ORIGINAL ARTICLE
ARAGÃO, José Aderval [1], ARAGÃO, Iapunira Catarina Sant’Anna [2], ARAGÃO, Felipe Matheus Sant’Anna [3], LOURENÇO, Bárbara Costa [4], KUHN, Caio Siqueira [5], MUNARETTO, Giovanna Freitas [6], GUERRA, Danilo Ribeiro [7], FEITOSA, Vera Lúcia Correa [8], REIS, Francisco Prado [9]
ARAGÃO, José Aderval. et al. The anatomical position of the vermiform appendix and its morphometry in relation to the extension of the mesoappendix: a study on fresh cadavers. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year. 08, Ed. 04, Vol. 06, pp. 133-144. April 2023. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/vermiform-appendix, DOI: 10.32749/nucleodoconhecimento.com.br/health/vermiform-appendix
ABSTRACT
Introduction: the Vermiform Appendix (VA) is a highly variable organ, being an enigma for the surgeon regarding its position, size and symptomatology. Rapid and accurate diagnosis for adequate treatment of acute appendicitis not only depends on the symptoms, but also on the knowledge of variations in its anatomical position. Objective: to determine the occurrence of the anatomical position of the VA in fresh cadavers, its relationship with the mesoappendix and morphometry. Material and method: the Vermiform Appendages (VAs) of 50 fresh cadavers were examined, the morphological aspects and morphometry of the VAs were studied, such as: position, length and diameter of the appendix, in addition to the length of the mesoappendix and whether it occupied the entire length of the appendix length. Morphometric data were performed with a digital caliper with a precision of 0.01 mm. Result: of the 50 cadavers autopsied during the study, 44 (88%) were male and six (12%) were female. Age ranged from 14 to 80 years, with an average of 36.8 years. Regarding the biotype, 44% (22) were athletic, 32% (16) leptosomic and 24% (12) pycnic. The VA was located in six different positions, with the pelvic and retrocecal positions being the most prevalent. The mesoappendix occupied, in 92% of the cases, the entire length of the VA. Conclusion: the most frequent position of the VA was the pelvic type. Knowledge about the anatomical position of the appendix and the complete mesoappendix in the population can contribute significantly to improving the early clinical diagnosis of appendicitis and, consequently, reducing morbidity.
Keywords: Vermiform appendix, Mesoappendix, Appendectomy, Appendicular artery, Variation.
INTRODUCTION
The Vermiform Appendix (VA) is a cylindrical, thin and curved organ located in the lower right quadrant of the abdomen (CHAN et al., 2002; GOLALIPOUR et al., 2003). It is a blind diverticulum of the intestine that, after birth, undergoes rotation due to the differential growth of the cecum (WAKELEY, 1933, AJMANI; AJMANI, 1983; MALAS; GÖKÇIMEN; SULAK, 2001). Its point of union with the cecum is approximately 2.5 cm below the ileocecal valve, in the coalescence of the three intestinal tapeworms, an important landmark to find it during surgical interventions (AJMANI; AJMANI, 1983; MALAS et al., 2004). Although its implantation is considered a consistent point, the location of the other parts of the appendix varies considerably (CHAN et al., 2002; WAKELEY, 1933).
The location of the appendix is influenced by changes in the position and shape of the cecum during development, with the base of the appendix basically fixed and its apex able to assume different positions (BIRNBAUM; WILSON, 2000; EL-MASRY; THEODOROU, 2002). The main known positions are: retrocecal, pelvic, pre-ileal, post-ileal, retrocolic, subcecal and paracecal 2001; MALAS et al., 2004). The vermiform appendix has a large number of lymph nodes aggregated in its walls and is suspended from the terminal portion of the ileum by the mesoappendix, which contains the appendicular vessels (JONES; KAYE, 1972; OUATTARA et al., 2007; SWATHIPRIYADARSHINI et al., 2022) .
Researches have revealed that the frequency of anatomical characteristics of the vermiform appendix vary between different ethnic groups and that these interfere in the signs and clinical diagnosis of acute appendicitis (CHAN et al., 2002). One in every 15 people will have acute appendicitis at some point in their lives, and its mortality ranges from 1 to 5.6% (BHANGU et al., 2015; WILLIAMS et al., 2021). Therefore, knowledge about an anatomical pattern of the reference site for the position of the vermiform appendix may be important for the diagnosis of acute appendicitis. The aim of the present study was to determine the occurrence of anatomical position of the VA, as well as its relationship with the mesoappendix and morphometry.
