decibels (dB) of the indigenous straw maraca
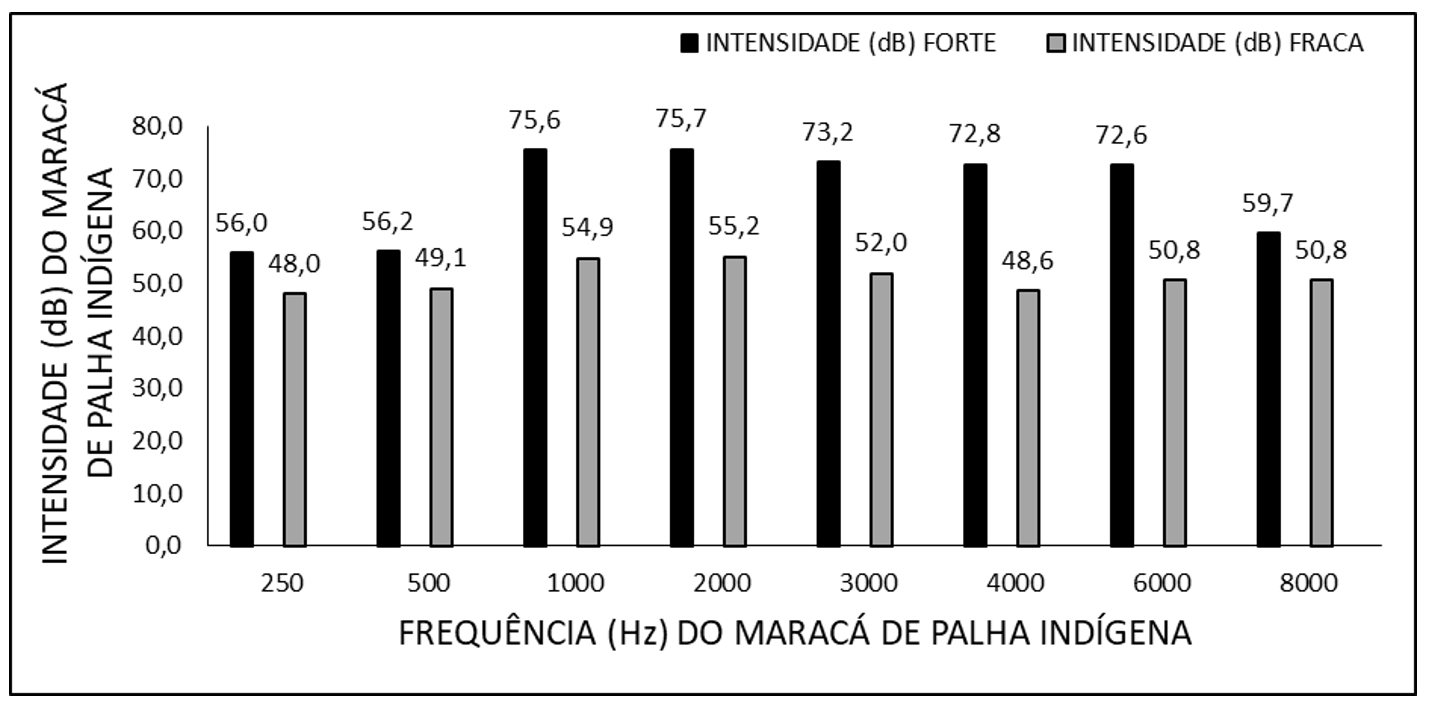
This instrument presented a variable from 56.0 to 75.7 dB with a peak at the frequency of 2000 Hz when played with strong intensity and a variable from 48.0 to 55.2 Hz, with a peak at the frequency of 2000 Hz when played with weak intensity.
This acoustic characteristic is similar to the agogô (large bell) of the standardized auditory kit, being considered a medium-intensity instrument (Simonek and Lemos, 1996; Botasso, 2022).
The analysis in Figure 3 shows that the frequencies used to verify the intensities of the indigenous gourd maraca were 250, 500, 1000, 2000, 3000, 4000, 6000, 8000 Hz.
