ORIGINAL ARTICLE
CARVALHO, Simone Meira [1], SOUZA, Karine Soriana Silva de [2], FERREIRA, Mariana Barbosa Leite Sérgio [3], SANTOS, Maíra Aparecida dos [4], BITTENCOURT, Jaqueline Ferreira Ventura [5], GRINCENKOV, Fabiane Rossi dos Santos [6]
CARVALHO, Simone Meira. et al. Spirituality/religiosity and support network in the perception of women with breast cancer. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year. 08, Ed. 04, Vol. 03, pp. 61-77. April 2023. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/perception-of-women, DOI: 10.32749/nucleodoconhecimento.com.br/health/perception-of-women
ABSTRACT
The diagnosis of breast cancer triggers an emotional impact, generating a variety of feelings. Spirituality and religiosity and support from family, friends and professionals is fundamental in coping with this period of adversity. The objective of this study was to understand how women’s spirituality and social support network help in coping with the diagnosis of breast cancer. This is a qualitative study, carried out in an oncology hospital, with the participation of forty women with breast cancer. For data collection, semi-structured interviews were applied, analyzed using Content Analysis. The thematic axis “Support” was composed of the categories “Spirituality/Religiosity” and “Social support”. Faced with the discovery of a disease that leads to suffering and death, a support network is needed to cope with cancer. Spiritual support was unanimous and faith favored overcoming the initial impact, infusing strength to face the diagnosis. The family represented a unique support, helping with health care and with words of encouragement. Professional support occurred through guidance, kindness in assistance and motivation. The pandemic has impacted social isolation. However, it brought benefits such as greater contact with the family. To cope with the cancer diagnosis, the women studied had social and spiritual support, through emotional support, material and practical resources, received from family members and significant others. These are strategies that need to be explored by the multidisciplinary team at the time of diagnosis, minimizing the impact and accepting the demands presented by women with breast cancer.
Keywords: Spirituality, Social Support, Breast neoplasm, Women’s health.
1. INTRODUCTION
The discovery of breast cancer affects women’s lives, triggering an emotional impact, permeating various feelings (KUGBEY; ASANTE; MEYER-WEITZ, 2020), from perplexity, stress, anguish and insecurity (AHMED; ELGHOBASHY; IBRAHIM, 2022). After the diagnosis, myths related to death are awakened, giving rise to feelings of denial and suffering (LOPES; CAMARGO; MAIA, 2020; ALVES et al., 2021).
In the meantime, women need support from family and friends, while they seek to understand the illness and face the treatment. Social support brings benefits in coping with illnesses and promoting health (LOPES; CAMARGO; MAIA, 2020; KUGBEY; ASANTE; MEYER-WEITZ, 2020). Religiosity and Spirituality (R/S) also act as support and motivation factors to help in understanding and coping with the disease (ARAB et al., 2016; AHMED; ELGHOBASHY; IBRAHIM, 2022). Likewise, adequate professional monitoring is necessary, covering the physical, psychosocial and cultural aspects of the illness process (SILVA et al., 2020)
The support network for women has been highlighted as an integral part of breast cancer treatment, providing support, comfort and collaborating in the various dimensions of their lives that are drastically impacted by the diagnosis (LOPES; CAMARGO; MAIA, 2020; ADAM; KORANTENG, 2020). This support network is made up of family, friends and health professionals and works as emotional support or through information, significantly reducing the stress resulting from the diagnosis of breast cancer and increasing emotional well-being (ADAM; KORANTENG, 2020).
For Lopes, Camargo and Maia (2020), spiritual support, arising from religious affiliations or from faith itself, instills strength and support in situations of adversity, favoring acceptance and the process of coping with the disease. Although authors recognize the importance of R/S as a source of support in coping with breast cancer, in Brazil there is still a low scientific production on the subject (ARAB et al., 2016; ALVES et al., 2021).
This research aims to collaborate with health professionals in understanding the factors that help to cope with breast cancer to serve as a tool to improve clinical practice. In this context, the aim was to apprehend how R/S and the social support network of women affected by breast cancer help in coping with the diagnosis.