During the performance of necropsies at the Instituto Médico Legal “Dr. Augusto Leite” in the State of Sergipe, the Vermiform Appendages (VAs) of 50 fresh cadavers were examined from October 2018 to February 2019. A xyphopubic incision of the abdominal cavity was performed by the medical examiner, allowing the VAs and their mesoappendices to be exposed. The identification of the position of the appendices was carried out by a team of duly prepared researchers, which consisted of physicians, anatomists and medical students.
The appendices that were in good condition were included in the study, and those vermiform appendages of decomposed bodies and in cases of lacerated lesions involving the appendix or its adjacent structures were excluded. The morphological aspects and morphometry of the VAs were studied, such as: position, length and diameter of the appendix, in addition to the length of the mesoappendix and whether it occupied the entire length of the appendix. Descriptive statistics was performed with taking the percentage and mean. To assess the degree of relationship between the appendix position, mesoappendix and biotype variables, as well as height, appendix diameter, mesoappendix length and biotype, Pearson’s correlation coefficient (Pearson’s r) was applied, which has the function of measuring the intensity and direction between two linear variables. The study was approved by the Ethics and Research Committee of the Universidade Federal de Sergipe CAAE: 03863612.7.0000.0058.
Morphometric data were performed with a digital caliper with a precision o
f 0.01 mm.
RESULTS
Of the 50 cadavers autopsied during the study, 44 (88%) were male and six (12%) were female. Age ranged from 14 to 80 years, with an average of 36.8 years. Height ranged from 1.49 cm to 1.84 cm, with an average of 1.66 cm. Regarding the biotype, 44% (22) were athletic, 32% (16) leptosomic and 24% (12) pycnic.
The VA was located in six different positions, with emphasis on the pelvic (Figure 1) and retrocecal (Figure 2) positions, which were the most prevalent (Table 1). In 92% (46) of the cases, the mesoappendix occupied the entire length of the VA (Figure 3). There was no association between the VA position and the presence of a mesoappendix (p = 0.449) or with the individuals’ biotypes (p = 0.799).
There was a weak and non-significant correlation between subjects’ height and VA diameter (Pearson’s r = 0.181, p = 0.207) and length (Pearson’s r = 0.159, p = 0.271). There was also a weak and non-significant association between the individual’s height and the length of the mesoappendix (Pearson’s r = 0.078, p = 0.591). There was no difference in VA length between subjects’ biotypes (p = 0.694).
Figure 1. Vermiform appendix in pelvic position
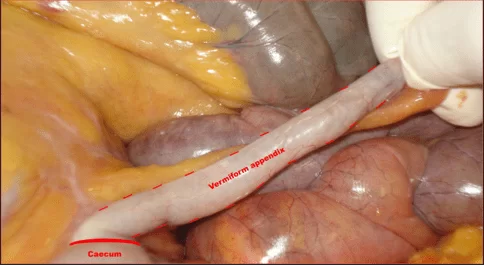
Figure 2. Vermiform appendix in retrocecal position
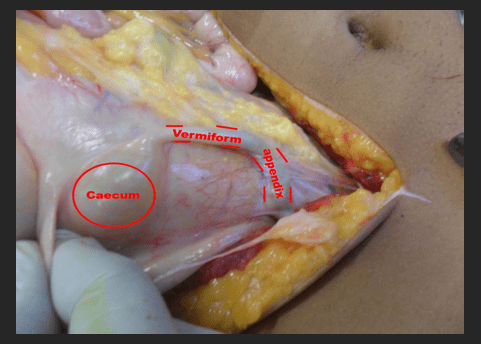
Table 1. Occurrence of the position of the vermiform appendix in fresh cadavers autopsied at the IML[10] of the State of Sergipe
| General position of the vermiform appendix | Occurrence |
| Pelvic | 52% (26) |
| Retrocecal | 22% (11) |
| Subcecal | 10% (5) |
| Pre-ileal | 6% (3) |
| Retrocolic | 6% (3) |
| Post-ileal | 4% (2) |
Source: Authors.
