REVIEW ARTICLE
FONSECA, Karine Lucas Tavares da [1], SOBRINHO, Raul Breves [2]
FONSECA, Karine Lucas Tavares da. SOBRINHO, Raul Breves. Patient response with lupus erythematosus to treatment with Yamamoto New Scalp Acupuncture (YNSA). Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 06, Ed. 04, Vol. 09, pp. 142-182. April 2021. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/with-lupus-erythemenasus, DOI: 10.32749/nucleodoconhecimento.com.br/health/with-lupus-erythemenasus
ABSTRACT
It is estimated that 5 million people worldwide have some form of Lupus. It is an autoimmune, idiopathic and until now incurable disease, which affects, especially women in reproductive period. In the West, its treatment is educational, essentially medication, with administration of anti-inflammatories, antimalarials and immunosuppressants. For Traditional Chinese Medicine (TCM), Lupus is above all a syndromic imbalance, which varies according to its manifestation. The set of these disorders is classified as deterioration of the Spleen (Pi) and Heart (Xin), weakening of the Fire and the Door of Life. Treatment by MTC occurs with the administration of herbal medicines, diet therapies, acupuncture, massage, moxibustion, Qi Gong, magnetotherapy, wind therapy, flowers and others. YNSA (Yamamoto Neue Schädelakupunktur) is a somatotopic scalp therapy that, among other advantages, has access points to the 12 main meridians, bilaterally. Usually used in case of pain, neurological disorders and surgical conditions, it has its own diagnostic methods that also serve to monitor the treatment. Ryodoraku is the most sensitive and reproducible current diagnostic tool for identifying the average circulating energy in the meridians. This research aimed to identify the usefulness of YNSA in the treatment of lupus patients. In this process, the energy evolution of a patient with lupus considered severe was monitored, over 23 applications of YNSA. It was compared with the results of acupuncture with those of allopathy. With YNSA, in addition to relaxation and pain control, there was greater energy adequacy. The relevant gains over the 23 applications of YNSA, reaching three times the initial energy pattern, have almost completely retreated to exclusive treatment with allopathy. In effect, chloroquine diphosphate brought much more losses than gains.
Keywords: YNSA, Lupus, Chloroquine Diphosphate, Acupuntura, Autoimmune disease.
1. INTRODUCTION
Lupus Erythematosus is an autoimmune disease that mainly affects women between 20 and 30 years of age. Discoid or systemic, if left untreated, can lead to death. In reliable literature, there is no case of cure or signal that leads to this path. Its etiology goes from genetics to psychology, going through the intricacies of gynecology, endocrinology, psychoneuroimmunology and pharmacology. In the eyes of Chinese medicine, it is a syndrome disorder, and can designate several syndromes according to the impairment.
YNSA (Yamamoto New Scalp Acupuncture or Yamamoto Neue Schädelakupunktur) is a Japanese scalp therapy, mainly used in cases of pain and neurological sequelae. It is also indicated for the treatment of internal organs and differs from the Chinese craniopuncture (developed a decade earlier), especially by the somatotopic and non-cortical approach (YAMAMOTO, 2007; BOUCINHAS, 2007) or reflexological (KWANG, s.d.).
According to Dethelefsen and Dahlke (1983, p. 16, 17) the disease is a state of the human being that indicates that in their consciousness there is disharmony. The mastery of physical and psychic activities, as well as organic structures, are promoted and commanded by the five essential organs, representatives of the Five Movements (YAMAMURA, 2004).
Converging TCM to Western concepts and YNSA to SLE, this monograph is subject to the standards of ABNT (Brazilian Association of Technical Standards), justifying:
- Socially, for launching a new look at the therapy in relation to lupus;
- Institutionally, it favors research and dissemination;
- Scientifically, it offers theme novelty backed by ryodoraku diagnosis and instigates discussions about YNSA in other autoimmune diseases.
In this work, the question arises: can YNSA be useful in controlling lupus? Lupus is a complex and multifactorial disease, which can be treated in several ways, depending on the manifestation of symptoms. YNSA immediately and extensively stimulates the brain, suggesting wide release of neurotransmitters (hills, biogenic amines, amino acids and neuropeptides), which are hormonosensitive (as well as lupus) and immunosensitive…
Specific objectives:
- Demonstrate the evolution of the 24 meridians via Ryodoraku during the treatment of the lupus patient with YNSA
- Compare the amperage of the 24 meridians of the lupus patient during: 1) exclusive treatment with YNSA; 2) the combination of YNSA with allopathy; and 3) the exclusive drug intervention;
- Assess the energy condition of the 5 Elements and Yin/Yang ratio
- Correlate eastern and western diagnostic and therapeutic perspectives;
- Record the patient’s impressions and reactions regarding YNSA treatment.
2. REVIEW
2.1 ERYTHEMATOSUS LUPUS ETYMO
“Lupus”, from the Latin lupus, synonym “lupo” (HOUAISS et al, 2009), means wolf. This is a term used to designate erosive skin lesions, in the form of a wolf bite (ANTAS, 1980; STEDMAN, 1990; COSTEIRA, 2001).
Systemic Lupus Erythematosus (SLE) is characterized by chronic inflammation of the skin, with ulcerations or blemishes, depending on the specific type (HOUAISS et al, 2009). Amadio (2002) defines it as a tuberculosis of the skin and Oliveira (2004) says it is one of a group of cutaneopathies in which the lesions are eroded.
2.2 ETIOLOGY AND PHYSIOPATHOLOGY OF SLE
Systemic Lupus Erythematosus (SLE) is the classic prototype of multisystemic disease of autoimmune origin, characterized by a wide range of autoantibodies, especially antinuclear (ANA) (COTRAN et al, 2000). Its autoimmune character is characterized by the production of antibodies against cell nucleus components, in association with a varied set of clinical manifestations (MAGALHÃES et al, 2003).
Its etiology is unknown and probably multifactorial (CECATTO et al, 2004), so that genetic, hormonal and environmental elements participate in its development (COMISSÃO DE LÚPUS DA SOCIEDADE BRASILEIRA DE REUMATOLOGIA, 2011). Studies suggest a relationship between SLE and the X chromosome and not with sexual gender or sex hormones (SCOFIELD et al, 2014).
According to Cotran et al (2000), the apparently unlimited number of antibodies in patients with lupus against autoconstituents is indicative that their fundamental defect is a failure of the regulatory mechanisms that maintain self-tolerance. Utiyama et al (2004), confirms. For him, it is the activation of complement, by immune complexes that are deposited in multiple organs that is connected to physiopathogeny. Complement is a labile thermo component of the serum capable of smoothing the bacterium that contributes to the defense of the host also by fixing opsonins or complement fragments on the bacterial surface, facilitating phagocytosis (MAYER, 2009; ABBAS et al, 2008).
Complement activation, which comprises more than 20 serum proteins (C1qrs, C2, C3, C4, etc.), can recruit and activate several cells, including polymorphonuclear cells and macrophages. In addition, it can participate in the regulation of antibody responses, as well as assist in the elimination of immunological complexes and apoptotic cells, or even contribute to inflammation and liver damage, generating anaphylaxis (MAYER, 2009).
Hereditary homozygous deficiency of C1q, C1r, C1s, C4 and C2 susceptibility to SLE. The impairment in the activation of the classical pathway due to this deficiency reflects in the solubilization and removal of the complexes. CR1 deficiency also compromises the removal of complexes, favoring their deposition in different tissues and, consequently, inflammation (UTIYAMA et al, 2004).
Another aspect involved in the triggering of this inflammatory disease (SOCIEDADE BRASILEIRA DE REUMATOLOGIA apud REIS et al, 2014), is in vitamin D deficiency (ARNSON et al, 2007), whose levels are inversely related to the activity of the disease (TEIXEIRA and COSTA, 2012).
Vitamin D acts on the regulation and differentiation of cells such as lymphocytes, macrophages and natural killer (NK) cells; interferes with the production of cytokines in vivo and in vitro; reduces the production of interleukin-2 (IL-2), interferon-gamma (INFγ) and tumor necrosis factor (TNF); inhibits il-6 expression and secretion and production of autoantibodies by B lymphocytes (MARQUES et al, 2010).
Stress does not cause lupus (SBR apud REIS et al, 2014), but the psychosomatic dimension considers stress and psychosocial suffering for triggering, evolution, worsening and possible control (MOREIRA and MELLO FILHO, 1992).
The risk of developing cancer from this inflammatory disease is about 1.15% higher than in the general population (SBR apud REIS et al, 2014) and 2.5% higher for malignant hematological diseases, such as lymphoma and leukemia (MEDEIROS, 2010).
Hypertension, hypercholesterolemia and renal failure, all conditions that are more frequent in lupus, contribute to heart diseases (SBR apud REIS et al, 2014), specifically, pancarditis (GROSS, 1932-1940 apud FALCÃO et al, 2000):
According to Auteroche and Navailh (1992, p. 37, 66, 76, 84, 128-129), Eiras (2006) and Wang (2001, p. 638), from the perspective of Traditional Chinese Medicine (TCM) in lupus occurs:
- Shen alteration (Mental activity);
- Disharmony in Gan (Responsible for ensuring the smooth progress and ease in the movements and transformation of Qi, with regulation of organic and visceral functions);
- Mucosity in the body (Product of partial interruption of metabolism of organic liquids, causing a condensation of moods);
- Poor fei that fails to regulate the circulation of defensive Qi to the skin;
- Shen Yin or Yang deficiency;
- Bi Migratory Syndrome (Syndrome that spreads throughout the body, starts and ends suddenly; one side can affect the other; its pain burns and can suddenly disappear);
- Out of control of Wei Qi (defense energy).
2.3 LES STATISTICS
SLE has a predilection for females of reproductive age, with onset of symptoms in the 2nd and 3rd decades of life and a ratio of nine to ten women to one man (AYACHE and COSTA, 2005; TISKIEVICZ, 2008; SATO et al, 2006).
It focuses on all ethnicities and geographical regions, especially individuals of African, Asian and Hispanic origin. Black ethnicity is 4 times more affected than white, affecting 1 in 1,000 white people and 1 in 250 black people (LUPUS FOUNDATION OF AMERICA, 2005; BONFÁ and NETO, 2000, p. 25-33 apud AYACHE and COSTA, 2005, p. 313).
It affects 1 in 700 women of childbearing age (DUTRAL and OLIVEIRA, 2009) and 1 in 1,700 Brazilian women (COMISSÃO DE LÚPUS DA SBR, 2011), with 10% to 20% genetic influence (AYACHE and COSTA, 2005, p. 313).
According to the Lupus Foundation of America (2005), based on available epidemiological data on the subject, researchers believe that at least 5 million people worldwide have lupus (0.08%), and more than 100,000 new cases each year develop (0.002%); probably low estimates.
Beltrão (2010) says there are no epidemiological studies in Brazil showing the incidence of SLE in the population. On the other hand, Villar and Sato (2001), nine years earlier, highlighted that the only sle incidence study conducted in Brazil occurred in Natal (RN), indicating an estimated 8.7 new cases per 100,000 inhabitants per year (0.01%).
For Villar and Sato (2001), the “high” incidence would be attributed to genetic and environmental factors, such as the permanent presence of sunlight with high rates of ultraviolet rays. It is important to highlight that the Data of the SBR, with statistical survey of the entire national territory, are 6 times higher than the surveys of Villar and Sato (2001).
Although the SBR Lupus Commission (2011) recognizes that it does not have exact numbers in Brazil, it is currently estimated that there are about 65,000 people with lupus; approximately 4,000 in Rio de Janeiro and 6,000 in São Paulo.
In the North American territory there is approximately 1 case of SLE in 194, or 0.51% or 1.4 million people (WD, 2011). Other studies indicate a prevalence ranging from 14 to 50/100,000 inhabitants and 1/2000 to 1/10,000 inhabitants (SATO et al, 2006; SANTO ANTONIO et al. 2004). Dutral and Oliveira (2009) state that the prevalence of SLE can reach up to 1 per 2,500 inhabitants in certain populations.