2. DEVELOPMENT
2.1 METHODS
A descriptive exploratory study, with a qualitative approach, was carried out in an oncological hospital, in Juiz de Fora, Minas Gerais, addressing 40 women with breast cancer, to understand how the spirituality and social support network of women affected by breast cancer help in coping with the diagnosis of the disease. The presentation of the study was guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
2.1.1 SAMPLING AND SAMPLE
The intentionality sample consisted of women diagnosed with breast cancer undergoing chemotherapy at the referred hospital. To enter the study, inclusion and exclusion criteria were selected according to Figure 1.
Figure 1. Participant inclusion and exclusion criteria
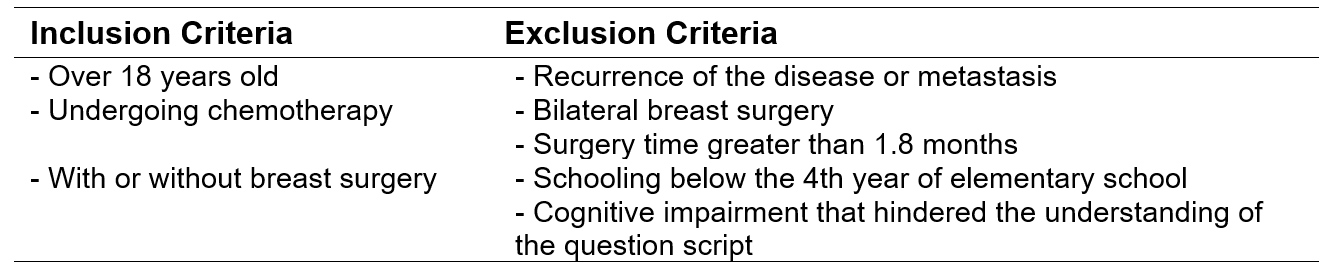
The approach was carried out in the chemotherapy sector. As there was no previous contact with patients in the chemotherapy sector, the patients’ records were evaluated and selected according to the research criteria, indicating which women were being treated for breast cancer. Those who fit the criteria were invited to participate in the study, explaining the objectives by reading and clarifying the Term of Free and Informed Consent (TCLE)[7].
2.1.2 DATA COLLECTION
An individual interview with a semi-structured script was used for data collection, containing sociodemographic and clinical data, as well as questions about the discovery of cancer, treatments and self-care guidelines. The script was appreciated by health professionals and tested by a pilot project. The interviews lasted 20 minutes on average. They were recorded, transcribed and reviewed by the main researcher, who has experience in qualitative health research. Collection was carried out from January 2020 to February 2021, with an interruption between March and October 2020, due to the pandemic. The saturation criterion was observed through the repetition of reports, totaling 40 interviews.
2.1.3 DATA ANALYSIS
Bardin’s Thematic Content Analysis was used to evaluate the qualitative data. This analysis consists of a set of techniques that aim to analyze and infer about the content of the messages identified in the interviews. To organize the data and define the categories, three stages were followed: the first, pre-analysis, aimed at organizing the transcripts of the interviews, formulating hypotheses through skimming reading and elaborating theme indicators; in the second, exploration of the material, the codification of the registration units and the categorization of the nuclei of meaning were carried out; finally, the treatment and interpretation of the results were carried out. At this stage, the inference and interpretation of the results were carried out, seeking a basis in theory to understand the meaning of the messages (BARDIN, 2016).
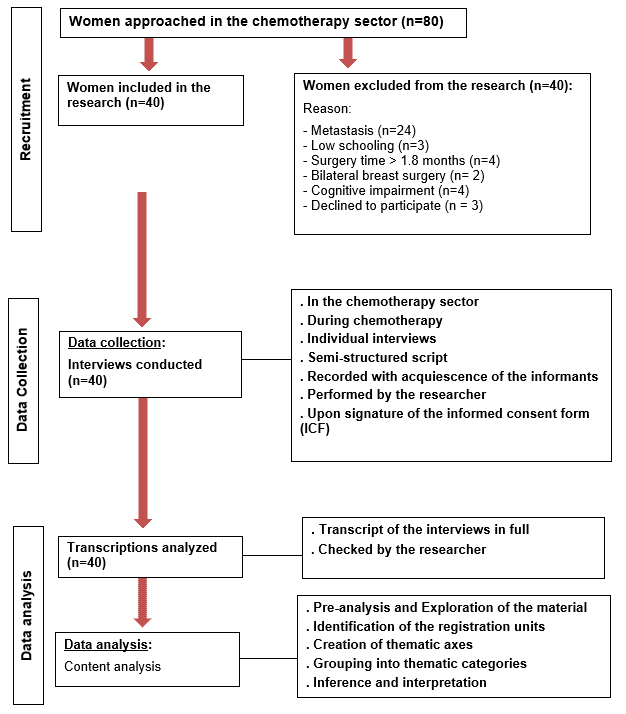
The medical records were accessed to complement the participants’ data. All data collection, analysis and categorization was performed by the main researcher, using the conventional manual method. The final themes were discussed with the other authors. Quotes from interviews were used to represent each category. The stages of recruitment, data collection and analysis are shown in Figure 2.
