ORIGINAL ARTICLE
ARAGÃO, José Aderval [1], TRINDADE, João Gabriel Santana [2], BATALHA FILHO, Airton Lima [3], ARAGÃO, Iapunira Catarina Sant’Anna [4], ARAGÃO, Felipe Matheus Sant’Anna [5], KUHN, Caio Siqueira [6], FEITOSA, Vera Lúcia Correa [7], REIS, Francisco Prado [8]
ARAGÃO, José Aderval. et al. Morphology of the bifid xiphoid process or foramen: is there a difference in cadaver or imaging?. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year. 08, Ed. 06, Vol. 03, pp. 35-46. June 2023. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/morphology-of-the-bifid, DOI: 10.32749/nucleodoconhecimento.com.br/health/morphology-of-the-bifid
ABSTRACT
Context: Anatomical variations of the sternum are frequent, in particular, the occurrence of foramina and divisions of the xiphoid process. The authors have used means of investigation ranging from dissection to imaging tests to detect these variations. Objective: To report a case of bifid xiphoid process in a male human fetus and/or xiphoid foramen through macroscopic analysis, complemented by the use of X-ray image. Case report: Anatomical variations were found at the level of the xiphoid appendix of the sternum such as a bifid formation of the appendix and a foramen found on X-ray imaging, located in the middle of a fibrous tissue that separated the two divisions of the xiphoid process. Conclusion: The present findings point to the need for greater collaboration in the use of other methods for studying the anatomical variations of the sternum. For example, Multidetector Computed Tomography (MDCT). This will be of great value to anatomists and specialists in imaging diagnostics.
Key words: Morphology, Bifid xiphoid, Anatomy, Cadaver.
1. INTRODUCTION
The human body has many anatomical variations. Knowing these variations is important to avoid diagnostic errors during radiological interventions, prevent injuries from medical error during invasive procedures, as well as facilitating the interpretation of physical examinations. The sternum is a bone in which anatomical variations have been frequently studied, based on imaging examinations, autopsies, and in dry skeletons. [9]
The sternum bone is a flat bone located vertically in the middle and anterior part of the thoracic cage, it articulates with the clavicles and the ribs, and has three parts, the manubrium, the body and the xiphoid process.[10]–[12] The xiphoid appendix, located at the level of the epigastrium, has the function of attaching anteriorly fibers of the rectus abdominis muscle, aponeurosis of the internal and external oblique muscles, as well as fibers of the diaphragm muscle, transversus thorax and posteriorly the costoxiphoid ligaments, [13],[14] and it has one or two ossification centers, which appear in the 1st decade of life and are generally completed in middle age and old age. [12],[15] In early life, the xiphoid process is cartilaginous and ossifies in adulthood, with the transition of the xiphoid joint from symphysis to synostosis around age 40. [16] Failure of the sternal bars to migrate, unite or ossify can result in variations. [17]
Morphologically, in most people, the xiphoid process appears as a single, tapering bony projection, but it can also appear as wide, slender, pointed, bifid, perforated, curved, or bent, and have a foramen.[9], [16] The formation of a sternal foramen can occur from the incomplete fusion of ossified segments.[18] For Pasieka et al.,[19] this would result in a complete perforation of the manubrium, body and/or xiphoid process, which could occur once or several times at any point along the sternum These variations in the sternum have challenged health professionals when performing physical examinations, interpreting chest imaging tests and performing surgical procedures on the anterior chest wall. [11],[12], [20] In this article, we tried to report the finding using the X-ray technique to complement the macroscopic analysis, comparing it to other techniques reported in the literature.
2. CASE REPORT
During routine dissection, at the Human Anatomy Laboratory of the Federal University of Sergipe, of a male fetus, obtained in accordance with Law No. 8501 of November 30, 1992, which addresses the use of unclaimed cadavers for use in research studies, aged approximately 34 weeks, some anatomical variations were observed at the level of the sternum, especially in the xiphoid process. In the anterior view of the sternum, a ventral convexity was found extending from the manubrium to the body, and a concavity was found in the xiphoid process. This process started from the posterior face of the body of the sternum, had a caudal direction and projected obliquely in the posteroanterior direction, forming an angle of approximately 20 degrees (Figure 1). In posterior view, there was another concavity that extended from the manubrium to the proximal end of the xiphoid process. Observed with the naked eye, the xiphoid process did not appear to have a break in continuity with the body of the sternum. From the body of the sternum, this process bifurcated into two other processes: one on the right, more caliber and 7 mm long, and another on the left, thinner, 8 mm long, which followed towards the right process, making an angle of approximately 120 degrees. The two processes were separated from each other by a distance of 5 mm and a whitish connective tissue could be seen between them, without presenting foramen, observed with the naked eye (Figure 2). However, in the radiography of the sternum, it allowed the visualization of an image compatible with that of a foramen in the xiphoid process, measuring 25 mm² in area, as well as four ossification centers, one in the manubrium and three in the body of the sternum (Figure 3).