Figure 3. Shows the frequency (Hz) and decibels (dB) of the indigenous gourd maraca
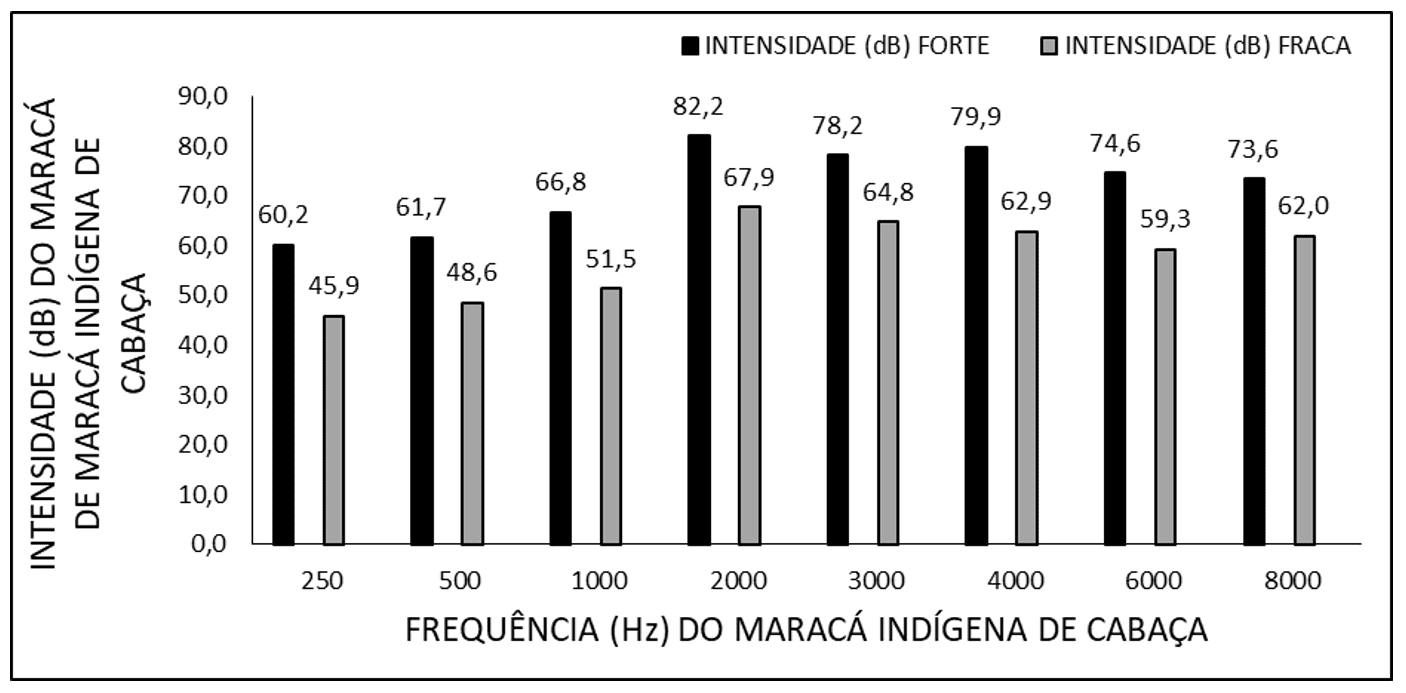
The instrument used was the gourd maraca, which presented a variation from 60.2 to 82.2 dB with a peak at the frequency of 2000 Hz when played with strong intensity and a variable from 45.0 to 67.9, also with a peak at 2000 Hz when played with weak intensity. This acoustic characteristic corresponds to the bell and the rattle of the traditional auditory kit, which are considered high-pitched instruments (Simonek and Lemos, 1996; Botasso, 2022).
The data of the Cochleo-Palpebral Reflex (CPR) in neonates, according to the type of non-calibrated indigenous sound instruments, in behavioral auditory screening are shown in Figure 4.