Figure 2. Data collection and analysis flowchart diagram
2.1.4 ETHICAL ASPECTS
This article is part of an ongoing doctoral research. The study was approved by the Research Ethics Committee of the Universidade Federal de Juiz de Fora (CAAE 16104219.8.0000.5147, version 3, opinion nº 3.649.430), on 10/18/2019. Ethical aspects were observed in the study procedures, according to Resolution No. 466, of December 12, 2012, of the National Health Council/Ministry of Health. The interviewees were identified by the letter E, followed by Arabic numerals, aiming at privacy.
2.2 RESULTS
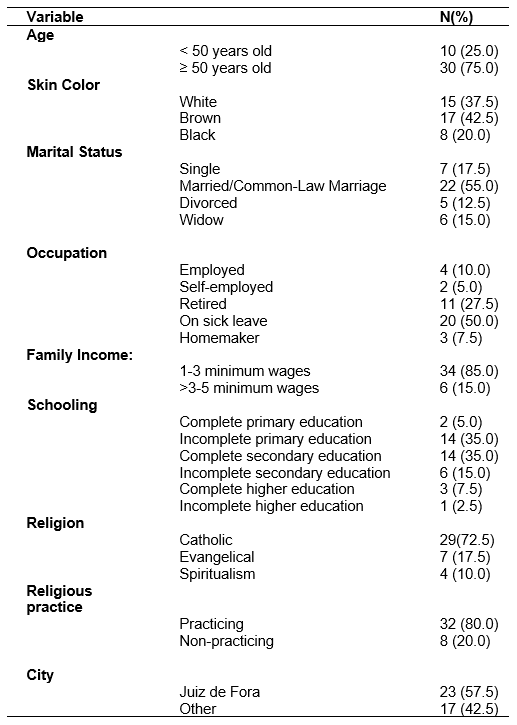
The participants’ age range ranged from 31 to 77 years, with a predominance of brown color/race (42.5%), incomplete elementary school level (35.0%) and complete secondary school (35.0%), and half on sick leave (50%). Most of the women were married (37.5%) and had a family composition of three people (37.5%). There was a prevalence of the Catholic religion (72.5%). The other data are presented in Table 1.
Table 1. Sociodemographic characteristics (n=40)
The analysis of the content of the interviews led to the emergence of registration units, which gave rise to the thematic axis “Support”, from which the thematic categories “Spirituality/Religiosity” and “Social Support” emerged, expressed below.
2.2.1 SPIRITUALITY/RELIGIOSITY
The support found in spirituality and religiosity was cited by all women in the present study. Faith contributed to overcoming the impact of the diagnosis, favoring acceptance and inspiring them to face a disease shrouded in myths, through the courage and strength found in faith.
A minha fé, crer em Deus. Ele quem está me ajudando muito. Se não fosse isso, a gente acaba caindo em depressão, porque enfrentar essa doença não é fácil (…) (E30).
É Deus mesmo que está me ajudando. Porque, eu não esperava ser tão forte assim. A fé em Deus me dá forças (E16).
Faced with illness, women find comfort in faith, which instills hope at a time when negative emotions arise. E/R is an important tool that helps in a positive coping process.
O médico falou (…): “tem gente que chega aqui já desespera, fala que já vai comprar o caixão, chora muito”. Eu não, não me desesperei por nada. (…) Entrego tudo na mão de Deus (E29).
Depois que eu descobri esse diagnóstico, Deus foi colocando um refrigério na minha alma: “vai dar tudo certo” (E31).