Figure 1. Ventral view of the sternum display a concaveness and angulation of the sternum of the sternum

Figure 2. Dorsal view of the sternum showing the two xiphoid processes separated by connective tissue and without a foramen visible to the naked eye

Figure 3. Area of the xiphoid foramen and ossification centers
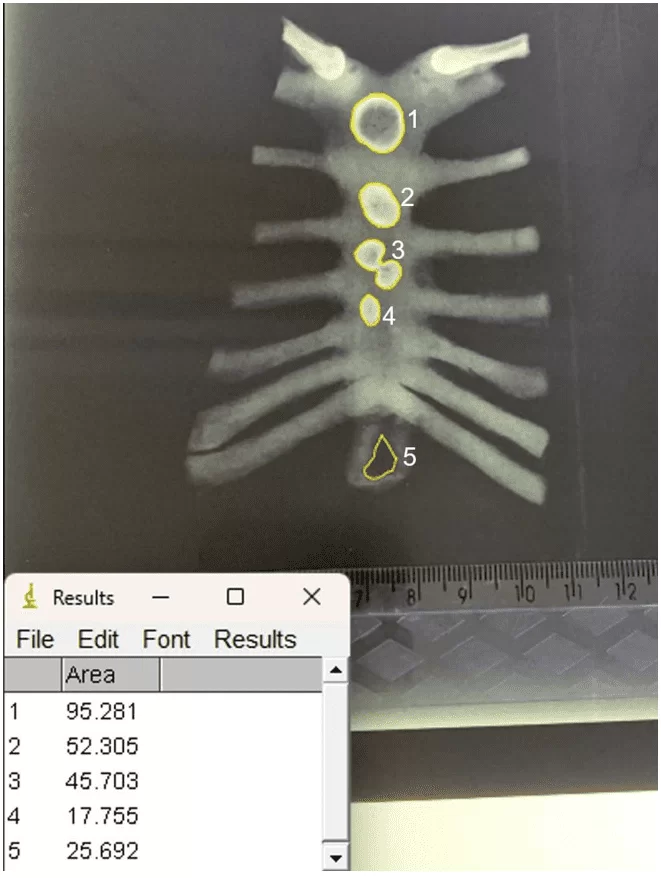
[13] Xiphoid foramen.
Source: Authors (2023).
3. DISCUSSION
The sternum originates from a pair of longitudinal mesenchymal bands, located on both sides of the anterior thoracic wall, which arise during the sixth week of intrauterine life, later grow and migrate medially to meet in the midline where they fuse. This fusion of the sternal bars is completed in the 10th week of intrauterine life, after the fixation of the ribs to form the sternal plate.[11] ,[18], [21]Several ossification centers are present in the sternum, and this progresses in a craniocaudal direction from the third to fourth year of postnatal life and is usually complete by adolescence or adulthood. [11],[18], [20]The ossification of the sternal bone is of the endochondral type, which is regulated from specific ossification centers located in the manubrium (one ossification point) and, in the mesosternum (three ossification points), it is conducted along specific segments in the mesosternum , known as sternebrae, may extend up to 25 years of life.[22]–[24] In the present study, it was possible to observe, through a radiograph of the fetus’ sternum, four ossification points, of which one was in the manubrium and three in the body. It is important to highlight that these findings were not observed in the dissection examination.
Failures in the development process of the fusion lines of multiple ossification centers result in various anomalies of the sternum, such as the formation of foramina or fissures.[11] ,[25], [26]Incomplete fusion of the lower end of the sternum results in a bifid or perforated xiphoid process,[13],[18], [20]which may appear filled with fibroadipose tissue and vessels.[26] In the present case, a fibroadipose tissue was also observed occupying the sternal foramen and/or the bifurcation of the xiphoid process.