Figure 4. Shows the percentage of Cochleo-Palpebral Reflex (CPR) in neonates, according to the type of non-calibrated indigenous sound instruments
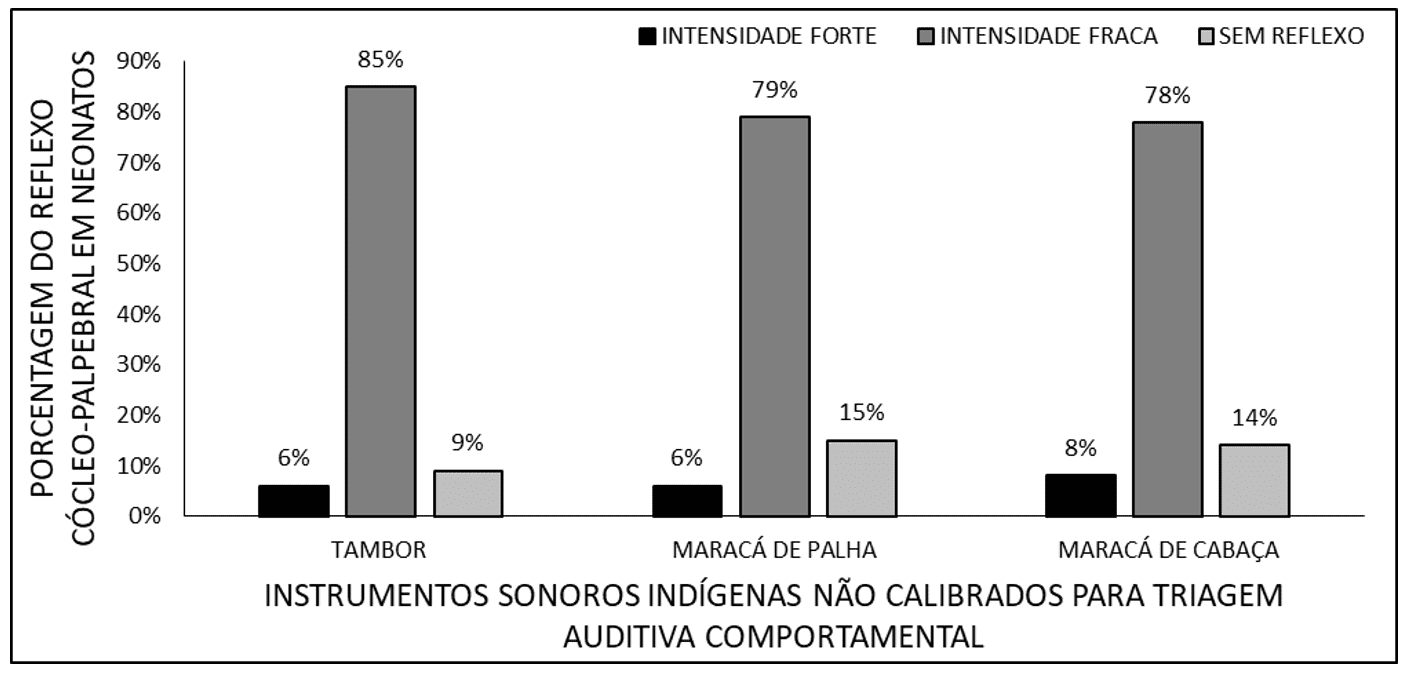
There was a predominance of Cochleo-Palpebral Reflex (CPR) for all instruments when played with strong intensity (123 cases – 85% with the drum; 114 cases – 79% with the straw maraca, and 142 cases – 78% with the gourd maraca). Of the babies who did not respond at this intensity, the CPR was investigated with strong intensity, with responses in 9 cases – 6% with the drum; 9 cases – 6% with the straw maraca, and 11 cases – 8% with the gourd maraca; the remaining cases remained without reflex (13 cases – 9% with the drum, 22 cases – 15% with the straw maraca, and 20 cases – 14% with the gourd maraca).
To detect the presence of hearing, screenings were performed with low intensity (between 49 and 55 dB) using the three sound instruments, with an average CPR observed of 81%. This is one of the most frequent reflexes in neonates (Northern and Downs, 1989; Marone et al., 2020).
The data of the Startle/Moro reflex in neonates, according to the type of non-calibrated indigenous sound instruments, in behavioral auditory screening are shown in Figure 5.