All interviewees consider S/R, as they say, “God”, as a primary source of support, coming before the social support of family, friends and health professionals.
Primeiro lugar é Deus. Tenho recebido muito apoio da minha família também e de vizinhos. Até as pessoas daqui mesmo [do hospital] (E12).
Primeiramente é Deus, que dá força à gente. Aí depois tem os médicos e os familiares da gente (E15).
The COVID-19 pandemic presented itself as a barrier to the maintenance of community religious activities. However, the flexibility offered by electronic media facilitated virtual participation.
Meu primo queria ir lá em casa. Tem que ir mais uns dois servos para fazer oração. Mas com a pandemia, não deu (E30).
Me apeguei muito a Ele [Deus]. (…) Agora, não vou mais à missa por causa da pandemia. Mas eu faço muita oração, assisto missas “on-line” e estou rezando muito terço. E tem me ajudado bastante (E13).
Attributing meaning to suffering reinforces women’s self-esteem. Even in a difficult situation, they find vigor in the search for treatment of the disease and infect those around them.
Minha sobrinha vai à minha casa e fala que eu passo muita alegria, mesmo enfrentando esse problema. Ela fala que vai me visitar e sai feliz, porque eu passo força para ela (E34).
Eu gosto de viver. Porque a gente tem que se gostar, querer estar bem […] para poder continuar. Se não estivermos bem, não têm como ajudar ninguém, não tem como fazer nada (E35).
2.2.2 SOCIAL SUPPORT
The family proved to be an important source of support for all research participants. Through assistance in health care, affection and words of encouragement, the support of this support network alleviates suffering and is the driving force to endure treatments and fight for life.
Uma coisa importante, que ameniza demais, é o carinho dos familiares, o amor e o cuidado (E7).
Uma [irmã] em especial, que sempre esteve comigo em todos os momentos, é a minha fortaleza. A família, amigos, me ajudaram muito (E37).
However, social support can also be perceived negatively. This perception may be influenced by several factors, mainly the difficulty in dealing with the illness of a family member.
Minha família é maravilhosa, só que eles não me acompanham de perto. Eles lá e eu aqui (E25).
Depois que descobri esse câncer (…). Faz diferença sim, tem a carência. O apoio não é só pagar as contas, mas tem o apoio de mais presença. Isso eu sinto falta (E26).
Regarding social support from family and friends, geographic distance and the need for isolation due to the pandemic were critical obstacles, due to the need for social isolation to avoid contamination by the coronavirus. In the midst of these barriers, family members sought ways to overcome the distance, playing an important role in supporting women.
Às vezes a pessoa tem até vontade de ir fazer uma visita, mas fica com medo por conta da pandemia, devido à possibilidade de eu pegar [coronavírus] (E33).
Minha filha que mora na Inglaterra, ela soube [do câncer]: “nem que eu tenha que ir comprar a passagem no cartão, vou dar um jeito de ir ver minha mãezinha” (E21).
On the other hand, the pandemic also brought closer family relationships, due to the interruption of work and student activities, in addition to the removal of women from their activities due to the treatment.
Minha filha estava com cinco meses e eu continuei trabalhando. Agora, com esse negócio de pandemia, que descobri o câncer, que eu estou ficando mais em casa com ela (E28).
Por causa da pandemia, não está tendo aula, então, ele [filho] fica do meu lado. Tudo que eu falo, ele me dá atenção (E35).
The support network of the women in the present study was constituted, in addition to the family, by friends, neighbors, co-workers and people from social life. This network works as support in a moment of fragility.
Tenho muitas amigas da igreja. Elas vão me visitar! Minha casinha tem dias que fica cheia (risos) (E6).
Minha amiga de infância. (…) a mãe dela teve câncer e faleceu no ano passado. Mesmo com esse período difícil, ela tem me apoiado muito (E7).
Electronic media played an important role in overcoming the barriers of distancing, especially in the pandemic period, highlighting benefits such as approximation, strengthening of bonds and the courage to face the illness.
Minha mãe me dá suporte em palavras, (…) pelo “whatsapp”. As palavras e o carinho das pessoas me deixam animada (E11).
Entrei agora em um grupo [da igreja], pelo celular. Estou seguindo e tem me ajudado bastante (E23).