Studies conducted in the UK and USA indicate an incidence of SLE from 3.7 to 5.5/100,000 inhabitants per year, respectively (MEINÃO and SATO, 2008). Two years earlier, Santantonio et al (2006) reported an approximate incidence of 5.7 to 7.6 cases per year per 100,000 inhabitants in The United States.
The Lupus Foundation of America (2005) estimates that 1.5 million Americans have a form of lupus. Scheinberg (2013) points to an estimated 5 million. In the last four decades alone, the incidence of lupus has almost tripled. The U.S. Centers for Disease Control and Prevention has published a report suggesting that lupus deaths have increased nearly 60 percent over 20 years.
Regarding morbidity, a study conducted in Rio Grande do Sul with 72 lupus patients (93% female) and 2,384 individuals from the community (55% female with a mean age of 42 years) identified psychiatric alterations in 89% of patients with SLE and 13% in individuals in the community. The level of morbidity was related to low school level, but not with family income (BELTRÃO, 2010).
2.4 DIAGNOSIS OF LUPUS
2.4.1 WESTERN DIAGNOSIS OF SLE
The diagnostic accuracy of Lupus depends on the evaluation of clinical, histopathological, IFD and serological reactions (BERBERT and MANTESE, 2005):
- Clinical: According to the criteria established by the American College of Rheumatology;
- Histopathological: Hyperquesatosis, thickening of the basal membrane with follicular tamponade, thinning and flattening of the Malpighian stratum (BERBERT and MANTESE, 2005, p. 1, 4);
- IFD: Of all available serological tests, the highest value in screening for SLE is Direct Immunofluorescence;
- Serological reactions: Detection of ANA, speckled, peripheral, homogeneous or nucleolar (JÚNIOR, 2007; BELTRÃO, 2010).
The criteria for diagnostic classification of SLE by the American College of Rheumatology were defined in 1982, pointing to the presence of at least 4 of the 11 criteria in the observation interval (BORBA et al, 2008, p. 196-197; JÚNIOR, 2007; BELTRÃO, 2010). They are: Eritema malar; discoide injury; photosensitivity; oral/nose ulcers; arthritis; serosite; renal impairment; neurological alterations; hematological changes; immunological changes; antinuclear antibodies.
2.4.2 EASTERN DIAGNOSIS OF SLES
For CTM, health corresponds to a state of equilibrium between the 5 elements and between the 2 opposite aspects, which results in the balance between body, mind and spirit. Diseases are seen as a rupture of this harmony (NASCIMENTO, 2006).
Skin, complexion, bones, meridians, odors, sounds, mental status, preferences, emotions, tongue, pulse, habits and body fluids reflect the state of internal systems and can be used in Chinese diagnosis, which, in turn, is based on the fundamental principle that signs and symptoms reflect the condition of internal systems (MACIOCIA, 1996; YAMAMURA, 1996).
The patterns indicate a disharmony that guide all clinical manifestations; which is the essence of Chinese pathology and medical diagnosis, which is given by observation; hearing and olfaction; anamnesis and palpation (MACIOCIA, 1996). For Mann (1996), there is no absolute norm, and something that can be normal for one individual, for another it can be pathological. An example of this is the relationship between temperament variations and radial artery quality.
2.4.3 DIAGNOSIS OF SLE BY RYODORAKU
Yoshio Nakatani developed the medicine Ryodoraku in 1950 at Kyoto University (GOTO, s.d.), from a device (Neuro Meter / Energy Meter), containing 12 volts of direct current, loaded with a current of 200 microamperes (AMORIM, s.d.). With this, it proved that it was possible to diagnose and act in the internal organs through the Ryodoraku “permeable pathways” related to the Autonomic Nervous System (SOBRINHO, 2007).
Ryodoraku is a stimulus therapy that refers to diagnosis and therapy based on its own theory, which recognizes electropermeability at points with electrical variation (Ryodo Points or Reactive Ryodo Points), naming the lines that connect these Ryodoraku points (GOTO, s.d.).
Nakatani’s work began to be used as a diagnostic parameter in traditional acupuncture. This diagnosis mediates the electroconductivity of the different representative points, 12 on the right side and twelve on the left side, of which 6 are in the hands (represented by the letter H) and 6 are in the feet (represented by the letter F) (AMORIM, s.d.).
2.4.4 DIAGNOSIS BY YNSA
Acupuncture points, located in energy channels and projected onto the skin, represent the most exterior of the interior-exterior ratio of organs and viscera (YAMAMURA, 1995, p. 39).
In YNSA, both abdominal and cervical diagnosis are essential to determine which points should be treated. Yamamoto splits his head according to a vertical line passing through the apex of the ear. Usually, for Yang problems (pain), points of the Yin region are sought; and for Yin problems (paralysis), points from the Yang region are sought (YAMAMOTO, 2007; KWANG, s.d.).
2.5 CONVENTIONAL THERAPEUTIC APPROACH
No medicine works for lupus in the same way (WALLACE, s.d.). The treatment includes a series of measures, which include drugs such as cortisone and/or thalidomide, anti-inflammatory drugs, antimalarials and immunosuppressants, as well as standards for living well (WALLACE, s.d.; MAGALHÃES et al, 2003). It is an individualized treatment, which depends on the affected organs or systems and the severity of the lesions (JÚNIOR, 2007).
The professional should guide people with SLE to learn about the disease; avoid sun and lamps as a function of ultraviolet radiation; psychotherapy and physical activity; adopt a balanced diet, reducing salt, carbohydrates and lipids; avoid smoking; if women, suspend contraceptives; avoid infections; and learn how to differentiate symptoms that can be caused by other diseases (KRAUTHAMER et al, 1999; SATO et al, 2002).
For Greco et al (2013), supplements such as vitamin D, omega 3 fatty acids, N-acetylcysteine and turmeric have been shown to be useful in controlling the disease. Mind-body methods such as cognitive behavioral therapy and other counseling interventions can improve mood and quality of life in SLE.
2.6 LES SECOND MTC
In TCM, all diseases are analyzed through energy disorders. Depending on the phase and organs affected, lupus can be Liver Fire; Kidney Yin deficiency; disharmony between Water and Fire; deterioration of the Spleen and Heart; heat accumulation in the Heart and Spleen, with insufficiency of the Yin of the Kidney that causes the hyperactivity of Fire; weakening of the Fire and the door of life; heat-moisture in the joints; etc. (KWANG, 2009; MEDEIROS, 2009). Other terms are “Mai Xing Pan Zhuang Hong Ban Xing Lang Chuang” and “Xi Tong Hong Xing Ban Lang Chuang” (JIAN-HUI, s.d.).
For TCM, lupus is a Bi-Migratory Syndrome, with Shen, Hun, Po, Yi and Zhi disorder (EIRAS, 2006; SOUSA and VASONCELOS, s.d.). In this polysyndrome (WANG, 2001, p; 638; KWANG, 2009), there is burning pain; generalized according to blood circulation; sudden onand end and one side may affect the other. It should be punctured repeatedly, even if the pain stops, to avoid remission (WANG, 2001, p. 638).
2.7 ENERGY SYNDROMES
The syndromes can be external or true: by Wind (Feng), Heat (Re) and Fire (Huo), Canicula (Huo) or Summer Heat (Syu), Moisture (Shi), Dryness (Zao) or Cold (Han). They can also be internal or false: by Internal Wind, Internal Heat, Internal Humidity, Internal Dryness or Internal Cold (KWANG, s.d.).
2.8 COMPLEMENTARY AND ALTERNATIVE METHODS FOR SLE
At T.C.M., the treatment of energy disorders aims to restore the balance of the 5 Elements and consists in the administration of herbal medicines such as Radix Glycyrrhizae (Gan Cao), Dai Qing Gao and/or Liu Wei Di Huang Wan. Also dietotherapies, Qi Gong practice, acupuncture, massage, mhoxhum, magnetotherapy, suction cup therapy, florals and others. Such measures are also used as prophylaxis. With this, it is estimated that more than 50% of patients with SLE are using complementary and alternative medicine (KWANG, 2008; JIAN-HUI, s.d.; GRECO et al, 2013).
2.8.1 ACUPUNCTURE
From latin acum (needle) punctum (sting), acupuncture means needle prick. In Japanese (Shin-Kyu) and Chinese (Zhen-Jiu), it means needle and moxa (HUSZ, 2007).
Acupuncture is the set of theoretical-empirical knowledge of traditional Chinese medicine that aims at the therapy and cure of diseases through the application of needles and moxas, in addition to other techniques (WEN, 2006). It alters blood circulation; promotes the release of hormones such as endorphins; increases host resistance; regulates organic functions and stimulates metabolism (WEN, 2006).
It has sedative effect; antiemetic; myorelaxant; antacid; immunizer; healing; aesthetic; neurorehabilitation; anxiolytic, antidepressant, hypnotic; antispasmodic; detoxifying; analgesic; bronchodilator (HUSZ, 2007).
In acupuncture, 5-Hydroxy-Tryptophan is released (SCOTTO, 2006; MARTINS et al, 2010), increases acetylcholine levels in the thalamus, restricting cholinesterase activity, which reduces levels of 17-Hydroxycorticosterone, and increasing the sensation of analgesia. Through peripheral stimuli, acupuncture accesses the SNC and SNA, modulating and increasing the immune response (SCOTTO, 2006).
As for the physiology of acupuncture, there are four accepted theories: 1. Transmission of Bioelectric Currents, with change in neuron membrane potential; 2. Biological repression, with repression of a nervous signal or elevation of the pain threshold; 3. Comportas Theory, with opening and closing of doors that allow the painful signal to pass through aferent fibers; 4. Immunological theory, with increased cellular immunity (T-lymphocytes) and plasma immunity (B-lymphocytes) (SCOTTO, 2006).
2.8.2 ELECTROSTIMULATION AND ELECTROACUPUNCTURE:
It is estimated that electricity in acupuncture treatments has been used since the first half of the 19th century. Despite this, electroacupuncture only began to be used more frequently from the 1930s onto the 1930s and became more widespread since the 1960s (AMESTOY, 2005).
In YNSA, the recommended adjustment of electrical stimulation should be around 5 to 15 Hz, 1,000 to 15,000 μA or be adjusted according to patient tolerance (YAMAMOTO et al, 2007).
2.9 JAPANESE CRANIAL SOMATOTOPIA – YNSA
YNSA was developed in 1970 and published in 1973 on the occasion of the 25th meeting of the Japanese Ryodoraku Society (Japischen Ryodoraku Gesellschaft); with a description of Points A, B, C, D and E. To emphasize the fact that Yamamoto’s craniopuntura is different from the Chinese craniopuntura known until then, the term “new” was purposely added (YAMAMOTO et al, 2007, p. 3; BOUCINHAS, 2007, p. 47).
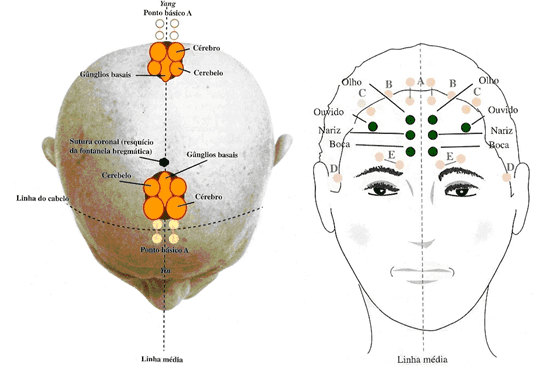
YNSA is a somatotopic acupuncture (Figures 1, 2 and 3), so the whole body mirrors over a small area. From Yamamoto’s perspective, the head divides according to a vertical line passing through the apex of the ear. The anterior part is Yin and the posterior is Yang. The Yang part treats the Yin disturbances and the Yin part treats the Yang disturbances (YAMAMOTO et al, 2007, p. 3; KWANG, s.d.).