Figure 5. Shows the percentage of Startle/Moro reflex in neonates, according to the type of non-calibrated indigenous sound instruments
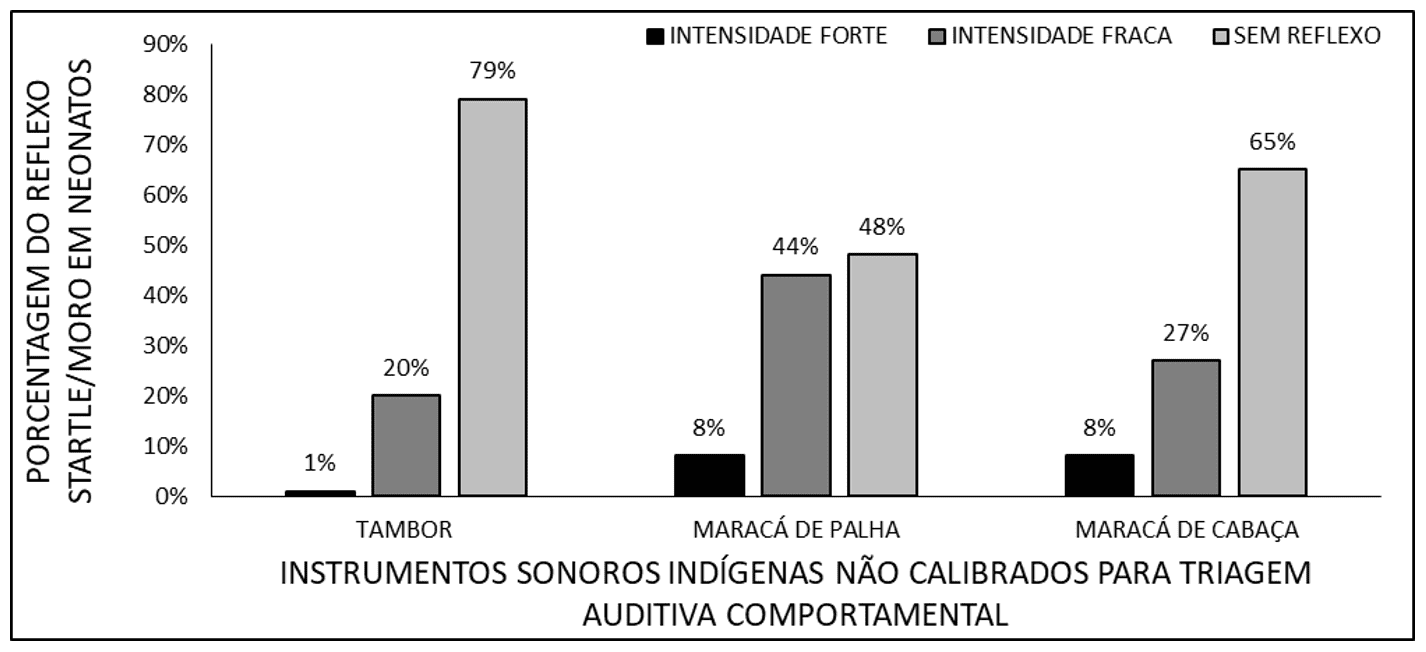
It was observed that the majority of screened babies did not exhibit a startle/Moro reflex (Startle (startle reaction)/Moro (sudden whole-body movement), according to Fernandes (2021), when the instruments were played (110 cases – 79% with the drum, 76 cases – 48% with the straw maraca, and 94 cases – 65% with the gourd maraca). Of those who exhibited reflexes at low intensity, 29 cases – 20% occurred with the drum, 64 cases – 44% with the straw maraca, and 30 cases – 27% with the gourd maraca. Reflexes at high intensity occurred in 1 case – 1% when the drum was played; 11 cases – 8% when the straw maraca was played; and 12 cases – 8% when the gourd maraca was played.
Thirty percent (30%) of neonates, on average, exhibited a startle/Moro reflex. This reflex is commonly present in newborns (NB) up to 6 weeks of age (Andrade, 1996; Souza, 2015).
The data of the cephalic reflex in neonates, according to the type of non-calibrated indigenous sound instruments, in behavioral auditory screening are shown in Figure 6.