Another source of support was that of health professionals, identified through attention, affection, good service, enlightening approach. The participants reported that these characteristics brought benefits such as safety and motivation.
Estou sendo bem tratada, seja pelos enfermeiros, os médicos e as meninas da recepção, todos são agradáveis, tratam a gente com carinho (E11).
O tratamento aqui [no hospital] é muito bom, o pessoal [profissionais de saúde], são todos muito bons, explicam tudo direitinho. Isso é muito importante (E25).
In the interviews, it was noticed that few participants received assistance from other professionals, including the importance of the psychologist. Only five women had contact with this professional.
Como te falei antes, o psicológico é muito importante (E7).
E a questão psicológica, na qual eu recorri ajuda. Às vezes precisamos conversar sobre essa questão [câncer]. Porque, tem dias que você só quer chorar, chorar, no outro dia você fica bem (E37).
2.3 DISCUSSION
Faced with the peculiarities of illness from cancer and the beliefs that trigger significant changes in lifestyle, the possibility of death and reflections on the meaning of life, R/S is a powerful tool in the coping process (SILVA et al., 2020; AHMED; ELGHOBASHY; IBRAHIM, 2022). In the research, R/S was present in the experience of all participants. Other research has shown that women used R/S to better cope with the illness (VARGAS et al., 2020).
By bringing with it feelings, decisions and deep reflections, adversities favor the pursuit of R/S, which becomes intensified in those moments when human beings are faced with their fragility (ALVES et al., 2021; SILVA et al., 2020 ; AHMED; ELGHOBASHY; IBRAHIM, 2022). In the present study, women sought relief, comfort and strength in their attachment to God, which helped in the acceptance process, minimizing negative impacts (FERREIRA et al., 2020; ALVES et al., 2021).
It was verified that the R/S contributed to the experience in the community of faith, which instills a hopeful look at the illness situation, corroborating other studies, which claim that women see God as someone who relieves suffering (BORGES; ANJOS; CAMPOS, 2021; FERREIRA et al., 2020; VARGAS et al., 2020).
Another factor highlighted in the present study was the emergence of reflections on life, its meaning and way of living it. The attribution of a new meaning to suffering was also present, allowing the establishment of priorities and future goals (MOKHTARI et al., 2021; AHMED; ELGHOBASHY; IBRAHIM, 2022).
With regard to social support, women perceived support from family and friends, manifested in the form of material resources, advice and affection, as a source of protection and strength to face adversity, a fact also verified by other authors (ADAM; KORANTENG, 2020 ; ARAB et al., 2016). Families are the closest support system, establishing themselves as an important factor in coping with and managing the disease (VARGAS et al., 2020; MOKHTARI; MARKANI; KHALKHALI, 2021).
On the other hand, situations were observed in which the woman does not perceive herself to be met in some need, such as, for example, the emotional one due to distancing. It is noteworthy that the family is also impacted, experiencing feelings of concern, fragility and uncertainty, which negatively influence relationships (FIGUEIREDO et al., 2017). Thus, it is relevant to include the family in the treatment, preparing them for the care and support of women diagnosed with cancer (LOPES; CAMARGO; MAIA, 2020).
Due to the need for social isolation, the pandemic triggered socioeconomic impacts on physical and mental health and, consequently, on quality of life (MASSICOTE; IVERS; SAVARD, 2021), especially in cancer patients, who are already dealing with physical and mental changes resulting from the treatment (MARÇAL; VAZ, 2022). In addition to the concern with the prognosis, social distancing impaired the functioning of the support network, imposing difficulties in contact with family and friends (CORRÊA; OLIVEIRA; TAETS, 2020). On the other hand, there were positive points brought by the “lockdown”, considering that a greater availability of time allowed the approximation of some family ties.
The support of health professionals is also of great importance for coping with cancer (MOKHTARI et al., 2021), whether emotional or informative. The present study showed that both provide greater emotional stability and knowledge about the treatment (ADAM; KORANTENG, 2020). In the present research, few women had contact with the psychologist. In the meantime, it is essential to highlight the importance of comprehensive care for women with cancer, covering not only physical aspects, but also social, psychological and spiritual aspects (LOPES; CAMARGO; MAIA, 2020).