The sternal foramen is a developmental defect of the sternum that results in complete perforation of the manubrium, body, or xiphoid process, but mostly appears on the lower part of the sternum. This anatomical variation can be single or multiple in any region along the sternum. (Pasieka et al., 2023). [19]The incidence of sternal foramen in the literature has ranged from 3.1% to 27.4%, while the presence of xiphoid foramen has been reported in up to 57.8% (Table 1).[9],[12],[13],[21],[22],[25]– [36]
Table 1. General occurrence of xiphoid foramen in human adults of both sexes
| Author | Method of study | Single xiphoid foramen % |
| Akin et al.,[13] | Multidetector computed tomography | 34.2 |
| Xie et al.,[36] | Multidetector computed tomography | 57.8 |
| Kuzucuoglu, Albayrak,[37] | Computed tomography | 33.8 |
| Vatzia et al.,[12] | Multidetector computed tomography | 30.7 |
| Pasieka et al.,[19] | Computed tomography and X-rays | 2.9 |
| Ashley,[29] | X rays | 13.3 |
| El-Busaid et al.,[33] | Cadavers | 13.8 |
| Babinski et al.,[20] | Cadavers | 16.7 |
| Xie et al.,[36] | Cadavers | 56.1 |
| Paraskevas et al.,[21] | Cadavers | 18.3 |
| Gkantsinikoudis et al.,[18] | Cadavers | 14.3 |
Source: Authors (2023).
In the present case, a xiphoid foramen was visualized through a radiograph of the sternum of a male fetus. Several authors also observed a higher prevalence of the xiphoid foramen in males,[18]–[20],[35] unlike Paraskevas et al.,[21] who did not observe differences in prevalence between genders.
As the sternum is a bone located anteriorly to several vital structures of the thoracic cage, knowledge about the sternal foramina becomes of great importance to avoid injuries to these structures located in the thorax, with numerous implications, such as traumatic injury to the pleura, heart, in as a result of bone marrow aspiration procedures or acupuncture.[11],[20] Thus, procedures such as acupuncture, bone marrow aspiration and sternal puncture need to be planned in advance with radiological image analysis. Because if a needle is inserted deeply, the pericardium can be injured, which can cause pneumothorax or cardiac tamponade, as well as injury to a vessel within the chest or even to the right ventricle.[12],[18],[20],[21],[26]
The bifurcation of the xiphoid process, the distinction between fracture and variation of the sternum is important in a trauma patient.[16],[30] Anatomical variations can simulate sternal fractures on plain radiography, but ultrasound and computed tomography of the sternum can be used to distinguish anatomical variations from fractures.[39] Therefore, cross-sectional images, such as Computed Tomography and MRI, are often needed to describe the findings detected on radiography and reveal additional small changes.[40]
Sternal variations are common incidental findings on radiographic images, and typical etiologies include suprasternal bones or tubercles, sternal sclerotic band or cleft, foramina, bifid or trifid xiphoid endings, and angulation of the xiphoid process.[9],[41] Anatomical variations of the sternum occur in up to 74% of the population,[12] with sternal foramen occurring in 2.5–13.8%,[17] bifid xiphoid processes in 17.5–32.8% and trifid xiphoid processes in 0.7–4.6% of individuals.[13],[42],[43] Although the presence of sternal variations, with a single xiphoid process, bifid, trifurcate, foramina and absence, rarely present symptoms, are typically occasional findings on radiographic images or autopsy, they have clinical relevance.[13],[16],[17],[21],[33],[41],[44] Reports in the literature have found a variable prevalence of bifid xiphoid processes ranging from 20% to 42.9% (Table 2), while a single xiphoid process was found in 62.6% to 80% of cases.[13],[17],[21],[33],[43],[44]
Table 2. General occurrence of bifid xiphoid process in human adults of both sexes
| Author | Method of study | Bifid xiphoid process % |
| Yekeler et al.,[9] | Multidetector computed tomography | 27.2 |
| Akin et al.,[13] | Computed tomography | 32.8 |
| El-Busaid et al.,[33] | Cadavers | 20.0 |
| Delgado et al.,[45] | Computed tomography | 1.0 |
| Kirum et al.,[44] | Cadavers | 42.9 |
| Turkay et al.,[43] | Computed tomography | 25.0 |
| Ateşoğlu, Deniz, Uslu,[40] | Multidetector computed tomography | 10.5 |
Source: Authors (2023).