Figure 6. Shows the percentage of cephalic reflex in neonates, according to the type of non-calibrated indigenous sound instruments
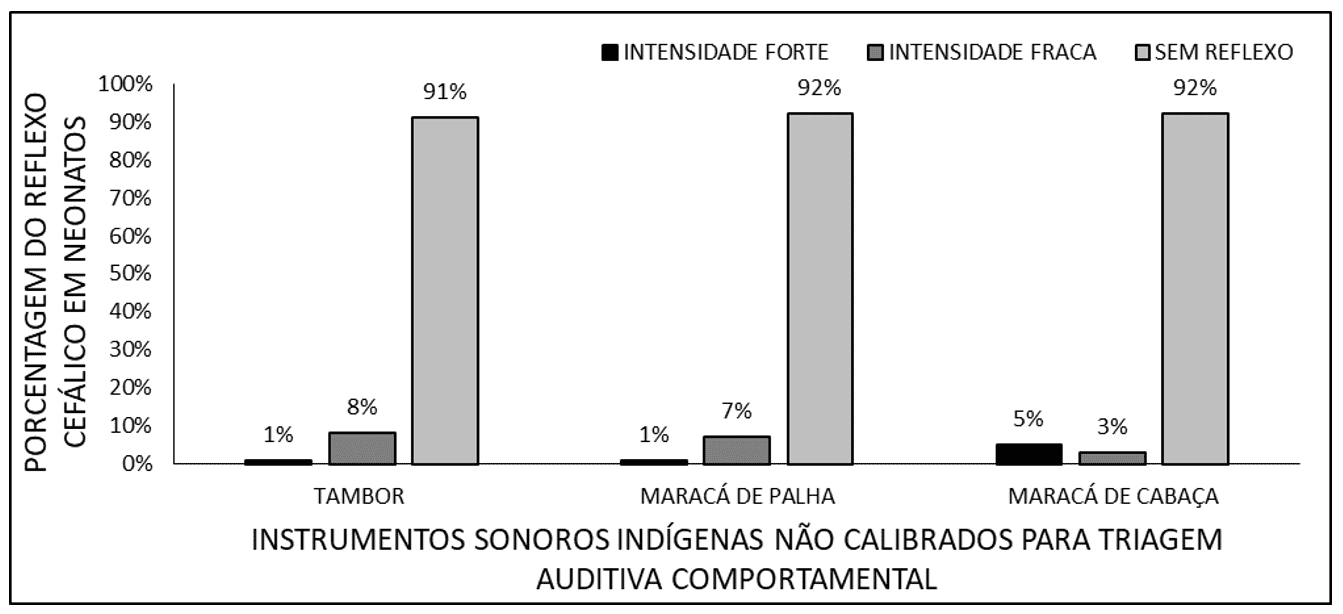
In most newborns, cephalic reaction was not observed (133 cases – 91% with the drum; 134 cases – 92% with the straw maraca, and 133 cases – 92% with the gourd maraca). In 11 cases – 8% with the drum, 10 cases – 7% with the straw maraca, and 5 cases – 3% with the gourd maraca, this reaction could be observed with weak intensity. With strong intensity, it occurred in 1 case – 1% with the drum; 1 case – 1% with the straw maraca, and 7 cases – 5% with the gourd maraca.
The cephalic reaction occurred, on average, in 6% of cases, but this was present with weak intensity and with direct localization for lateral sounds. This does not correspond to the findings of Northern and Downs (1989), who report that direct localization for lateral sounds only occurs around 4 to 7 months. However, there are more recent studies that demonstrate the ability to recognize lateral sounds at 60 days of age (Costa, 2020).
The data of sleep arousal in neonates, according to the type of non-calibrated indigenous sound instruments, in behavioral auditory screening are shown in Figure 7.