Figure 1: Part Yin and part Yang, according to Yamamoto’s somatotopia.
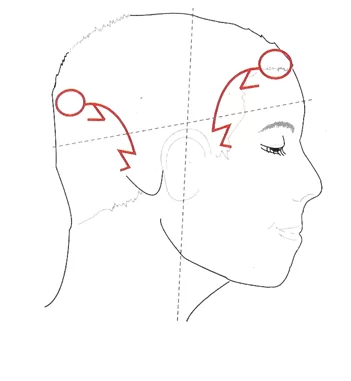
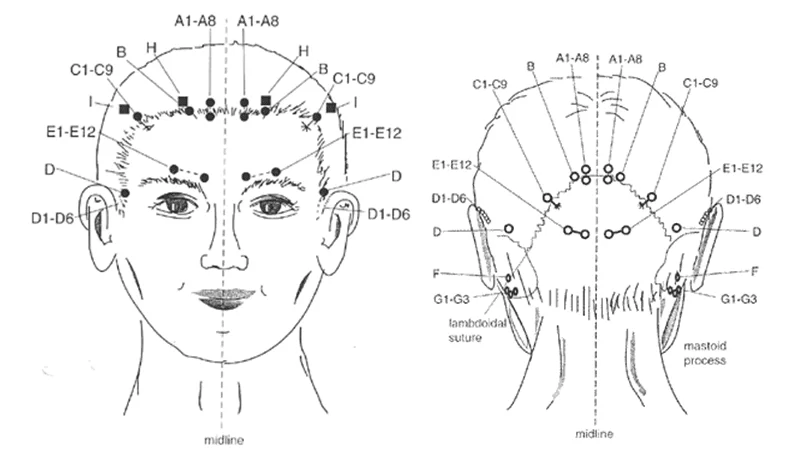
figure. 2. YNSA base points.
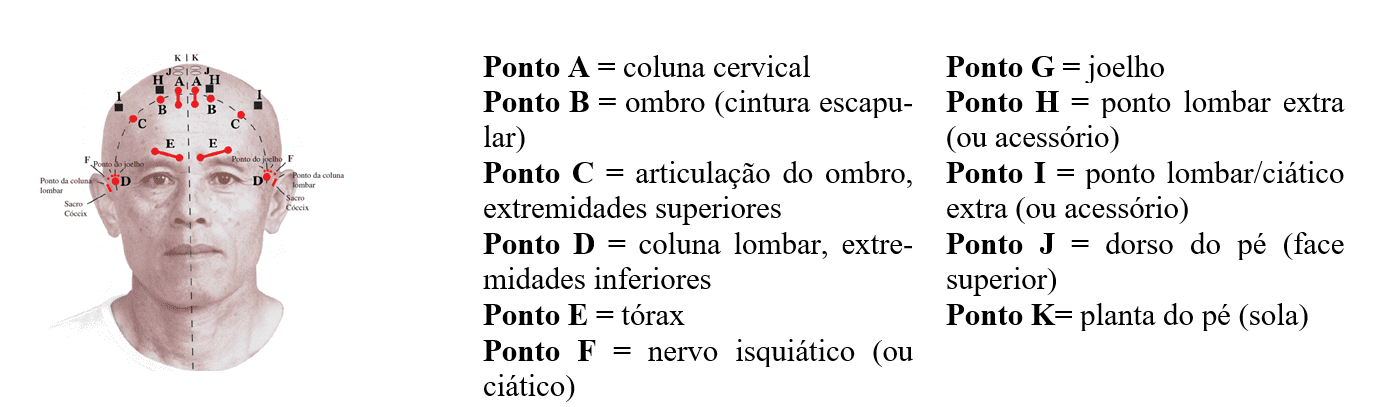
Figure 3. YNSAbase points, part Yin and Yang part, respectively.
They are two hemi-somatotopias, one Yin in the structural-anatomical part and another Yang, being corresponding, almost true specular images juxtamarketed, peer-to-peer, to the Yin (BOUCINHAS, 2007).
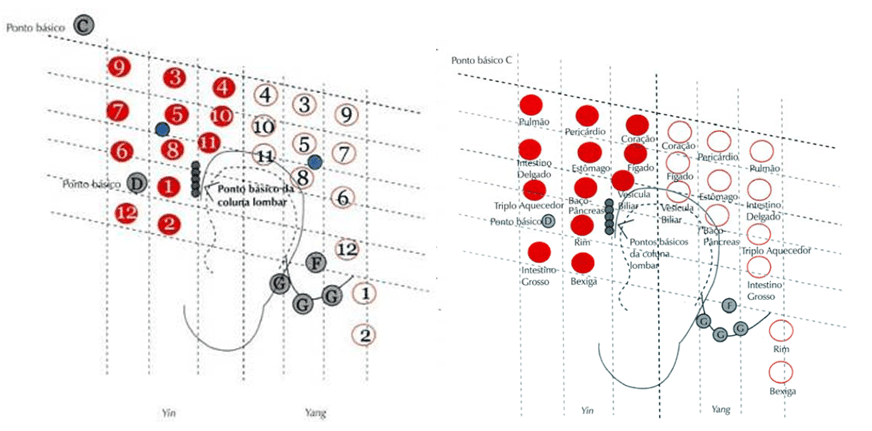
The Energetic or Functional Hemi-Somatotopia Yin differs fundamentally from structural or basic, because it comprises the Y Points (Yamamoto Points), which are correspondence with the Zang-Fu of the TCM (Figure 4). They are used for meridian energy disorders, linked to internal organ disorders and is also a field for psychosomatic, vegetative and meridian indications (BOUCINHAS, 2007).
Figure 4: Yamamoto Y points.
The YNSA is divided into four groups of points (Figure 5): 1. Basic points: Locomotor apparatus.; 2. Brain points: Brain, cerebellum and basal ganglia; 3. Sensory points: Sense organs; 4. Points Y: Internal organs (YAMAMOTO et al, 2007).
Figure 5: YNSA Points: Cerebral on the left and Sensory on the right.
2.9.1 YNSA PROCEDURES
After anamnesis, with recognition of the patient’s basic problem, the corresponding area is palpated in the Yin Structural Somatotopia (Basic Points), to check if it is painful or “high and hardened”. It is repeated. (BOUCINHAS, 2007). In general, the side homolateral to the complaints is chosen. For sequelae such as stroke, the contralateral side (KWANG, s.d.) is used.
If the patient’s complaint is above the diaphragm, it is recommended to palpate, first of all, the IG4 point (Hegu), in order to determine the most sensitive side, which will be the first to be treated. In problems in the lower body, one should tighten the D point symmetrically and use the more sensitive side as well (YAMAMOTO et al, 2007, p. 71; KWANG, s.d.) (Figure 6).
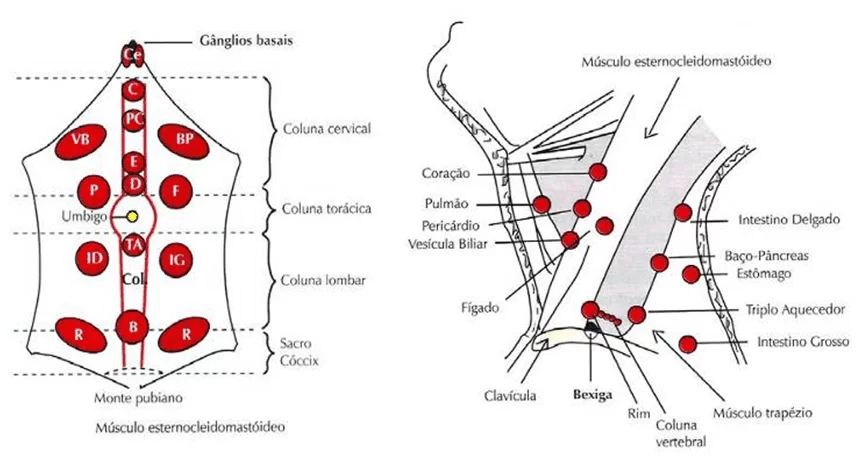
In cases with changes in organs or meridians, it is important to diagnose cervical or abdominal sensitive points (KWANG, s.d) (Figure 7). The entire length of a meridian is contained within a respective Y-spot and any point of classical acupuncture belonging to a meridian can be treated by point Y (YAMAMOTO et al., 2017).
Figure 6: IG4 and D points, respectively, used to define the side to be treated.
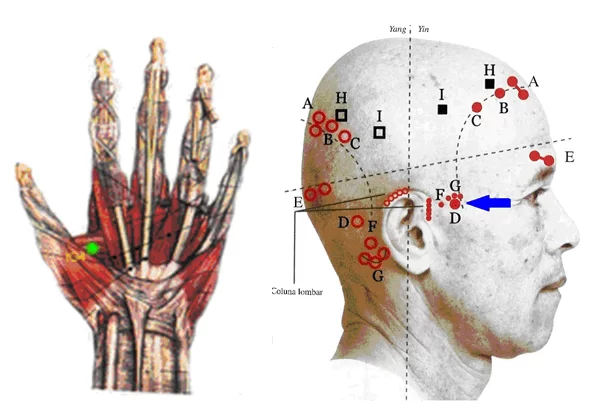
Figure 7: Points used in abdominal and cervical diagnosis in YNSA.
2.10.2 INDICATIONS FOR YNSA
The 11 basic points of YNSA are used for nerve motor dysfunctions, pain and other dysfunctions of the locomotor system caused by injuries, surgical procedures or alterations of the type tumors or disc hernias. Treatment of internal organs by the basic points is rare. The 4 sensory points are used for dysfunctions, pain snares and allergic processes related to the organs of the senses (YAMAMOTO et al, 2007).
2.10.3 CONTRAINDICATIONS TO YNSA
Without contraindications to any treatment with YNSA, care is recommended for febrile or too weakened-looking patients (YAMAMOTO et al, 2007).
2.10.4 LUPUS-YNSA RATIO
Despite the indication for the treatment of lupus with YNSA (YAMAMOTO et al, 2007), in 7 languages (English, Portuguese, Spanish, Italian, French, German and Chinese), no research was found in this line.
3. MATERIALS AND METHOD
3.1 SERVICE PLACE
The Acupuntura & Terapias Therapies office located at Corphus Academia, in the city of Mogi das Cruzes, SP, was the place chosen for the practice of this research, in 2009. Reason: Infrastructure.
3.2 SUBJECT
Because it is a case study and demandmore rigor, the selection of the patient for this research was according to the following criteria:
- Be carrier of Systemic Lupus Erythematosus;
- Being female (Predominant gender);
- Moderate to high severity (recent hospitalization, lower limb amputation and persistent anemia);
- Recurrent signs and symptoms.
3.3 MATERIALS AND PROCEDURES
Sulfite A4 leaf, Times New Roman font, letter size 12 and 9 were used in the preparation of the forms and the questionnaire. The AccusPoint ryodoraku appliance was used in the 24 sessions, as well as hydrophilic cotton of the Apollo brand and drinking water to perform the exams.
In the treatment, needles of the Dong Bang brand, 25x40mm (sterilized and reused[3]) and Electrostimulator of the Lautz brand, with 6 cables, were used, in continuous mode[4].
The volunteer was explained the treatment to be performed; required prior bath only with water in all sessions; applied the “Free and Informed Consent Form”; the “Initial Evaluation Form”; in the 23rd and last application of YNSA, the “Final Evaluation Form”; and after 30 days (11/8/9) a new analysis was made and the Questionnaire was applied. The 24th session of the research did not have scalpotherapy and ceased with the patient’s wrist responses in the Questionnaire.
3.4 DATA ANALYSIS
Data analysis was performed by interpretative and structural method. interpretive, by assessing the details of the data collected; organization and classification by categories. structural, by data analysis and concentrated efforts to find patterns in the situation under study.
4. RESULTS AND DISCUSSIONS
The values are recorded in excel worksheet for ryodoraku chart formation and automatically a midpoint is determined between them, tracing in following, a parallel line. From the average, two parallel lines of 7 mm each are drawn. The range of 14 mm found corresponds to the energy normality of the graph (AMORIM, s.d.).