3. FINAL CONSIDERATIONS
Faced with the repercussions of the diagnosis of breast cancer on women’s lives, R/S has been a priority coping resource, helping in the process of accepting the diagnosis. It also contributes to social support by providing community experience.
Faced with the emergence of reflections related to the meaning of life and the way of living it, the R/S helped in attributing new meanings to the suffering experienced. The social support received from family and friends, as well as the emotional and informational support received from health professionals, played an important role. Such coping mechanisms become preventive and health-promoting strategies that should be explored by the multidisciplinary team, aiming to minimize the emotional impact of the diagnosis of women affected by breast cancer.
3.1 LIMITATIONS
The study had limitations regarding the sample recruitment method. Choosing for convenience can bring with it possible selection biases. As it is restricted to only one cancer hospital, it does not allow the results to be generalized to the population of patients studied. As for the number of participants, research with a qualitative approach covers a limited number of interviews, since the understanding of a phenomenon or event does not need to be quantified. However, the depth of this data collection instrument is usually sufficient to achieve the proposed objectives. It is also necessary to demarcate that the results found by the qualitative study are not subject to statistical generalizations, but naturalistic ones. The cross-section used prevents the evaluation of the impacts of the event under study in the long term.
3.2 FUTURE COLLABORATIONS
This research offers the possibility of future studies that deeply investigate R/S and social support in women at the time of diagnosis, such as the effects of these experiences, in the long term, on the socio-emotional impacts of the news of the diagnosis.
Some repercussions of the COVID-19 pandemic were seen in the experience of the investigated resources. Thus, follow-up studies are needed to investigate the greater repercussions of this event on the use of these coping resources.
In view of the role assumed by R/S and social support in coping with women at the time of diagnosis, it is extremely important that the health team uses such resources in a preventive and promoting way, developing an integral work to address the biopsychosocial aspects -spiritual, also envisioning the family, caregivers and other sources of support. For this, the presence of a multidisciplinary team, capable of providing support to women, is of paramount importance. Emotional support is not restricted to psychology professionals, since all professionals must use strategies for this immediate support.
REFERENCES
ADAM, Awolu; KORANTEN, Felix. Availability, accessibility, and impact of social support on breast cancer treatment among breast cancer patients in Kumasi, Ghana: A qualitative study. PLoS ONE, v. 15, n. 4, p. e0231691m, 2020. PMCID: PMC7162460. DOI: https://doi.org/10.1371/journal.pone.0231691. Acesso em: 05 jan. 2023.
ALVES, Débora Pimenta; PEREIRA, Laura Costa; ALVES, Calima Sousa Bragunce; GOMES, Laiza Bonela. Spirituality and its reflections in oncological patients. Health & Society, v. 1, n. 4, p. 37-69. 2021. ISSN: 2763-5724. DOI: https://doi.org/10.51249/hes01.04.2021.360. Acesso em: 05 jan. 2023.
AHMED, Marwa Mohammad; ELGHOBASHY, Soheir Fahim; IRBAHIM, Noha Yahya. Seeking social support and religious spiritual predictors of posttraumatic growth câncer survivors. American Journal of Applies Psychology, v. 11, n. 5, p. 133-141, 2022. DOI: https://doi.org/10.11648/j.ajap.20221105.12. Disponível em: https://www.sciencepublishinggroup.com/j/ajap. Acesso em: 05 jan. 2023.
ARAB, Cláudia; CORREIA, Clara Knierim; DEMONICO, Bruna Belusse; VILARINO, Guilherme Torres; ANDRADE, Alexandro. Câncer de mama e reações emocionais: revisão sistemática. Revista Baiana de Saúde Pública, v. 40, n. 4, p. 968-009, 2016. DOI: https://doi.org/10.22278/2318-2660.2016. Acesso em: 05 jan. 2023.
BARDIN, Laurence. Análise de conteúdo. São Paulo: Edição 70, 2016.
BORGES, Marcela Guaritá; ANJOS, Anna Cláudia Yokoyama dos; CAMPOS, Cristiane Soares. Espiritualidade e religiosidade como estratégias de enfrentamento do câncer de mama: revisão integrativa da literatura. Brazilian Journal of Health Review, v. 4, n. 1, p. 1002-1021, 2021. DOI: https://doi.org/10.34119/bjhrv4n1-088. Acesso em: 05 jan. 2023.