Figure 7. Shows the percentage of sleep arousal in neonates, according to the type of non-calibrated indigenous sound instruments
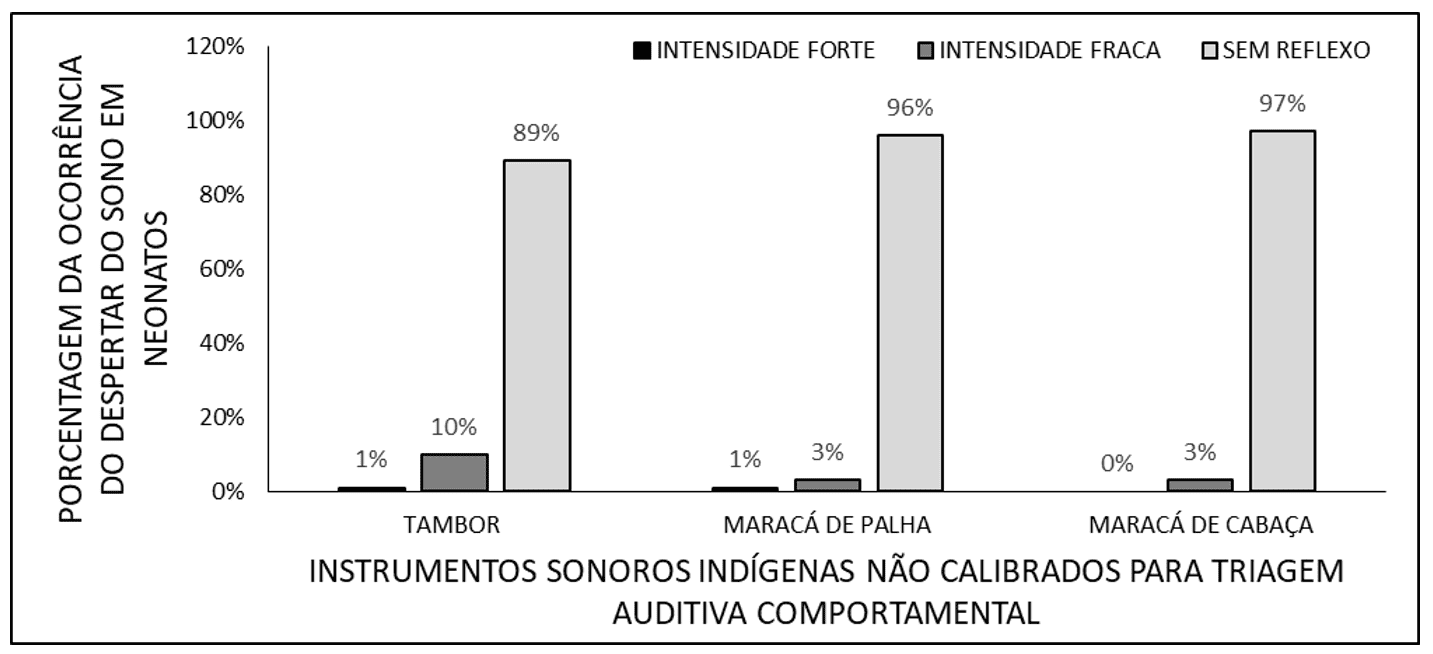
Sleep arousal occurred, on average, in 5% of cases. Most children who responded to low intensities do not need screening at high intensity. A newborn is only able to wake up from sleep in a sound environmental intensity of 70 to 75 dB (Russo and Santos, 1994), with locations of 45 dB or less advised for neuroauditory health (Abrunheiro, 2023).
5. CONCLUSIONS
The evaluated auditory kit with regional instruments proved to be effective, assessing the main reflexes of the newborn. It also demonstrated the simplicity of a detection method and the feasibility of its inclusion in routine screening methods in neonatal services, enabling the early diagnosis and monitoring of deafness in newborns, which can be presented as an alternative, especially in locations that do not have traditional equipment.
REFERENCES
ABRUNHEIRO, C. I. D. R. Práticas promotoras do sono do recém-nascido pré-termo em unidades de cuidados intensivos neonatais: revisão integrativa. Escola Superior de saúde de Viseu. Viseu PT. 2023.
ALMEIDA, I. D. Metodologia do trabalho científico. Recife: Ed. UFPE, 2021. 51 p. Disponível em: <https://repositorio.ufpe.br/bitstream/123456789/49435/1/METODOLOGIA%20DO%20TRABALHO%20CIENT%C3%8DFICO.pdf>. Acesso em: 15 mar.2024.