4.1 EVOLUTION OF THE ENERGY AVERAGES OF THE PERSON WITH LUPUS DURING TREATMENT WITH YNSA
In the initial evaluation of the patient, Ryodoraku graphs indicated a markedly low overall energy condition; reaching 27% of the minimum energy considered normal (45-70 μA) in left CS7 and C7. Left hemibody (HE) presented 54% of the desired minimum energy and right hemibody (HD) 72%. The first session of YNSA, HD was performed with an advance of 0.6% and HE by 17% (Table 1).
Table 1: Results obtained by Ryodoraku before and after the first YNSA session
| Before the 1st session of YNSA | After the 1st session of YNSA | |||
| Left. (a) | Right (b) | Left. | Right . | |
| P9 | 22 | 33 | 29 | 30 |
| CS7 | 12 | 28 | 18 | 24 |
| C7 | 12 | 28 | 16 | 34 |
| ID5 | 19 | 22 | 21 | 30 |
| TA4 | 29 | 39 | 28 | 42 |
| IG5 | 28 | 35 | 28 | 41 |
| BP3 | 28 | 22 | 25 | 10 |
| F3 | 47 | 71 | 45 | 47 |
| R4 | 25 | 30 | 33 | 38 |
| B65 | 15 | 18 | 19 | 14 |
| VB | 21 | 22 | 34 | 34 |
| E42 | 35 | 39 | 47 | 46 |
| Average | 24,4 | 32,3 | 28,6 | 32,5 |
(a) Left: Left hemibody energy in microamps (μA).
(b) Right: Right hemibody energy in microamps (μA).
Until the 12th session, the oscillating advances resulted, in HE, an energy increase of 41%, mitigating the initial deficit from 46% to 24%. HD has progressed 26%, reducing its deficit from 28% to 10%. The lowest value found was in left C7 and right B65, both with 51% of the desired minimum energy (Table 2). From the beginning to the end of craniopuncture sessions (Table 3), the volunteer had an energy advance of 32% in HE (deficit reduction from 46% to 13%) and 24% advance in HD (Deficit reduction from 28% to 3%). Performed the 23rd and last acupuncture, in relation to the beginning of the research, HE advanced 61% and, HD advanced 35%.
Table 2. Results obtained by Ryodoraku in the 12th and 23rd session of YNSA
| 12th session of YNSA | 23rd session of YNSA | |||
| Left. (a) | Right (b) | Left. | Right | |
| P9 | 30 | 33 | 36 | 40 |
| CS7 | 31 | 29 | 40 | 45 |
| C7 | 23 | 33 | 39 | 45 |
| ID5 | 31 | 30 | 41 | 45 |
| TA4 | 30 | 32 | 45 | 45 |
| IG5 | 29 | 38 | 42 | 45 |
| BP3 | 27 | 46 | 31 | 45 |
| F3 | 49 | 60 | 41 | 52 |
| R4 | 50 | 45 | 44 | 44 |
| B65 | 31 | 23 | 30 | 21 |
| VB | 35 | 55 | 37 | 45 |
| E42 | 47 | 63 | 46 | 50 |
| Average | 34,4 | 40,6 | 39,3 | 43,5 |
(a) Left: Left hemibody energy in microamps (μA).
(b) Right: Right hemibody energy in microamps (μA).
Table 3. Results obtained by Ryodoraku before the 1st and 23rd session of YNSA, and after the 23rd session of YNSA.
| Before the 1st session | Before the 23rd session | After the 23rd session | ||||
| Left. (a) | Right (b) | Left. | Right. | Left. | Right. | |
| P9 | 22 | 33 | 19 | 28 | 36 | 40 |
| CS7 | 12 | 28 | 16 | 22 | 40 | 45 |
| C7 | 12 | 28 | 20 | 21 | 39 | 45 |
| ID5 | 19 | 22 | 26 | 38 | 41 | 45 |
| TA4 | 29 | 39 | 29 | 38 | 45 | 45 |
| IG5 | 28 | 35 | 31 | 37 | 42 | 45 |
| BP3 | 28 | 22 | 36 | 41 | 31 | 45 |
| F3 | 47 | 71 | 36 | 45 | 41 | 52 |
| R4 | 25 | 30 | 44 | 35 | 44 | 44 |
| B65 | 15 | 18 | 35 | 34 | 30 | 21 |
| VB | 21 | 22 | 36 | 43 | 37 | 45 |
| E42 | 35 | 39 | 51 | 45 | 46 | 50 |
| Average | 24,4 | 32,3 | 31,6 | 35,6 | 39,3 | 43,5 |
(a) Left: Left hemibody energy in microamps (μA).
(b) Right: Right hemibody energy in microamps (μA).
4.2 INFLUENCE OF ALLOPATHY ON RESEARCH RESULTS
With the implementation of chloroquine diphosphate (DC), which took place around the 14th application of YNSA, HE slowed its progress; already HD advanced. The energy of right F, which from the beginning showed a tendency to excess, was even more exacerbated with the drug and the patient began to complain of cracks in the tips of the fingers and toes. During this period, 3 dental restorations were given.
After one month without YNSA, but with drug treatment, half of the meridians, involving the metal, fire and wood elements, were below the initial condition of the research. The rest: water, earth, part wood and fire, achieved at least higher values than the initialones.
4.3 FINAL SEARCH RESULTS
From the 23rd and last application of YNSA to the 24th and last meeting, which took place after one month of exclusive allopathy, the setback was intense (Table 4).
Table 4. Results obtained by Ryodoraku before the 1st YNSA session, after the 23rd YNSA session and after one month of YNSA suspension.
| Before the 1st session | After the 23rd session | After 1 month without YNSA | |||||
| Left. (a) | Right (b) | Left. | Right. | Left. | Right. | ||
| P9 | 22 | 33 | 36 | 40 | 19 | 19 | |
| CS7 | 12 | 28 | 40 | 45 | 14 | 23 | |
| C7 | 12 | 28 | 39 | 45 | 13 | 24 | |
| ID5 | 19 | 22 | 41 | 45 | 14 | 21 | |
| TA4 | 29 | 39 | 45 | 45 | 23 | 26 | |
| IG5 | 28 | 35 | 42 | 45 | 26 | 25 | |
| BP3 | 28 | 22 | 31 | 45 | 45 | 49 | |
| F3 | 47 | 71 | 41 | 52 | 52 | 50 | |
| R4 | 25 | 30 | 44 | 44 | 42 | 48 | |
| B65 | 15 | 18 | 30 | 21 | 56 | 26 | |
| VB | 21 | 22 | 37 | 45 | 20 | 30 | |
| E42 | 35 | 39 | 46 | 50 | 40 | 47 | |
| Average | 24,4 | 32,3 | 39,3 | 43,5 | 30,3 | 32,3 | |
(a) Left: Left hemibody energy in microamps (μA).
(b) Right: Right hemibody energy in microamps (μA).
Unlike the beginning of the research that were outside the maximum and minimum line, only F, E, CS and C, after 1 month without YNSA, there was distancing of almost all meridians, for more or less, indicating a change in the generation cycles (Xiag Sheng) and Dominance (Xiang Ke).
Between the patient’s energy balance and the relative predominance of 5 Zang and 6 Fu in any of the hemibodies, no correlation was seen.
Except f, already strengthened in relation to the other meridians, all other Zang Fu showed increased amperage at the end of ynsa applications.
From the first evaluation to the first month of discontinuation of YNSA treatment, the evolution of left hemibody was 5.91uA (24%) and right hemibody was 0.08uA (irrelevant percentage), demonstrating retreat in results.
4.4 VARIATIONS IN THE TREATMENT OF LUPUS EXCLUSIVELY WITH YNSA, YNSA WITH CHLOROCHINE DIPHOSPHATE AND CHLOROCHINE DIPHOSPHATE ONLY
The ratio of gains and losses during the research fluctuated a lot. Most Zang Fu responded better to exclusive treatment with YNSA and, although right P, C and bilateral CS also evolved with YNSA allied to DC, in this second situation, the evolution occurred much more timidly.
With exclusive scalpotherapy, only bilateral F regressed, which was harmonizing, since F at first was expressly more developed than the other 22 meridians, which in turn advanced.
In the combination of YNSA and DC, 18 meridians regressed: Zang Fu of Water, Wood and Earth, in addition to left P and ID, bilateral IG and TA. Right ID, on the other hand, maintained the result prior to the therapeutic combination and the rest progressed.
In the exclusive consumption of the drug, compared to the combination of YNSA and antimalarial drugs, 17 meridians receded: P / IG, C / ID, CS / TA, left R, bilateral VB and E. Despite this, the exclusivity of the drug was significantly positive for left BP and bilateral B, and, although to a lesser extent, also for left F, right BP (which in isolation with YNSA responded better) and, finally, right R, which in turn , with YNSA combined evolved better.
4.4.1 TREATMENT OF LUPUS PATIENT EXCLUSIVELY WITH YNSA
Over the initial 13 applications of YNSA, left hemibody gained on average 63.46μA/session (total 825μA) and right on average 74.75μA/session (total 897μA). In this process, each left hemibody meridian evolved on average 5.29μA/session and right hemibody 5.75μA/session.
By the setbacks that characterized the intervals between sessions, the accumulated rate up to immediately before the 13th session was only 5.9μA in left hemibody (mean/session 0.49μA) and 3.2μA in the right hemibody (mean/session 0.27μA). During the 13th application, the accumulated throughout the treatment jumped to 18.1μA (mean/application1.39μA) in the left hemibody and 13.3μA (mean/application 1.02μA) in the right hemibody. The results were shown to be better on average immediately after the sessions than in the intervals.
4.4.2 ENERGY DEVELOPMENTS IN THE THERAPEUTIC COMBINATION OF YNSA WITH CHLOROCHINE DIFOSPHATE
In the combined treatment of YNSA with DC (10 sessions, distributed in 1 month), HE gained on average 47.3μA/session (Total 473μA), while HD advanced on average 28.2μA/session (Total 282μA). This corresponded to an increase of 3.94μA/session in each HE meridian and an increase of 2.35μA/session in each HD meridian.
The energy development of the 14th pre-application to the 23rd pre-application of YNSA was -8.5μA in HE (mean/session -0.94μA) and -6.4μA in HD (mean/session -0.71μA). After the last application of YNSA combined with allopathic treatment (23rd session of the research), the accumulated regression in relation to the previous combined treatment (14th session of the research) was minimized, from -8.5μA to -0.8μA in HE (mean/application -0.08μA) and the decline in HD was converted into advancement, going from -6.4μA to +1.5μA (mean/application +0.15μA).
The DC combined with YNSA impaired the response to treatment.
4.4.3 ENERGY DEVELOPMENT ONLY WITH CHLOROQUINE DIPHOSPHATE
The continuous and exclusive use of DC for 1 month resulted from the last application of scalpotherapy at the 24th meeting, in a rewind of -9μA (mean per meridian -0.75μA) in HE and -11.2μA (mean per meridian -0.93 μA) in HD. From the previous application of YNSA to the last evaluation (after 1 month of treatment with antimalarial), the energetic kickback in HE was much less impacting (although also important), with a variation of -1.3μA in HE and -3.3 μA in HD.
At the end of the research, already without YNSA, the indentation was so expressive that the values were leveled to those obtained at the beginning: Small variation of +5.9μA in HE and null in HD. According to the available data, although it is impossible to ascertain whether the final energy leveling in relation to the initial parameters occurred by the suspension of the YNSA and/or by the toxicity of the drug, the therapeutic evolution points to the second hypothesis.