Pasieka et al.,[19] performed a meta-analysis with 16,666 patients to study the prevalence of the sternal foramen in the body and in the xiphoid process, as well as to verify its clinical importance. The authors reported that there was a statistically significant improvement in detection of the sternal foramen in cadaveric studies compared with CT and X-ray imaging modalities. However, no statistically significant differences were found between multidetector computed tomography, computed tomography and X-ray studies, as well as between cadaveric and multidetector computed tomography studies. This is probably due to the fact that at autopsies it is possible to visualize small foramina that could possibly not be reliably visualized on multidetector computed tomography, X-rays and computed tomography. Despite there being no statistically significant difference between multidetector computed tomography, computed tomography and X-rays, it has been suggested that healthcare professionals looking to verify the presence of a sternal foramen should use multidetector computed tomography images.[40]
4. CONCLUSION
The present findings show the need for more attention to be given to anatomical variations of the sternum through the use of different methods such as computed tomography, multidetector computed tomography and X-rays. This attention will be important not only for anatomists, but especially for imagenologists, in order to avoid errors in diagnostic analysis.
REFERENCES
[9] YEKELER, E. et al. Frequency of sternal variations and anomalies evaluated by MDCT. AJR Am J Roentgenol, 2006.
[10] SACCHERI, P. et al. A keyhole-shaped sternal defect in an ancient human skeleton. Surg Radiol Anat, 2012.
[11] FOKIN, A. A. Cleft sternum and sternal foramen. Chest Surg Clin N Am, 2000.
[12] VATZIA, K. Frequency of sternal variations and anomalies in living individuals evaluated by MDCT. Eur J Radiol, 2021.
[13] AKIN, K. et al. Anatomic evaluation of the xiphoid process with 64-row multidetector computed tomography. Skeletal Radiol, 2011.
[14] KUMAR, N. S.; BRAVIAN, D.; MORE, A. B. Xiphoid foramen and its clinical implication. Int J Anat Res, 2014.
[15] DURAIKANNU, C.; NORONHA, O. V.; SUNDARRAJAN, P. MDCT evaluation of sternal variations: Pictorial essay. Indian J Radiol Imaging, 2016.
[16] MASHRIQI, F.; D’ANTONI, A. V.; TUBBS, R. S. Xiphoid process variations: a review with an extremely unusual case report. Cureus, 2017.
[17] CHOI, P. J.; IWANAGA, J.; TUBBS, R. S. A comprehensive review of the sternal foramina and its clinical significance. Cureus. 2017.
[18] GKANTSINIKOUDIS, N. et al. Morphological approach of the sternal foramen: an anatomic study and a short review of the literature. Folia Morphol (Warsz), 2017.
[19] PASIEKA, P. et al. Prevalence and morphometry of sternal and xiphoid foramen: a meta-analysis on 16,666 subjects. Surg Radiol Anat, 2023.
[20] BABINSKI, M. A. et al. High prevalence of sternal foramen: quantitative, Anatomical analysis and its clinical implications in acupuncture practice. Int. J. Morphol, 2012.
[21] PARASKEVAS, G. et al. Sternal foramina: incidence in Greek population, anatomy and clinical considerations. Surg Radiol Anat, 2015.
[22] BAYAROĞULLARI, H. et al. Evaluation of the postnatal development of the sternum and sternal variations using multidetector CT. Diagn Interv Radiol, 2014.
[23] WEAVER, A. A. et al. Morphometric analysis of variation in the sternum with sex and age. J Morphol, 2014.
[24] CUBUK, S.; HAMCAN, S. Anatomic variations of sternum may mimic traumatic complications. Am J Emerg Med, 2016.
[25] MOORE, M. K.; STEWART, J. H.; MCCORMICK, W. F. Anomalies of the human chest plate area. Radiographic findings in a large autopsy population. Am J Forensic Med Pathol, 1988.
[26] COOPER, P. D.; STEWART J. H.; MCCORMICK, W. F. Development and morphology of the sternal foramen. Am J Forensic Med Pathol, 1988.
[27] MCCORMICK, W. F. Sternal foramena in man. Am J Forensic Med Pathol, 1981.