CORRÊA, Karine Marques; OLIVEIRA, Júlia Damasceno Borges; TAETS, Gunnar Glauco de Cunto Carelli. Impacto na qualidade de vida de pacientes com câncer em meio à pandemia de COVID-19: uma reflexão a partir da Teoria das Necessidades Humanas Básicas de Abraham Maslow. Revista Brasileira de Cancerologia, v. 66, n. 1, p. 1-5:e-1068, 2020. DOI: https://doi.org/10.32635/2176-9745.RBC.2020v66nTemaAtual.1068. Acesso em: 05 jan. 2023.
FERREIRA, Laura Fernandes; FREIRE, Alyssa de Pinho; SILVEIRA, Ana Luiza Cunha; SILVA, Anthony Pereira Martins; SOUZA, Hermo Igor Soares; GARCIA, Lohane Stefany Araújo; PERALTA, Rafael Silva; ARAÚJO, Laís Moreira Borges. A influência da espiritualidade e da religiosidade na aceitação da doença e no tratamento de pacientes oncológicos: revisão integrativa da literatura. Revista Brasileira de Cancerologia, v. 66, n. 2, p. 1-13, 2020. DOI: https://doi.org/10.32635/2176-9745.RBC.2020v66n2.422. Acesso em: 05 jan. 2023.
FIGUEIREDO, Tamara; SILVA, Andréia Pereira da; SILVA, Rita Mânia Rosa; SILVA, Juliana de Jesus; SILVA, Carla Silvana de Oliveira e; ALCÂNTARA, Deivite Danilo Ferreira; SOUZA, Luís Paulo Souza e; SOUZA, Ana Augusta Maciel de. Como posso ajudar? Sentimentos e experiências do familiar cuidador de pacientes oncológicos. ABCS Health Science, v. 42, n. 1, p. 34-39, 2017. DOI: http://dx.doi.org/10.7322/abcshs.v42i1.947. Acesso em: 05 jan. 2023.
KUGBEY, Nuworza; ASANTE, Kwaku Oppong; MEYER-WEITZ, Anna. Depression, anxiety and quality of life among women living whith breast cancer in Ghana: mediating roles of social support and religiosity. Supportive Care in Cancer, v. 28, n. 6, p. 2581-2588, 2020. DOI: https://doi.org/10.1007/s00520-019-05027-1. Disponível em: https://pubmed.ncbi.nlm.nih.gov/31520120/. Acesso em: 11 jan. 2023.
LOPES, Ana Paula; CAMARGO, Carmem Aparecida Cardoso Maia; MAIA, Maria Ambrosina Cardoso. Sofrimento psíquico vivenciado por mulheres diante do diagnóstico de câncer de mama: uma revisão bibliográfica reflexiva. Revista Eletrônica Acervo Saúde, v. 52, n. 52, p. 1-7, 2020. DOI: https://doi.org/10.25248/reas.e3556.2020. Disponível em: https://acervomais.com.br/index.php/saude/article/view/3556. Acesso em: 21 dez. 2022.
MARÇAL, Ruan Thompson de Souza; VAZ, Camila Teixeira. Treatment of breast cancer in the time of COVID-19: an integrative review. Research, Society and Development, v. 11, n. 10, p. 3-13:e252111032915, 2022. DOI: https://doi.org/10.33448/rsd-v11i10.32915. Disponível em: https://rsdjournal.org/index.php/rsd/article/view/32915. Acesso em: 16 dez. 2022.
MASSICOTE, Véronique; IVERS, Hans; SAVARD, Josée. COVID-19 Pandemic stressors and psychological symptoms in breast cancer patients. Current Oncology, v. 28, n. 1, p. 294-300, 2021. DOI: https://doi.org/10.3390/curroncol28010034. Acesso em: 05 jan. 2023.
MOKHTARI, Leila; MARKANI, Abdollah Khorami; KHALKHALI, Hamid Reza; FEIZI, Aram. The perceveid social support by Iranian women with breast cancer: a qualitative study. Supportive Care in Cancer, v. 30, n. 1, p. 941-949, 2021. DOI: https://doi.org/10.1007/s00520-021-06478-1. Acesso em: 05 jan. 2023.