4.5. YIN AND YANG ASPECTS OF THE PATIENT DURING THE SEARCH
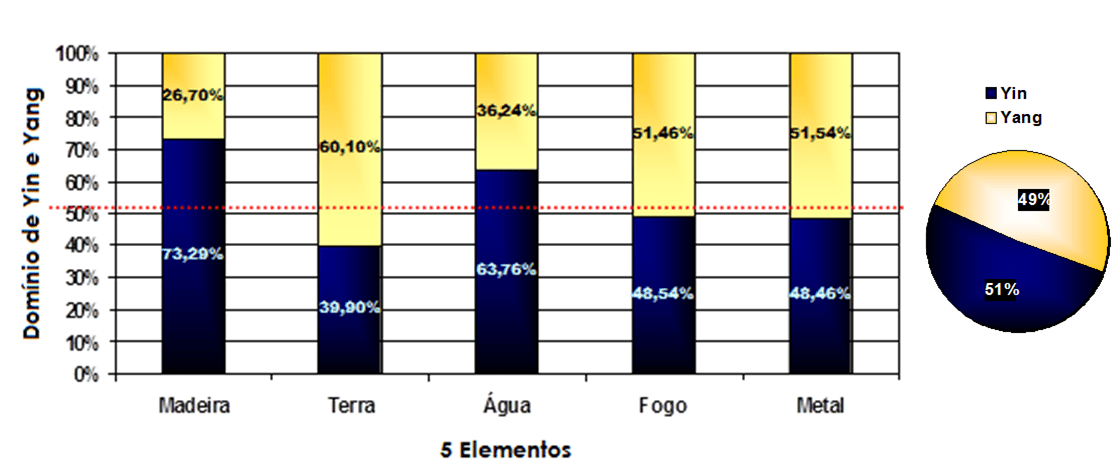
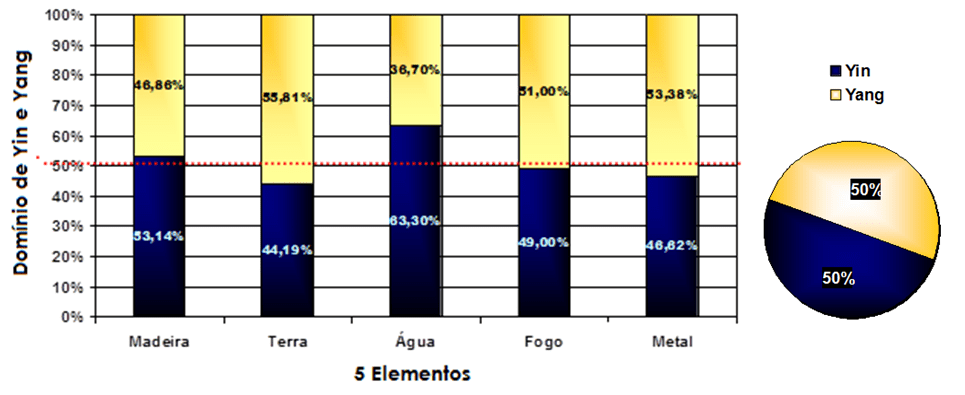
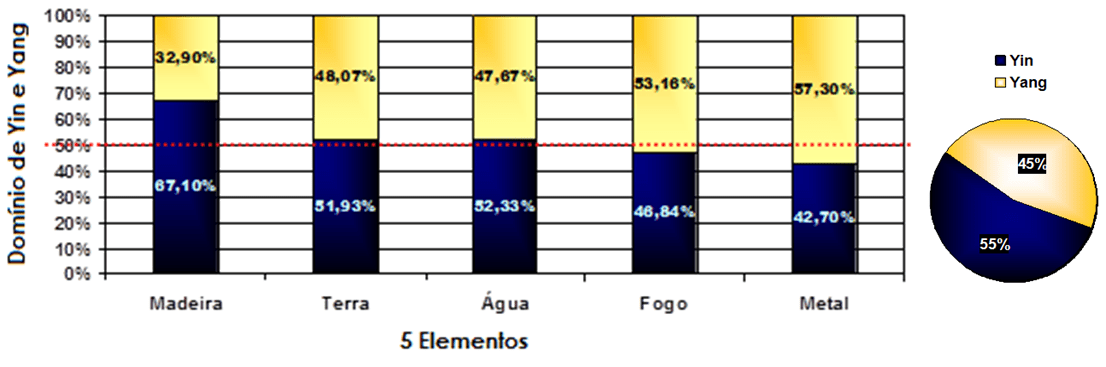
With YNSA, the initial condition more Yin than Yang (Graph 1) was balancing (Graph 2), reaching the equitable participation of antagonistic and complementary polarities (Graph 3). Suspended the YNSA, in 1 month, returned to be predominantly Yin, although with greater balance of the Yin-Yang ratio in the 5 Elements (Graph 4). In the last scalpotherapy, Madeira Yin was more controlled (Compare Graphs 1, 2 and 3), other elements progressed (Graphs 2, 3 and 4) with greater proportionality (Graphs 1 and 5).
Graph 1. Yin and Yang ratio of the 5 Elements in the 1st evaluation.
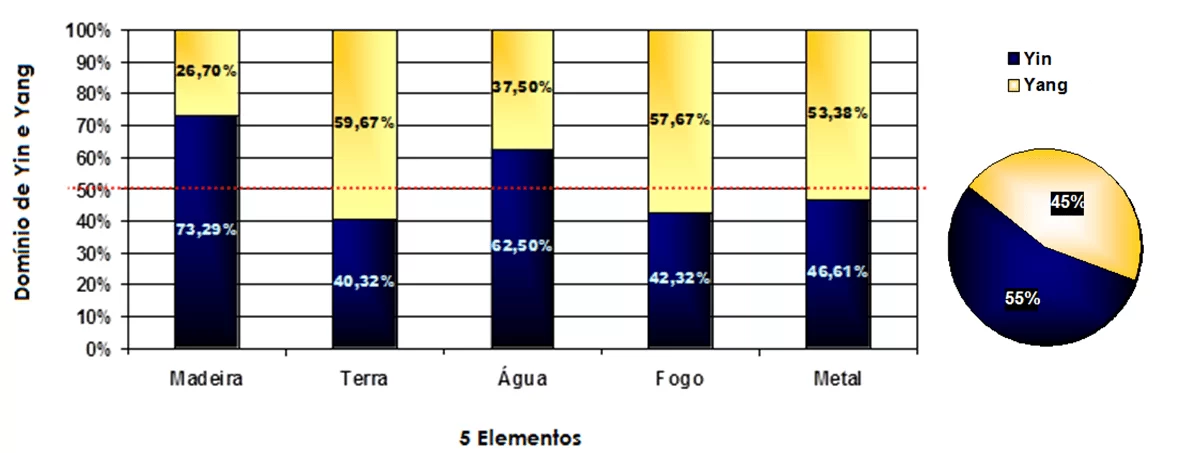
Graph 2. Yin and Yang ratio of the 5 Elements in the 12th application of YNSA.
Graph 3. Yin and Yang ratio of the 5 Elements in the 23rd YNSA application.
Graph 4. Yin and Yang ratio of the 5 Elements in the last evaluation of the research, after 1 month of allopathic treatment and suspension of YNSA.
4.6 ZANG FU ANALYSIS THROUGHOUT THE RESEARCH
4.6.1 EVOLUTION OF LUNG OR SIF DURING RESEARCH
Lung (P) showed increased stability with YNSA, especially in HE (Table 6). He progressed with YNSA and went back wards with DC intervention, a process that worsened with scalpotherapy suspension.
Table 6.Evolution of lung meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
 P presented, respectively, before and after the sessions, maximum of 52μA and 47μA in HE, and maximum of 51μA and 54μA in HD. The minimum acquired, also respectively before and after the sessions, was 13μA and 20μA in HE, and 21μA and 23μA in HD. Therefore, the mean obtained respectively before and after the YNSA sessions was 28.9μA and 32.04μA in HE, and 33.61μA and 36.17μA in HD. The energy oscillations were more pronounced in the intervals between sessions than during the sessions: The coefficient of variation was, respectively, before and after the YNSA, 0.34 and 0.23 in HE and 0.29 and 0.25 in HD.
P presented, respectively, before and after the sessions, maximum of 52μA and 47μA in HE, and maximum of 51μA and 54μA in HD. The minimum acquired, also respectively before and after the sessions, was 13μA and 20μA in HE, and 21μA and 23μA in HD. Therefore, the mean obtained respectively before and after the YNSA sessions was 28.9μA and 32.04μA in HE, and 33.61μA and 36.17μA in HD. The energy oscillations were more pronounced in the intervals between sessions than during the sessions: The coefficient of variation was, respectively, before and after the YNSA, 0.34 and 0.23 in HE and 0.29 and 0.25 in HD.
4.6.2 EVOLUTION OF LARGE INTESTINE OR CHANG DURING RESEARCH
Like P, Large Intestine (GA) evolved better with the YNSA intervention (Table 7). Likea, she progressed with YNSA and retreated with CD, a process aggravated by scalp ore therapy suspension.
Therefore, respectively before and after the sessions, P presented a maximum of 56μA and 57μA in HE and 55μA and 61μA in HD. The minimum acquired was, respectively before and after the sessions, 17μA and 26μA in HE, and 18μA and 32μA in HD. The mean found was, respectively before and after the sessions, 38.22μA and 40.26μA in HE, and 43.96μA and 45.30μA in HD. The energy oscillations were the same before and after the YNSA sessions in HE (Coefficient of variation: 0.23) and more pronounced in the intervals between sessions than during HD sessions (Coefficient of variation before and after scalpotherapy, respectively, of 0.20 and 0.14).
Table 7. Progress of large intestine meridians in the research “Response of patient with LE to treatment with YNSA – Case Study”
| large intestine | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | +67,85% | +5,21% | -8,69% | -0,86% | -38,09% | |
| Right | +40,00% | +3,07% | -10,00% | -1,00% | -44,44% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | +50,00% | +21,17% | -7,14% | -0,29% | ||
| Right | +28,57% | +1,24% | -28,57% | -0,19% |
4.6.3 EVOLUTION OF KIDNEY OR SHEN DURING RESEARCH
Kidney (R), to the YNSA intervention, evolved more in HE than in HD (Table 8). In the association of DC with acupuncture, both hemibodies receded, especially right. In the exclusive administration of DC, HD has evolved again and HE continued to decline.
R, respectively before and after the sessions, presented in HE, maximum of 48μA and 70μA; meanwhile, in HD it was a maximum of 59μA and 70μA. The minimum acquired was respectively before and after the sessions, 18μA and 33μA in HE, and 30μA and 33μA in HD.
The mean, respectively before and after scalp therapy sessions, was 35μA and 48.26μA in HE, and 45μA and 51.87μA in HD. Among the YNSA sessions, energy oscillations were subtly more pronounced in HE and, during the sessions, the oscillations were more accentuated in HD. The coefficient of variation, respectively before and after YNSA was 0.27 and 0.20 in HE and 0.18 and 0.19 in HD.
Table 8.Progress of rim meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
| kidney | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | +80,00% | +6,15% | -4,34% | -0,43% | -4,54% | |
| Right | +53,33% | +4,10% | -16,98% | -1,69% | 9,09% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 76,00% | 3,30% | 68,00% | 2,83% | ||
| Right | 46,66% | 2,02% | 60,00% | 2,50% |
4.6.4 EVOLUTION OF BLADDER OR PANG GUANG DURING THE SEARCH
Bladder (B) varied more after than before YNSA applications (Table 9). Progressed with YNSA, regressed in the combination of YNSA with CD, and progressed again after discontinuation of drug-continuity scalpotherapy. In fact, only with DC B progressed more, especially in HE.
Table 9. Progress of bladder meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
| bladder | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 66,66% | 5,12% | -18,91% | -1,89% | 86,66% | |
| Right | 27,77% | 2,13% | -25,00% | -2,50% | 23,80% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 100,00% | 4,34% | 273,33% | 11,38% | ||
| Right | 16,66% | 0,72% | 44,44% | 1,85% |
Respectively before and after scalpotherapy, B presented a maximum of 45μA and 57μA in HE and 47μA and 61μA in HD. The minimum obtained was, respectively before and after scalpotherapy, 15μA and 16μA in HE, and 17μA and 12μA in HD.