ALMEIDA, R. F.; SILVA, R. L. D. S. Triagem Auditiva Neonatal Utilizando Kit Auditivo Regional. 2001. 62p. (Graduação). UNAMA, Belém do Pará PA.
ANDRADE, C. R. F. D. Fonoaudiologia Em Bercario Normal E De Risco. Ribeirão Preto SP: Editora Lovise, 1996. 280p.
BASSETO, M. C. A. T. Triagem auditiva em berçário. In: BASSETO, M. C. A.;BROCK, R., et al (Ed.). Neonatologia: um convite a atuação fonoaudiologia. São Paulo SP: Editora Lovise, 1998. p.374 p.
BOTASSO, K. D. C. Implantação E Desenvolvimento De Um Programa De Saúde Auditiva Infantil Ambulatoria. 2022. 149p. (Doutorado). Universidade Estadual de Campinas Campinas SP, 2022.
BOTELHO, J. B. L. et al. Seguimento de crianças com diagnóstico de surdez em programa de triagem auditiva neonatal em Manaus. Rev Saude Publica, v. 56, n. 120, p. 1-10, 2022.
CASOL, K.; MENDES, K. Triagem auditiva neonatal universal: conhecimento de profissionais da saúde atuante em hospital. Revista Thêma et Scientia, v. 10, n. 1, p. 106-118, 2020.
COSTA, F. C. S. Tradução, adaptação cultural e validação do school companion sensory profile 2 para crianças brasileiras. 2020. 149 p. (Mestrado). USP, Ribeirão Preto SP, 2020.
CRUZ, L. R. L.; FERRITE, S. Cobertura estimada da triagem auditiva neonatal p usuários do Sistema Único de Saúde, Brasil, 2008-2011. Rev. Bras. Saúde Matern. Infant., v. 14, n. 4, p. 401-411, 2014.
CTA. Kit Auditivo III. Rio de Janeiro RJ, 2024. Disponível em: < http://www.surdez.com.br/pagina.asp?categoria=13 >. Acesso em: 15 mar. 2024.
DUTRA, M. R. P.; CAVALVANTI, H. G.; FERREIRA, M. A. F. Programas de triagem auditiva neonatal: indicadores de qualidade e acesso aos serviços de saúde. Rev. Bras. Saúde Mater. Infant., v. 22, n. 3, p. 601-607, 2022.
FERNANDES, R. Universo do surdo: os desafios da aquisição da Lingua Brasileira de Sinais na educação infantil. 2021. 136 p. (Mestrado). UNINOVE, São Paulo SP, 2021.
LEWIS, D. R. As habilidades auditivas do recém nascido e a triagem auditiva neonatal. In: ANDRADES, C. R. F. (Ed.). Fonoaudiologia em berçário normal e de alto risco. São Paulo SP: Editora Lovise, 1996. p.280 p.
MARONE, S. et al. Comitê Brasileiro sobre Perdas Auditivas na Infância – CBPAI. Jornal de Pediatria. 77. 1-7, 2020. Disponível em: <https://www.researchgate.net/publication/344874815_Comite_Brasileiro_sobre_Perdas_Auditivas_na_Infancia_-_CBPAI>. Acesso em: 13 mar. 2024.
MOITINHO, G. C. D. O.; GONSALVES, M.; PILENGHY, M. M. O. Aplicação do método markup para formação de preço em uma indústria de uniformes. 9º Forum Rondonense de Pesquisa. Ji Paraná RO: Centro Universitário São Lucas 2023.
NORTHERN, J. L.; DOWNS, M. P. A audição em crianças. São Paulo SP: Manole, 1989. 421p.
PASCHOAL, M. R.; CAVALCANTI, H. G.; FERREIRA, M. F. Análise espacial e temporal da cobertura da triagem auditiva neonatal no Brasil (2008-2015). Ciência & Saúde Coletiva, v. 22, n. 11, p. 3615-3624, 2017.
PIMENTEL, M. C. R.; FIGUEIREDO, N.; LIMA, M. L. L. T. Construção e validação do Modelo Lógico do Programa de Triagem Auditiva Neonatal. Rev. CEFAC, v. 22, n. 4, p. 1-9, 2020.