Figure 3. Mesoappendix occupying the entire length of the vermiform appendix
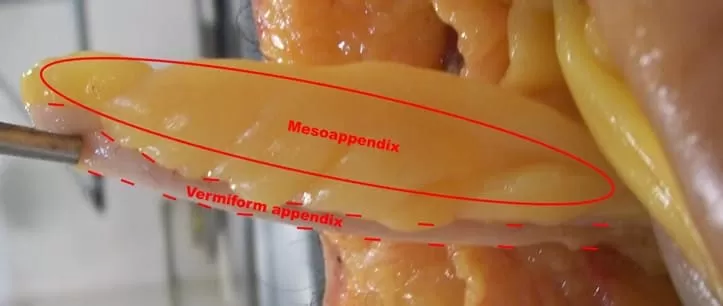
Table 2 shows the morphometric data of the VA and the mesoappendix.
Table 2. Vermiform appendix and mesoappendix morphometry (mm)
| Morphometry | Minimum | Maximum | Average | SD |
| Length of the vermiform appendix | 5.2 | 17.7 | 9.74 | 2.60 |
| Diameter of the vermiform appendix | 0.3 | 0.8 | 0.54 | 0.12 |
| Mesoappendix length | 2.5 | 17.9 | 9.36 | 3,03 |
mm – millimeters
Source: Authors.
DISCUSSION
The VA, in humans, is characterized by its mobility, thus making it an organ of variable position, length and diameter, which can change in various situations (NAYAK, 2010). In the present study, with 52% of the cases, the pelvic position of the VA was the most frequent. Similar findings in fresh and formalinized adult cadavers were reported by Golalipour et al. (2003), Rahman et al. (2006), Ahmed et al. (2007), Tofighi et al. (2013), Ghorbani; Forouzesh; Kazemifar (2014) and Altunkas et al. (2022). Already Wakeley (1933), Shah; Shah (1945), Paul et al. (2009), Bakar et al. (2013), Mwachaka et al. (2014), Souza; Coast; Souza (2015), Mohammadi et al. (2017), Khatun; Thakur; Shah (2019), observed that the most frequent position was retrocecal.
Searle et al. (2013), with the objective of investigating the relationship between length, diameter and age of the appendix, in children under eighteen years of age, to determine whether the appendix changes size with age, showed that, after an initial period of growth, during the Early childhood, until about age 3, the appendix reaches its adult proportions and does not continue to grow during childhood. For Chan et al. (2002) and Verginio et al. (2019), the VA, would vary from 6 cm to 9 cm in length, and would arise from the posteromedial face of the cecum below the ileocecal junction. Other authors admitted for the length of the VA variation from 1 to 20 cm, with an average of 5.43 to 11.4 cm (SOLANKE 1970; NAYAK, 2010; TOFIGHI et al., 2013, BAKAR et al., 2013; MANISHA et al., 2013; GHORBANI; FOROUZESH; KAZEMIFAR, 2014; MWACHAKA et al., 2014; SOUZA; COSTA; SOUZA, 2015; MOHAMMADI et al., 2017). In the present study, an average length of 9.74±2.6 cm was found for the VA (Table 3).
Table 3. VA morphometric data in relation to the literature
| Author | Kind of study | Minimum | Maximum | Average |
| Solanke (1970) | Formaldehyde cadavers | 4 | 20 | 9,6 |
| Nayak (2010) | Cadavers | 2,0 | 20,0 | 9,0 |
| Tofighi et al. (2013) | Fresh cadavers | 1,5 | 17,5 | 8,5 |
| Bakar et al. (2013) | Fresh cadavers | 6,0 | 16,3 | 10,2 |
| Manisha et al. (2013) | Formaldehyde cadavers | 2,0 | 9,0 | 5,43 |
| Ghorbani; Forouzesh; Kazemifar (2014) | Fresh cadavers | 1,5 | 17,5 | 8,5 |
| Mwachaka et al. (2014) | Formaldehyde cadavers | 3,5 | 14,5 | 7,65 |
| Souza; Costa; Souza (2015) | Fresh cadavers | 1,0 | 20,0 | 11,4 |
| Mohammadi et al. (2017) | Fresh cadavers | 0,5 | 16,0 | 8,52 |
| Present study | Fresh cadavers | 5,2 | 17,7 | 9,74 |
Source: Authors.
In similar studies, the VA diameter measured at its base ranged from 1.76 to 8.3 mm, with an average of 0.6 to 5.2 mm (SOLANKE, 1970; BAKAR et al., 2013; MOHAMMADI et al., 2017; ALTUNKAS et al., 2022). In the current study, the average found was 0.54 mm, ranging from 0.3 to 0.8 mm.