Averages were found, respectively before and after the sessions, of 30.61μA and 31.78μA in HE, and of 28.87μA and 27.87μA in HD. The energy oscillations were more accentuated immediately after scalpotherapy, with coefficient of variation, respectively before and after YNSA, of 0.32 and 0.34 in HE, and 0.30 and 0.40 in HD.
4.6.5 LIVER OR GAN EVOLUTION DURING RESEARCH
Liver (F) at the beginning of the research presented a picture in the CTM known as Tyranny. Under these conditions, the excess Zang Fu begins to depress the “grandson”.
F oscillated more in the scalp omission intervals than during the sessions (Table 10) and regressed with YNSA, especially in combination with DC. After acupuncture, he progressed in HE and continued to decline in HD, but slowed down (Table 10).
It exhibited, respectively before and after YNSA, a maximum of 75μA and 70μA in HE, and 77μA and 91μA in HD. The minimum acquired was, respectively before and after the applications of YNSA, of 32μA and 21μA in HE, and of 38μA and 37μA in HD.
Table 10. Progress of liver meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
| liver | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | -4,25% | -0,32% | -19,60% | -1,96% | 26,82% | |
| Right | -5,63% | -0,43% | -14,75% | -1,47% | -3,84% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | -12,76% | -0,55% | 10,63% | 0,44% | ||
| Right | -26,76% | -1,16% | -2,93% | -0,12% |
The mean found in HE was 46.96μA before and 49.74μA after scalpotherapy, and the mean found in right hemibody was 55.78μA before and 59.96μA after scalpotherapy. The energy oscillations were slightly more pronounced in the YNSA sessions and not in the intervals: The coefficient of variation was, respectively before and after acupuncture, 0.21 and 0.22 in HE, and 0.19 and 0.20 in HD.
4.6.6 EVOLUTION OF GALLBLADDER OR DAN DURING RESEARCH
Gallbladder (VB) was more variable between YNSA sessions than during. It progressed with YNSA, regressed in the combination of YNSA with DC and regressed further in the exclusive administration of antimalarial (Table 11).
Before and after the sessions, respectively, VB presented a maximum of 70μA and 63μA in HE and 69μA and 76μA in HD. The minimum obtained was, respectively before and after scalpotherapy, 21μA and 27μA in HE, and 22μA and 31μA in HD.
The means found, respectively before and after the sessions, were 36.74μA and 43.04μA in HE, and 46.87μA and 51.26μA in HD. The greatest energy variation occurred in the interval between the YNSA sessions, especially in HE. The coefficient of variation, respectively before and after, was 0.32 and 0.23 in HE; 0.22 and 0.21 in HD.
Table 11. Progress of gallbladder meridians in the research “Response of patient with LE to treatment with YNSA – Case Study”
| gall bladder | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 114,28% | 18,79% | -22,91% | -2,29% | -45,94% | |
| Right | 131,81% | 10,13% | -21,05% | -2,10% | -33,33% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 76,19% | 3,31% | -4,76% | -0,19% | ||
| Right | 104,54% | 4,54% | 36,36% | 1,51% |
4.6.7 HEART EVOLUTION OR XIN DURING RESEARCH
Heart (C) in HE progressed more during scalpotherapy, and in HD, more between sessions (Table 12). It evolved a lot with YNSA, especially in HE, and crashed with the DC intervention. Suspended craniopuncture, but with permanence of the drug, declined in both hemibodies reaching, in HD, to values lower than those of the first evaluation.
C showed, respectively before and after the sessions, a maximum of 37μA and 47μA in HE and 46μA and 50μA in HD. It obtained a minimum, respectively before and after YNSA, of 12μA and 16μA in HE, and of 14μA and 23μA in HD.
Their means were, respectively before and after the YNSA sessions, 27.09μA and 32.43μA in HE, and 27.70μA and 36.30μA in HD. The coefficient of variation, respectively before and after, was 0.25 and 0.26 in HE, and 0.27 and 0.21 in HD.
Table 12. Progress of heart meridians throughout the research “Patient response with Lupus Erythematosus to treatment with YNSA – Case Study”
| heart | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 175,00% | 13,46% | 11,42% | 1,14% | -66,66% | |
| Right | 39,28% | 3,02% | 18,42% | 1,84% | -46,66% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 225,00% | 9,78% | 8,33% | 0,34% | ||
| Right | 60,71% | 2,63% | -14,28% | -0,59% |
4.6.8 EVOLUTION OF SMALL INTESTINE OR XIAO CHANG DURING RESEARCH
Small Intestine (ID) evolved in exclusive treatment with YNSA (Table 13), and, in combination with DC, declined in HE, remaining in HD. Suspended YNSA and allopathy was maintained, it declined substantially, reaching levels lower than those found at the beginning of the study in both hemibodies.
Table 13. Progress of small intestine meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
| small intestine | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 110,52% | 8,50% | -10,86% | -1,08% | -65,85% | |
| Right | 90,90% | 6,99% | 0,00% | 0,00% | -53,33% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 115,78% | 5,03% | -26,31% | -1,09% | ||
| Right | 104,54% | 4,54% | -4,54% | -1,18% |
During scalpotherapy it varied slightly lower than between sessions. Its coefficient of variation in HE was, respectively before and after YNSA, 0.27 and 0.25; HD was 0.26 and 0.25.
It reached, respectively before and after YNSA, a maximum of 41μA and 53μA in HE, and 47μA and 50μA in HD. It obtained a minimum of 16μA and 21μA in HE, and 20μA and 22μA in HD.
Their means were, respectively before and after the YNSA sessions, 26.91μA and 34.30μA in HE, and 33.65μA and 38.26μA in HD.
4.6.9 EVOLUTION OF CIRCULATION-SEX OR XIN BAO LUO DURING RESEARCH
Circulation-sex (CS) evolved with acupuncture; continued to evolve, but slowly in the combination of DC, and declined to the suspension of YNSA (Table 14). At the end of the research, the decline in HD with the drug was so much, it reached an energy standard lower than that initially found in the research.
It varied more between YNSA sessions than during scalpotherapy. Its coefficient of variation was, in HE, 0.33 and 0.25, respectively before and after YNSA; and, in HD, 0.36 and 0.27 respectively before and after YNSA.
Table 14.Progress of circulation-sex meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
| Circulation-Sex | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 241,66% | 18,58% | 25,00% | 2,50% | -65,00% | |
| Right | 60,71% | 4,67% | 40,62% | 4,06% | -48,88% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 233,33% | 10,14% | 16,66% | 0,69% | ||
| Right | 60,71% | 2,63% | -17,85% | -0,74% |
Before and after the sessions, respectively, CS presented a maximum of 39μA and 50μA in HE and 47μA and 50μA in HD. Respectively before and after scalpotherapy, the minimum obtained was 12μA and 18μA in both hemibodies; the means were 24.13μA and 30.57μA in HE, and 26.13μA and 34.83μA in HD.
4.6.10 EVOLUTION OF TRIPLE-HEATER OR SAN JIAO DURING THE SEARCH
Triple-heater (TA) varied more its energy between YNSA sessions than during treatment. The coefficient of variation of 0.23 and 0.19 in HE, respectively before and after scalpotherapy, obtained a coefficient of variation of 0.23 and 0.19 in HE, and 0.19 and 0.17 in HD.
He progressed with YNSA, further to the right, and regressed to the DC combination, especially when acupuncture was suspended. In exclusive allopathy, it retreated in such a way that it reached values lower than those at the beginning of the research in HE (Table 15).
TA reached, respectively before and after the sessions, a maximum of 56μA and 55μA in HE and 55μA and 58μA in HD. It obtained a minimum, respectively before and after YNSA, of 19μA and 28μA in HE, and of 20μA and 26μA in HD.
Table 15. Progress of Triple-Heater Meridians in the research “Response of the patient with Lupus Erythematosus to treatment with YNSA – Case Study”
| Triple-Heater | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 17,94% | 1,38% | -13,46% | -1,34% | -42,22% | |
| Right | 97,14% | 7,47% | -11,53% | -1,15% | -13,04% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 15,38% | 0,66% | -33,33% | -1,38% | ||
| Right | 31,42% | 1,36% | 14,28% | 0,59% |
Their means, respectively before and after the YNSA sessions, were 39.30μA and 41.09μA in HE and 44.04μA and 45.13μA in HD.
4.6.11 EVOLUTION OF SPLEEN-PANCREAS OR PI DURING RESEARCH
Right Spleen-Pancreas (BP) changed more in the YNSA sessions than in the intervals; the opposite occurred in left BP. It presented, respectively before and after YNSA, coefficient of variation of 0.35 and 0.37 in HD, and of 0.31 and 0.26 in HE.
He progressed, above all to the right in exclusive treatment with YNSA, and, soon after the combination of DC. In the exclusive allopathy, his energy rose again, especially to the left (Table 16).
Table 16. Progress of spleen-pancreas meridians throughout the research “Response of patient with LE to treatment with YNSA – Case Study”
| Spleen-Pancreas | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 25,00% | 1,92% | -13,88% | -1,38% | 45,16% | |
| Right | 127,27% | 9,79% | -23,72% | -2,37% | 8,88% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 10,71% | 0,46% | 60,71% | 2,52% | ||
| Right | 104,54% | 4,54% | 122,72% | 5,11% |
Before and after YNSA, BP obtained the same maximum of 47μA in HE; on HD, obtained 67μA before and 76μA after scalpotherapy. Its minimum was, respectively before and after YNSA, 12μA and 18μA in HE, and 14μA and 10μA in HD. Meanwhile, the means found, respectively before and after the YNSA sessions, were 29.87μA and 31.41μA in HE and 40.48μA and 44.17μA in HD.
4.6.12 EVOLUTION OF STOMACH OR WEI DURING RESEARCH
Stomach (E) oscillated more during YNSA than in the interval between sessions. Its coefficient of variation was, respectively before and after scalpotherapy, 0.17 and 0.23 in HE and 0.18 and 0.22 in HD. He progressed with YNSA, regressed to the combination of DC and plummeted into exclusive allopathy (Table 17).
Table 17. Progress of stomach meridians throughout the research “Patient response with Lupus Erythematosus to treatment with YNSA – Case Study”
| Stomach | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 97,14% | 7,47% | -11,53% | -1,15% | -13,04% | |
| Right | 25,64% | 1,97% | -12,28% | -1,22% | -6,00% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 31,42% | 1,36% | 14,28% | 0,59% | ||
| Right | 28,20% | 1,22% | 20,51% | 0,85% |
The maximum, respectively before and after scalpotherapy, was 65μA and 86μA in HE; and 63μA and 85μA in HD. The minimum was, respectively before and after YNSA, 30μA and 40μA in HE, and 26μA and 30μA in HD. The means found were, respectively before and after YNSA, 46.43μA and 54.61μA in HE and 50.04μA and 55.17μA in HD.
4.6.13 EVOLUTION OF ENERGY AVERAGES DURING THE SURVEY
On average, HE varied slightly more between YNSA sessions than during therapy; the opposite occurred in HD. The coefficient of variation in HE was, respectively before and after YNSA, 0.17μA and 0.16μA in HE, and 0.15μA and 0.17μA in HD.
In the final calculation, the volunteer progressed in exclusive scalp therapy, regressed in the combination of DC, especially in the exclusive allopathy (Table 18).
The mean of the entire study was, respectively before and after YNSA, 34.22μA and 39.35μA in HE and 51.3μA and 58.1μA in HD. The maximum was 44.3μA and 53.1μA in HE, and 51.3μA and 58.1μA in HD. The minimum was 22.9μA and 29μA in HE, and 26.8μA and 31.2μA in HD.