SILVA, Karline Kelly da; BARRETO, Francisca Adriana; CARVALHO, Francisca Patrícia Barreto de; CARVALHO, Pablo Ramon da Silva. Estratégias de enfrentamento após o diagnóstico de câncer de mama. Revista Brasileira em Promoção da Saúde, v. 33, p. 1-10, 2020. DOI: https://doi.org/10.5020/18061230.2020.10022. Acesso em: 05 jan. 2023.
VARGAS, Gabriela de Souza; FERREIRA, Carla Lizandra de Lima; VACHT, Crischima Lunardi; DORNELLES, Carla da Silveira; SILVEIRA, Vanessa do Nascimento; PEREIRA Adriana Dall”Asta. Social support network of women with breast cancer. Revista de Pesquisa Cuidado é Fundamental Online, v. 12, p. 73-78, 2020. DOI: http://dx.doi.org/10.9789/2175-5361.rpcfo.v12.7030. Disponível em: http://seer.unirio.br/cuidadofundamental/article/view/7030. Acesso em: 16 fev. 2023.
APPENDIX – FOOTNOTE
7. Termo de Consentimento Livre e Esclarecido (TCLE).
[1] Doctoral student in the Graduate Program in Psychology at the Universidade Federal de Juiz de Fora (graduate in progress); Juiz de Fora (MG), Brazil. Master in Collective Health, by the Universidade Federal do Rio de Janeiro; Juiz de Fora (MG), Brazil. Graduated in Physiotherapy, by Centro Universitário Metodista do Instituto Porto Alegre (1987); Porto Alegre (RS), Brazil. ORCID: 0000-0002-7680-131X. Currículo Lattes: http://lattes.cnpq.br/2502447838688845.
[2] Specialist in Adult Health, with Emphasis in Chronic-Degenerative Diseases, by the Programa de Residência Multiprofissional do Hospital Universitário da Universidade Federal de Juiz de Fora (HU/UFJF). Graduated in Psychology, by the Institute of Human Sciences of the Universidade Federal de Juiz de Fora; Juiz de Fora (MG), Brazil. ORCID: 0000-0003-3763-6478. Currículo Lattes: http://lattes.cnpq.br/3483394631182991.
[3] Master in Psychology, from the Universidade Federal de Juiz de Fora; Juiz de Fora (MG), Brazil. Specialist in Cognitive-Behavioral Therapy, by Faculdade Redentor. Graduated in Psychology, from the Centro de Ensino Superior de Juiz de Fora Juiz de Fora (MG), Brazil. ORCID: 0000-0001-6819-6482. Currículo Lattes: http://lattes.cnpq.br/1343124968034583.
[4] Undergraduate student in Psychology at the Institute of Human Sciences at the Universidade Federal de Juiz de Fora; Juiz de Fora (MG), Brazil. ORCID: 0009-0000-8439-4024. Currículo Lattes: https://lattes.cnpq.br/9465882716674784.
[5] PhD in Nursing from the Anna Nery School of Nursing at the Universidade Federal do Rio de Janeiro (UFRJ). Master in Nursing from the School of Nursing of the Universidade Federal de Minas Gerais (UFMG). Specialization (lato sensu post-graduation) in Occupational Nursing, by the Faculdade de Enfermagem Luiza de Marillac – Centro São Camilo de Desenvolvimento em Administração da Saúde (CEDAS). Degree in Nursing and Midwifery from the Universidade Federal de Juiz de Fora; Juiz de Fora (MG), Brazil. ORCID: 0000-0001-9395-4388. Currículo Lattes: http://lattes.cnpq.br/8032123272413172.
[6] Advisor. Doctor in Health, from the Universidade Federal de Juiz de Fora; Juiz de Fora (MG), Brazil. Master in Health, Universidade Federal de Juiz de Fora; Juiz de Fora (MG), Brazil. Degree in Psychology, from the Higher Education Center of Juiz de Fora; Juiz de Fora (MG), Brazil. ORCID: 0000-0003-0948-2635. Currículo Lattes: http://lattes.cnpq.br/0976974025888018.
Submitted: February 9, 2023.
Approved: April 06, 2023.