Regarding the extension of the mesoappendix, in 92% of the cases, it occupied the entire length of the AV. This finding is close to that reported by Solanke (1970), who found the mesoappendix occupying 88.5% of the VA extension. For Rahman et al. (2009), Golalipour et al. (2003), Tofighi et al. (2013), Bakar et al. (2013) and Ghorbani; Forouzesh; Kazemifar (2014), the extent of occupation of the mesoappendix in relation to the length of the VA ranged from 24 to 79.5% of cases. As VA vascularization follows through the mesoappendix, the reduced length of the mesoappendix extension may hinder vascularization to the end of the organ, which may cause serious implications during the inflammatory process and early perforation.
CONCLUSION
The most frequent position of the VA was the pelvic type. Knowledge about the anatomical position of the appendix and the complete mesoappendix in our population can contribute significantly to improving the early clinical diagnosis of appendicitis and, consequently, reducing morbidity. Like other anatomical variations, the position of the vermiform appendix and the mesoappendix can cause difficulties for surgeons when performing surgical interventions on this organ. The findings of the present study may provide information about the morphological variations of the appendix in the Sergipe population.
ACKNOWLEDGEMENT
The authors of this article thank and pay homage to Professor José Carlos Nunes Mota (in memoriam), not only for the theme of the work, but also for the incentive to carry it out and collect the study material.
REFERENCES
AHMED, I.; et al. The position of the vermiform appendix at laparoscopy. Surg Radiol Anat., vol. 29, n. 2, p. 165-8, 2007.
AJMANI, M. L.; AJMANI, K. The position, length and arterial supply of vermiform appendix. Anat Anz., vol. 153, n. 4, p. 369-74, 1983.
ALTUNKAS, A.; et al. The normal vermiform appendixin adults: Its anatomical location, visualization, and diameter at computed tomography. J Anat Soc India, n. 71, p. 225-33, 2022.
BAKAR, S. M.; et al. Negative correlation between age of subjects and length of the appendix in Bangladeshi males. Arch Med Sci., vol. 9, n. 1, p. 55-67, 2013.
BHANGU, A.; et al. appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet, vol. 386, n. 10000, p. 1278-1287, 2015.
BIRNBAUM, B. A.; WILSON, S. R. Appendicitis at the millennium. Radiology, vol. 215, n. 2, p. 337-48, 2000.
CHAN, W. T.; et al. Does appendix position affect the clinical outcome of acute appendicitis? Annals of the College of Surgeons Hong Kong, vol. 6, n. 4, p. 109-12, 2002.
EL-MASRY, N. S.; THEODOROU, N. A. Retroperitoneal perforation of the appendix presenting as right thigh abscess. Int Surg., vol. 87, n. 2, p. 61-4, 2002.
GHORBANI, A.; FOROUZESH, M.; KAZEMIFAR, A. M. Variation in Anatomical Position of Vermiform Appendix among Iranian Population: An Old Issue Which Has Not Lost Its Importance. Anat Res Int., vol. 2014, p. 313575, 2014.
GOLALIPOUR, M. J.; et al. Anatomical Variations Of Vermiform Appendix In South-East Caspian Sea (Gorgan-IRAN). Journal of the Anatomical Society of India, vol. 52, n. 2, p. 141-43, 2003.
JONES, W. R.; KAYE, M. D.; ING, R. M. The lymphoid development of the fetal and neonatal appendix. Biol Neonate, vol. 20, n. 5, p. 334-45, 1972.
KHATUN, S.; THAKUR, D.; SHAH, D. K. Prevalence of Retrocaecal Appendix among Patients with Appendicitis in A Tertiary Care Hospital of Nepal. JNMA J Nepal Med Assoc., vol. 57, n. 217, p. 150-153, 2017.
MALAS, M. A.; GÖKÇIMEN, A.; SULAK, O. Growing of caecum and vermiform appendix during the fetal period. Fetal Diagn Ther, vol. 16, n. 3173-7, 2001.
MALAS, M. A.; et al. Development of the vermiform appendix during the fetal period. Surg Radiol Anat., vol. 26, n. 3, p. 202-7, 2004.
MANISHA, L. C.; et al. A study of morphology of vermifrom appendix in 200 cases. Int J Med Res Health Sci., vol. 2, n. 4, p. 780-85, 2013.