Table 18. Progress of hemibody means throughout the research “Response of the patient with Lupus Erythematosus to the treatment with YNSA – Case Study”
| Average hemirbodies | Hemibody | YNSA (1-13) | YNSA (1-13) medium / session | YNSA+DC
(14-23) |
YNSA+DC
(14-23) medium / session |
DC (23-24) |
| Left | 11,84% | 0,91% | -9,65% | -0,96% | -22,90% | |
| Right | 16,03% | 1,23% | -8,61% | -0,86% | -25,74% | |
| After 23 apl. YNSA (1-23) | After 23 apl. YNSA (1-23) medium / session | After the research (1-24) | After research (1-24) medium / session | |||
| Left | 3,42% | 0,14% | -20,26% | -0,84% | ||
| Right | 10,68% | 0,46% | -17,81% | -0,74% |
4.7 ENERGY PREDOMINANCE OF THE 5 ELEMENTS DURING THE SEARCH
The 5 elements were predominant in HD. Although the 12 Zang Fu varied greatly in the research, with an energy predominance now in HE, or in HD, the weak correlation between scalpotherapy and the predominance of Zang Fu on one side to the detriment of the other indicated Pearson: -0.04192 in HE and Pearson: 0.168675 in HD.
5. CONCLUSIONS
This study pointed to the most relevant issues of energy character in the treatment of Lupus with Electroacupuncture in the YNSA technique. We used a patient considered severe, after screening involving more than 300 lupus patients, selected and indicated by a rheumatologist, professor of medicine in Mogi das Cruzes. The criterion was the presence of lupus, moderate to severe patient. This volunteer had suffered 3 months before the study, lower limb amputation due to the disease, presented anemic condition, functional hyperkalephosis and apathetic expression. After 23 applications, his posture was more erect, of self-confidence, safety and serenity, maintaining this standard until the 24th and last meeting.
In Ryodoraku it was observed in the first intense and generalized session (with the exception of Liver) energy deficit, indicating severe degenerative process. The normality of the energy average of some hemibody, disregarding the particularity of each meridian, was only possible after two applications of YNSA in the right hemibody, and after eight applications of YNSA in the left hemibody.
At the time of the eighth session, for the first time, even before scalp therapy, right hemibody started session with adequate energy average, despite deficits in numerous meridians of the same hemibody. Even with the advances, the mean energy of the left hemibody did not present at any time of the normalized research before YNSA, as in none of the 47 evaluations, the 24 normalized meridians were simultaneously found.
Throughout the research, the patient demonstrated unstable energy and inability to maintain a line of energetic rise or decline: They were ups and downs. While, in general, YNSA has improved its overall energy standard. Although scalpotherapy proved effective if continued in SLE, there were rare moments in which the technique itself depressed the already deficient energy pattern and the advance occurred between sessions.
2/3 of the sessions with normal energy average were composed of post-sessions and 1/3 of pre-sessions. This suggests that better results are more immediate than in the medium term and that over the course of the days there is usually energy decline. This data is in line with the great energy decline observed in the 24th meeting, after a month of suspension therapy.
Of the 5 sessions (10th, 16th, 17th, 18th and 22nd) whose patient attended with normal energy average, only in the 22nd session, instead of reinforcing this condition, YNSA provided energy levels below normal. Apparently, what differentiated the 22nd session from the others (10th, 16th, 17th and 18th) to obtain a differentiated final result, were the menstrual signs absent until then, for more than 9 months, and that manifested in the coming days… And/or, perhaps, the incipient flu.
In relation to exclusive therapy with YNSA, the association of chloroquine diphosphate brought more negative than positive results and YNSA prevented the energy aggravation caused by allopathy in the middle of treatment. Due to the energy oscillation throughout the treatment with the subsequent fall in a single month without YNSA, it is concluded the need for continuity of treatment with YNSA to preserve a more adequate energy state.
Despite the negative variations and the lack of cure for Lupus, throughout the research there were situations of tripling of the body’s very deficient energy pattern. Indeed, the volunteer herself was expressly happy with the result.
REFERENCES
ABBAS, A.K. et. al. Imunologia Celular e Molecular. 6. ed. 564p. Rio de Janeiro: Elsevier, 2008 ISBN 978-85-352-2244-9
AMADIO, I. Dicionário de Termos Médicos e de Enfermagem. P. 295. 1 Ed. São Paulo: Rideel, 2002.
AMESTOY, R. D. F.. Eletroterapia e Eletroacupuntura. Cap. 1. Breve Referência Histórica da Eletricidade e Seu Emprego em Eletroterapia e Eletroacupuntura. p. 8. Florianópolis: Absoluta, 2005.
AMORIM, E.K.; AMORIM, P.F.C.. Ryodoraku: Método de Avaliação. VII Simpósio Brasileiro de Aperfeiçoamento em Acupuntura e Terapias Orientais – EBRAMEC. Acupuntura Japonesa e Técnicas Associadas. Disponível em: <http://www.ebramec. com.br/palestras/palestras1/Paulo%20e%20%C9rika.pdf>. Acesso em: 5/914.
ANTAS, L.M., 1980. Dicionário de Termos Técnicos Inglês-Português. 6ª Ed: Traço.
AP 585 Accurate Pulse Microprocessado. Manual de Instruções – MS 80005120011. Fabricante: VMV Costa. CNPJ: 71.594.899/0001-66. Distribuidor: Lautz. P. 6.
ARNSON, Y; AMITAL, H.; SHOENFELD, Y. Vitamin D and autoimmunity: new etiological and therapeutic considerations. Ann Rheum Dis 2007; 66:1137-42.
AUTEROCHE, B. e NAVAILH, P.. O Diagnóstico na Medicina Chinesa. Andrei, 1992. P: 37, 66, 76, 84, 128-129.
AYACHE, D. C. G.; COSTA, I. P. da. Alterações da Personalidade no Lúpus Eritematoso Sistêmico. Personality Disorders in Systemic Lupus Erythematosus. Revista Brasileira de Reumatologia, v. 45, p.313, set./out., 2005.
BELTRÃO, S.M.R. Prevalência de sintomas psiquiátricos em pacientes com Lúpus Eritematoso Sistêmico em um centro de referência. Dissertação de Mestrado para obtenção do grau de Mestre pelo Programa de Pós-Graduação em Medicina da Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS). Porto Alegre: 2010.
BERBERT, A. L. C. V e MANTESE, S. A. de O. Lúpus eritematoso cutâneo – Aspectos clínicos e laboratoriais. Anais Brasileiros de Dermatologia, vol.80 nº 2, Rio de Janeiro, 2005. Disponível em: <https://www.scielo.br/j/abd/a/zLK4S5BCrWZc77f3vsDK3sM/?lang=pt>.
BONFÁ, E.S.D.O.; NETO, E.F.B.B.. Lúpus Eritematoso Sistêmico. In: BONFÁ, E.S.D.O.; IOSHINARI, N.H.: Reumatologia para o clínico. São Paulo: Roca, 2000. P: 25-33.
BORBA, E.F; et al. Consenso de Lúpus Eritematoso Sistêmico. Consensus of Systemic Lupus Erythematosus. Rev. Bras. Reumatol., v.48, n.4, p.196-197, jul/ago 2008. Disponível em: < http://www.scielo.br/pdf/rbr/v48n4/v48n4a02.pdf>. Acesso em: 15/7/14.
BOUCINHAS, J.. Acupuntura Craniana de Yamamoto. Cap. 5. Idéias básicas sobre YNSA. WP Gráfica e Editora, 2007. p.: 47, 50, 105.
CALLADO, J.C.. Nova Craniopuntura Japonesa. Caderno – Anotações da 11ª aula do curso de pós-graduação em acupuntura lato sensu, turma XXII, do CBF/CEATA. Ano: 2008.
CECATTO, S.B., GARCIA, R.I.D., COSTA, K.S., ANTI, S.M.A., LONGONE, E., RAPOPORT, P.B.. Perda auditiva sensorioneural no lúpus eritematoso sistêmico: relato de três casos. Rev Bras Otorrinolaringol. V. 70, n.3, 398-403, mai/jun 2004. Disponível em: <http://www.scielo.br/pdf/%0D/rboto/v70n3/a17v70n3.pdf>. Acesso em: 28/dez/11.
COMISSÃO DE LÚPUS DA SOCIEDADE BRASILEIRA DE REUMATOLOGIA – SBR. Lúpus Eritematoso Sistêmico (LES) – Cartilha da SBR. Ano: 2011. Disponível em: < http://www.reumatologia.com.br/index.asp?Pagina=reumatologia/principaisDoencasEorientacoesPacienteResultados.asp&IDPrincipalDoencaIDOrientacaoPaciente=OP;28>. Acesso em: 28/dez/11.
COSTEIRA, O., Termos e Expressões da Prática Médica. Rio de Janeiro: Farmoquímica, 2001. 262p. P. 114.
COTRAN, R. S., KUMAR, V., COLLINS, T.. Lúpus Eritematoso Sistêmico; Etiologia e Patogenia. Robbins: Patologia Estrutural e Funcional, p. 193, 194. Ano: 2000.
DETHLEFSEN, T. & DAHLKE, R.. A Doença como caminho. Cap.1. A doença e os sintomas. São Paulo: Cultrix, 1983. 265p. P. 16,17.
DUTRAL, R. M.; OLIVEIRA, T. B.. Lúpus eritematoso sistêmico (LES): perfil clínico-laboratorial dos pacientes atendidos em um serviço privado de reumatologia na cidade de Santo Ângelo-RS. Revista: RBAC, vol. 41(1): 77-80, 2009. Disponível em: <http://www.sbac.org.br/pt/pdfs/ rbac/rbac_41_01/rbac_41_0 1_14.pdf>. Acesso em: 7/5/11.
EIRAS, M. E. C.. Lúpus – Trabalho de Conclusão de Curso – Turma 80. Curso de Acupuntura e Medicina Tradicional Chinesa – CEATA, SP. Ano: 2006.
_________________. Equipe Doia. Lúpus Vulgar, Lúpus Carcinoma. Lúpus Vulgar. Dermis – Dermatology Information System. Disponível em: <http://www.dermis.net /dermisroot/pt/10368/image.htm>;<http://www.dermis.net/dermisroot/pt/10340/image.htm>;<http://www.dermis.net/dermisroot/pt/10275/image.htm>; <http://www.dermis.net/ dermisroot/pt/10376/image.htm>. Alemanha, 1996-2011. Acesso em: 7/5/11.
FALCÃO, C.A.; LUCENA, N.; ALVES, I.C.; PESSOA, A.L.;GODOI, E.T.. Cardite Lúpica. Arq Bras Cardiol vol.74 nº1. P: 56 Recife: 2000. Disponível em: < http://publicacoes.cardiol.br/abc/2000/7401/74010007.pdf>. Acesso em: 21/7/14.
GOTO, K. O que é Ryodoraku? JSRM – Japanese Society Ryodoraku Medicine. Disponível em: <http://www.ryodorakudobrasil.com.br/o-que-e-ryodoraku/>. Acesso em: 5/9/14. S.d.
GRECO, C.M.; NAKAJIMA, C.; MANZI, S. Update review of complementary and alternative medicine treatments for systemic lupus erythematosus. Curr Rheumatol Rep; 15 (11): 378, 2013 Nov. Portal de Pesquisas da BVS. Disponível em: <http://bvsalud.org/portal/resource/pt/mdl-24078104>. Acesso em: 15/7/14.
HOUAISS, A., VILLAR, M.S. e F.M.M., FRANCO, 2009. Houaiss da Língua Portuguesa. 1. ed. – Rio de Janeiro: Objetiva, 2009, 1986p. P.1202, 1899.
HUSZ, I.. O que é acupuntura. Apostila do Curso de Especialização em Acupuntura CBF/CEATA. Ano: 2007.
JIAN-HUI, L.. 1. Systemic Lupus Erithematosus; 2. Chronic Disciform Lupus Erythematosus. A Handbook of Tradicional Chinese Dermatologia. S.d. Acesso em: 2008.
JÚNIOR, A. M.. Lúpus Eritematoso Sistêmico. Disponível em: <http: // http://www.medicinageriatrica.com.br/tag/psicose/>. Acesso em: 2/mar/2004.