RODRIGUES, R. P. Avaliação Da Implantação Do Programa De Triagem Auditiva Neonatal Em Maternidades Públicas Brasileiras. 2020. 126p. (Mestrado). Fundação Oswaldo Cruz, Rio de Janeiro RJ, 2020.
RUSSO, I. C. P.; SANTOS, T. M. M. D. Audiologia infantil. São Paulo SP: Editora Cortez, 1994.
SIMONEK, K. M. C.; LEMOS, P. V. Surdez na lnfâncla: diagnóstico e terapia. Rio de Janeiro RJ: Editora Design Studio, 1996. 107 p.
SOUZA, G. L. D. Características Audiológicas Relacionadas Ao Baixo Peso, Prematuridade, Anóxia/Hipóxia E Infecções Congênitas Ao Nascimento: Da Triagem Auditiva Neonatal Ao Diagnóstico. 2015. 98 p. (Metsrado). UNICAMP, Campinas SP, 2015.
VALADARES, A. C. Comparação entre potenciais evocados auditivos de estado estável, potenciais evocados auditivos de tronco encefálico por clique e avaliação comportamental em uma população pediátrica. 2023. 52p. (Mestrado). Universidade Federal de Minas Gerais, Belo Horizonte MG, 2023.
VIEIRA, G. D. S. P.; DUARTE, J. L. Incidência de indicadores de risco para a deficiência auditiva de acordo com o Joint Committee on Infant Hearing emumprograma de triagem auditiva neonatal credenciado ao Sistema Único de Saúde. Aracajú SE, 2020. Disponível em: <https://ri.ufs.br/bitstream/riufs/14115/2/IncidenciaIndicadoresRisco.pdf>. Acesso em: 10 mar. 2024.
[1] Speech therapist, Specialist in Neurology Rehabilitation from the State University of Pará (UEPA); Specialist in Orofacial Motricity with a focus on Hospital Speech Therapy from the Superior School of the Amazon (ESAMAZ); Specialist in Intensive Therapy from the International University Center (UNINTER) and Specialist in Special Education from Descomplica Digital College. Educational Speech Therapist at the Municipal Government of Macapá – AP, assigned to the Special Education Division and Technical Responsible for the Hospital Speech Therapy Service of the Government of Amapá assigned to the ICU of the Osvaldo Cruz Emergency Hospital. ORCID: https://orcid.org/0009-0002-7823-3245.
[2] Biomedical scientist, PhD in Tropical Diseases (UFPA), Professor and researcher in the Medicine Course at the Macapá Campus, Federal University of Amapá (UNIFAP), in the Postgraduate Program in Health Sciences (PPGCS/UNIFAP), and in the Postgraduate Program in Science and Mathematics Teaching (RedECIM). ORCID: https://orcid.org/0000-0001-5128-8903.
[3] PhD in Communication and Semiotics. PhD in Psychology and Clinical Psychoanalysis from the Pontifical Catholic University of São Paulo (PUC/SP). Master’s degree in Religious Sciences from the Mackenzie Presbyterian University. Master’s degree in Clinical Psychoanalysis. Bachelor’s degree in Biological Sciences. Bachelor’s degree in Theology. Has been working for over 15 years with Scientific Methodology (Research Method) in guiding the Scientific Production of Master’s and PhD students. Specialist in Market Research and Research focused on the Health area. ORCID: https://orcid.org/0000-0003-2952-4337. Lattes: https://lattes.cnpq.br/2008995647080248.
[4] Biologist, PhD in Behavior Theory and Research (UFPA), Professor and researcher at the Institute of Basic, Technical, and Technological Education of Amapá (IFAP), in the Professional and Technological Education Postgraduate Program (PROFEPT IFAP), and in the Postgraduate Program in Biodiversity and Biotechnology of the Legal Amazon (BIONORTE Network – Amapá Pole – UNIFAP). ORCID: https://orcid.org/0000-0003-0840-6307. Currículo Lattes: http://lattes.cnpq.br/8303202339219096.
Material received: March 14, 2024.
Material approved by peers: March 15, 2024.
Edited material approved by authors: March 15, 2024.