[28] STARK, P. Midline sternal foramen: CT demonstration. J Comput Assist Tomogr, 1985.
[29] ASHLEY, G. T. The relationship between the pattern of ossification and the definitive shape of the mesosternum in man. J Anat, 1956.
[30] SCHRATTER, M. et al. Foramensternale: kleine Anomalie—grosse Relevanz [The foramen sternale: a minor anomaly—great relevance]. Rofo, 1997.
[31] AKTAN, A.; SAVAŞ, R. Anatomic and HRCT demonstration of midline sternal foramina. Turk J Med Sci. 1998.
[32] ISHII, S. et al. Causes of photopenic defects in the lower sternum on bone scintigraphy and correlation with multidetector CT. Clin Nucl Med, 2011.
[33] EL-BUSAID, H. et al. Sternal foramina and variant xiphoid morphology in a Kenyan population. Folia Morphol (Warsz), 2012.
[34] SINGH, J.; PATHAK, R. K. Sex and age related non-metric variation of the human sternum in a Northwest Indian postmortem sample: a pilot study. Forensic Sci Int, 2013.
[35] MACALUSO, P. J.; LUCENA, J. Morphological variations of the anterior thoracic skeleton and their forensic significance: radiographic findings in a Spanish autopsy sample. Forensic Sci Int, 2014.
[36] XIE, Y-Z. et al. Morphology of the human xiphoid process: dissection and radiography of cadavers and MDCT of patients. Surg Radiol Anat, 2014.
[37] KUZUCUOGLU, M.; ALBAYRAK, I. Topographic evaluation of sternal foramen patients with thoracic computed tomography. Surg Radiol Anat, 2020.
[38] HUGGETT, J. M.; ROSZLER, M. H. CT findings of sternal fracture. Injury, 1998.
[39] JIN W.; YANG, D. M.; KIM, H. C.; RYU, K. N. Diagnostic values of sonography for assessment of sternal fractures compared with conventional radiography and bone scans. J Ultrasound Med, 2006.
[40] ATEŞOĞLU, S.; DENIZ, M.; USLU, A. I. Evaluation of the morphological characteristic and sex differences of sternum by multi-detector computed tomography. Folia Morphol (Warsz), 2018.
[41] LACHKAR, S.; IWANAGA, J.; TUBBS, R. S. An elongated dorsally curved xiphoid process. Anat Cell Biol, 2019.
[42] BABINSKI, M. A. et al. Frequency of sternal foramen evaluated by MDCT: a minor variation of great relevance. Surg Radiol Anat , 2015.
[43] TURKAY, R. et al. Frequency of sternal variations in living individuals. Surg Radiol Anat, 2017.
[44] KIRUM, G. G. et al. Anatomical variations of the sternal angle and anomalies of adult human sterna from the Galloway osteological collection at Makerere University Anatomy Department. Folia Morphol (Warsz), 2017.
[45] DELGADO, J. et al. Sternal development in the pediatric population: evaluation using computed tomography. Pediatr Radiol, 2014.
[1] Titular Professor of Clinical Anatomy. ORCID: 0000-0002-2300-3330. Currículo Lattes: http://lattes.cnpq.br/6911783083973582.
[2] Medical Student. ORCID: 0009-0002-4983-464X. Currículo Lattes: https://lattes.cnpq.br/2925585130535492.
[3] Medical Student. ORCID: 0000-0002-5298-537X. Currículo Lattes: https://lattes.cnpq.br/4094603011437055.
[4] Medical Clinic Resident. ORCID: 0000-0002-5298-537X. Currículo Lattes: http://lattes.cnpq.br/6291628187714859.
[5] Medical Clinic Resident. ORCID: 0000-0001-9211-7000. Currículo Lattes: http://lattes.cnpq.br/4619345212343744.
[6] Medical Student. ORCID: 0000-0002-1804-5114. Currículo Lattes: http://lattes.cnpq.br/0947941516831134.
[7] Titular Professor of Molecular Biology. ORCID: 0000-0001-5705-6433. Currículo Lattes: http://lattes.cnpq.br/3337321488338686.
[8] Titular Professor of the Medical School. ORCID: 0000-0002-7776-1831. Currículo Lattes: http://lattes.cnpq.br/6858508576490184.
Submitted: April 06, 2023.
Approved: May 10, 2023.