MOHAMMADI, S.; et al. Morphological variations of the vermiform appendix in Iranian cadavers: a study from developing countries. Folia Morphol (Warsz), vol. 76, n. 4, p. 695-701, 2017.
MWACHAKA, P.; et al. Variations in the position and length of the vermiform appendix in a black kenyan population. ISRN Anat., n. 2014, p. 871048, 2014.
NAYAK, B. S. Why the tip of vermiform appendix has variable position? Med Hypotheses, vol. 75, n. 6, p. 682-3, 2010.
OUATTARA, D.; et al. Classification of the terminal arterial vascularization of the appendix with a view to its use in reconstructive microsurgery. Surg Radiol Anat., vol. 29, n. 8, p. 635-41, 2007.
PAUL, U. K.; et al. Position of vermiform appendix: a postmortem study. Bangladesh J Anat., vol. 7, n. 1, p. 34-6, 2009.
RAHMAN, M. M.; et al. Anatomical positions of vermiform apêndix in Bangladeshi people. J Bangladesh Soc Physiol., n. 1, p. 5-9, 2006.
SEARLE, A. R.; et al. Changes in the length and diameter of the normal appendix throughout childhood. J Pediatr Surg., vol. 48, n. 7, p. 1535-9, 2013.
SHAH, M. A.; SHAH, M. The position of the vermiform appendix. Ind Med Gaz., vol. 80, n. 10, p. 494, 1945.
SOLANKE, T. F. The position, length, and content of the vermiform appendix in Nigerians. Br J Surg., vol. 57, n. 2, p. 100-2, 1970.
SOUZA, S. C.; COSTA, S. R. M. R.; SOUZA, I. G. S. Vermiform appendix: positions and length – a study of 377 cases and literature review. Journal of Coloproctology, vol. 35, n. 04, p. 212-16, 2015.
SWATHIPRIYADARSHINI, C.; et al. A comprehensive study of mesoappendix and arterial pattern of appendix. Turk J Surg., vol. 38, n. 1, p. 55-59, 2022.
TOFIGHI, H.; et al. The anatomical position of appendix in Iranian cadavers. Int J med Toxicology Forensic Med., vol. 3, n. 4, p. 126-30, 2013.
VERGINIO, H. R.; et al. Apendicite aguda em paciente idoso: relato de caso. Arch Health Invest., vol. 8, n. 12, p. 818-20, 2019.
WAKELEY, C. P. The Position of the Vermiform Appendix as Ascertained by na Analysis of 10,000 Cases. J Anat., vol. 67, n. Pt 2, p. 277-83, 1993.
WILLIAMS, B. M.; et al. Appendicitis Mortality in a Resource-Limited Setting: Issues of Access and Failure to Rescue. J Surg Res., n. 259, p. 320-325, 2021.
APPENDIX – FOOTNOTE
10. Instituto Médico Legal (IML).
[1] Professor of Clinical Anatomy. ORCID: 0000-0002-2300-3330. Currículo Lattes: http://lattes.cnpq.br/6911783083973582.
[2] Internal Medicine Resident. ORCID: 0000-0002-5298-537X. Currículo Lattes: http://lattes.cnpq.br/6291628187714859.
[3] Internal Medicine Resident. ORCID: 0000-0001-9211-7000. Currículo Lattes: http://lattes.cnpq.br/4619345212343744.
[4] Medicine student. ORCID: 0000-0001-5924-8658. Currículo Lattes: http://lattes.cnpq.br/1862815448788019.
[5] Medicine student. ORCID: 0000-0002-1804-5114. Currículo Lattes: http://lattes.cnpq.br/0947941516831134.
[6] Medicine student. ORCID: 0000-0003-2773-9238. Currículo Lattes: http://lattes.cnpq.br/3363589852903709.
[7] Assistant Professor of Clinical Anatomy. ORCID: 0000-0002-2146-3499. Currículo Lattes: http://lattes.cnpq.br/3543011108453552.
[8] Professor of Molecular Biology. ORCID: 0000-0001-5705-6433. Currículo Lattes: http://lattes.cnpq.br/3337321488338686.
[9] Professor at the Faculty of Medicine. ORCID: 0000-0002-7776-1831. Currículo Lattes: http://lattes.cnpq.br/6858508576490184.
Submitted: March 13, 2023.
Approved: April 13, 2023.