KONO, A. Craniopuntura de Yamamoto. Disponível em: < http://pontoacupuntura.blogspot. com.br/2011/05/cranioacupuntura-de-yamamoto.html >. Acesso em: 26/9/14.
KRAUTHAMER, A., COELHO, L.E. & SATO, E.I., 1999; SATO et al, 2002. Tratamento do LES. In E. I. Sato (Org.), Lúpus Eritematoso Sistêmico – O que é? Quais são suas causas? Como se trata? (p. 26-31). São Paulo: Sociedade Brasileira de Reumatologia.
KWANG, W. T., S/D. Classificação das Doenças; Etiopatogenia; YNSA. Apostilas do Curso de Especialização em Acupuntura CBF/CEATA, turma XXII. São Paulo, 2007.
KWANG, W.T.. Craniopuntura de Yamamoto – YNSA. Disponível em: < http://pt. slideshare.net/simonepascelli/yamamoto-ynsa)>. Acesso em: 8/9/14. S.d.
KWANG, W. T.. Entrevista. Jornal: O Legado. Ano: 2008.
KWANG, W. T., S/D. Mecanismo Neurofisiológico. Ponto de Acupuntura; Vias Aferente e Eferente da Acupuntura; Acupuntura e Neuroendocrinoimunologia. Apostila do Curso de Especialização em Acupuntura CBF/CEATA, turma XXII, Ano: 2007, p. 1,2,4.
KWANG, W. T.. Lúpus Eritematoso Sistêmico/Discóide. Disponível em E-mail: <[email protected]>. Ano: 2009.
KWANG, W.T., S/D. Craniopuntura 1 (YNSA 1) e Craniopuntura 2 (YNSA 2). DVD da Escola CEATA.
LUPUS Foundation of America, Inc., 2005. World Lupus Day Observed. Who Gets Lupus? Disponível em: <http://www.lupus.org/webmodules/webarticlesnet/?z=59&a= 1487>. Acesso em: 28/dez/11.
MACIOCIA, G.. Cap 16 – Diagnóstico; Cap 17 – Identificação dos Padrões. Os Fundamentos da Medicina Chinesa. São Paulo: Roca, 1996.
MACIOCIA, G. A Psique na Medicina Chinesa. Cap.9. A Prática da Medicina Chinesa: Tratamento das Doenças com Acupuntura e Ervas Chinesas. São Paulo: Roca, 2010.
MARTINS, A.C. C. L.; SILVA, T. M.; GLORIA, M. B. A. Determinação simultânea de precursores de serotonina – triptofano e 5-hidroxitriptofano – em café. Artigo. Quím. Nova vol.33. nº2. Disponível em: <http://www.scielo.br/scielo.php?pid=S0100-40422010000200016&script=sci_arttext>. Acesso em: 24/9/14. São Paulo, 2010.
MEDEIROS, E.F. Lúpus Eritematoso Sistêmico/Discóide. E-mail do [email protected]. Acesso em: 14/3/9. Ano: 2009.
MAGALHÃES M. B; DONADI E. A; LOUZADA JUNIOR, P. Manifestações clínicas do lúpus eritematoso sistêmico: Abordagem diagnóstica e terapêutica na sala de urgência. Medicina, Ribeirão Preto, 36: 409-417, abr/dez. Disponível em: <https://www.revistas.usp.br/rmrp/article/view/752/765>. Acesso em: 28/dez/11. Ribeirão Preto, 2003.
MANFRED, P. The theoretical foundations of Chinese medicine. Massachusetts: The MIT Press, 1974.
MANN, F.. Acupuntura – A Arte Chinesa de Curar. Hemus, 1994. P.: 98-101.
MARQUES, C. D. L; DANTAS, A. T; FRAGOSO, T. S; DUARTE, A. L. B. P. A importância dos níveis de vitamina D nas doenças autoimunes. Ver Bras Reumatol vol.50 nº1 São Paulo Jan/Feb. 2010. Disponível em: < https://www.scielo.br/j/rbr/a/5BcvSsQGhJPXXD8Q9Pzff8H/?format=pdf&lang=pt > Acesso em: 21/7/14.
MAYER, G. Trad: HOPKINS, M. Cap.2 – Imunologia. 2009. Disponível em: <http://pathmicro.med.sc.edu/portuguese/immuno-port-chapter2.htm>. Acesso em: 14/7/14.
MEDEIROS, C. Lúpus aumenta as chances de desenvolvimento de câncer. Correio do Estado, 2010. Disponível em: < https://correiodoestado.com.br/tecnologia/lupus-aumenta-as-chances-de-desenvolvimento-de-cancer/86327 >. Acesso em: 21/7/14.
MERCADO LIVRE. Anúncio: Acupuntura – Analyser Diagnóstico (Ryodoraku) – Cosmotrom. Acesso em: 5/9/14.
MOREIRA M.D. & MELLO FILHO, J. Psicoimunologia hoje. In J. Mello Filho (Org.), Psicossomática hoje (pp. 119-151). Porto Alegre: Artes Médicas, 1992.
NASCIMENTO, M.C. As duas faces da montanha: estudos sobre medicina chinesa e acupuntura. São Paulo, Hucitec: 2006.
NOGIER, R. e BOUCINHAS, J.C., 2006. Prática Fácil de Auriculoterapia e Auriculomedicina. Cap. 4: Detecção e Tratamento dos Pontos. 3ª Edição. Ed.: Ícone. P.: 31,32.
NÖTHLICH, B., 2006. Pulsologia Chinesa: o estudo moderno e a prática clássica. Disponível em: <http://acupuntura.pro.br/artigos/pulsologia-chinesa/>. Acesso em: 24/4/11.
OLIVEIRA, Paulo Marcos Agria – Tradução do original: Dorland’s Pocket Medical Dictionary. Dorland (Pocket) Dicionário Médico. 26 ed. – São Paulo: Roca, 2004. 1056p.
PINTO A.R., SILVA, B., OLIVEIRA, I.C., PEREIRA, J.O.S., NUNES, L.. Manual de normalização de trabalhos acadêmicos. Universidade Federal de Viçosa, 2011. Biblioteca Central. Disponível em: < http://pt.scribd.com/doc/ 72692510/31/ Figura-18-%E2%80%93-Modelo-de-anexo-ABNT-NBR-14724-2011>. Acesso em: 31/12/11.
REIS, E.C.F.B. et al.; EVARISTO, T.. Verdades e Mentiras sobre o Lúpus Eritematoso Sistêmico. Centro de Reumatologia do DF. Disponível em: <http://reumatologiadf.com.br/neosite/index.php/reumatologia-menu/dicas-reumato-me nu/48-verdades-e-mentiras-sobre-o-lupus-eritematoso-sistemico>. Acesso em: 21/7/14.
REQUENA, Y. Acupuntura e Psicologia. São Paulo: Andrei, 1990. P. 61-63.
SANTANTONIO, J., YAZIGI, L., SATO, E.. Adolescentes com Lúpus Eritematoso Sistêmico: Um estudo por meio do método de Rorschach. Psicologia: Teoria e Pesquisa. Mai-Ago 2004, Vol. 20 n. 2, PP 145-151. Disponível em: < http://www.scielo.br/pdf/ptp/v20n2/a07v20n2.pdf>. Acesso em: 15/mai/11.
SATO et al pela Sociedade Brasileira de Reumatologia. Lúpus eritematoso sistêmico: acometimento cutâneo articular. Rev. Assoc. Med. Bras. vol.52 nº6 São Paulo Nov./Dec. 2006. Disponível em: <http://www.scielo.br/scielo.php?script=sci_arttext& pid=S0104-42302006000600012>. Acesso em: 28/dez/ 11.
SATO, E. I; et al. Consenso brasileiro para o tratamento do lúpus eritematoso sistêmico (LES). Revista Brasileira de Reumatologia, 2002. P. 42(6), 362-370.
SCHEINBERG, M. Morton Scheinberg: A conquista do lúpus. Folha de S. Paulo. Opinião. 10/5/13. Disponível em: < http://www1.folha.uol.com.br/opiniao/ 2013/05 /1276223-morton- scheinberg-a-conquista -do-lupus.shtml>. Acesso em: 15/7/14.
SCOFIELD, R.H.; WINDLE, M.L.; RUSH, E.T.; BUEHLER, B.. Genetics of Systemic Lupus Erythematosus. Disponível em: < http://emedicine.medscape.com/article/1884 084-overview>. Acesso em: 7/7/14.
SCOTTO, C.M.. Relação com as Biomoléculas. Masterclin Treinamentos. Apostila: Acupuntura Auricular, 2006. p.3.
SILVEIRA, L.M.R. Acupuntura como tratamento auxiliar nas alterações comportamentais em cães.52 f. Monografia de Especialização em Acupuntura Veterinária. Instituto Qualittas. São Paulo, 2009.
SOBRINHO, R.B.. Dr. Nakatani. Ryodoraku = “sinal” do S.N.A. – 1950. Ryodoraku – Caminhos Permeáveis, p. 9. Apostila do Curso de Especialização em Acupuntura CBF/CEATA, 2007.
SOBRINHO, R. B. Manual EAV/Ryodoraku. Medchina, 2008.
SONTHEIMER, R.D.. Clinical manifestations of cutaneous lupus erythematosus. In: Wallace DJ, Hahn BH. Dubois’lupus erythematosus. Pennsylvania: Lea & Febiger, 1993. P.285-301.
SOUSA, J.L. e VASCONCELOS, E.B. Acupuntura Constitucional (Tipologia). Disponível em: <http://webcache.googleusercontent.com/ search?q=cache:JFpgrFlD Mu0J:www.portalunisaude.com.br/arquivos/CONSTITUCIONAL.pdf+hum+po+yi+zhi&cd=2&hl=pt-BR&ct=clnk&gl=br&source=ww w.google.com.br>). Acesso em: 21/4/ 11. S.d.
SOUZA, M.P.. Tratado de Auriculoterapia. Cap. 3. Diagnóstico. Brasília: LooK, 2001. P.: 31.
STEDMAN, T. L., 1990 (1853-1938). Trad.: ARAÚJO, C.L.C. et al., 1996. Stedman – Dicionário Médico 25ª Edição. Ed.: Guanabara Koogan. 1657p. P.: 746-748, 1376. Rio de Janeiro, 1990 Baltimore, USA.
TEIXEIRA, T. de M; COSTA, C. L. da. Papel da vitamina D no Lúpus eritematoso sistêmico. The role of vitamin D in systemic lupus erythematosus. Rev. Nutr. Vol. 25 nº4 Campinas Jul/Ago 2012.
TISKIEVICZ, F.. Perfil hormonal, marcadores imunológicos e atividade da doença em mulheres com lúpus eritematoso sistêmico, 2008. Tese de Mestrado da Faculdade de Medicina da Universidade Federal do Rio Grande do Sul. Programa de Pós-Graduação em Ciências Médicas: Endocrinologia.
UTIYAMA, S. R. da R; REASON, I. T. de M; KOTZE, L. M. da S. O sistema complemento nas doenças: genética e patogenia. The complement system in diseases: genetic and pathogeny. Revista Brasileira de Reumatologia, vol.44, nº 4, São Paulo, Jul/Ago, 2004. Disponível em: < https://www.scielo.br/j/rbr/a/ymRVJCGWVrJ3Dm5Mw8YbfVp/?format=pdf&lang=pt >. Acesso em: 7/7/14.
VILLAR, M. J. P., & SATO, E. I.. Estimando a incidência de lúpus eritematoso sistêmico em Natal/RN-Brasil. Comunicação apresentada na XVI Jornada Brasileira de Reumatologia e XIII Jornada do Cone-Sul de Reumatologia. Florianópolis, 2001.
WALLACE, D. et al. Tratamentos. Disponível em: <http://http://www.lupusonline.com. br/trata.asp>. Acesso em: 14/3/9. S.d.
WEN, T. S.. Conceito sobre os mecanismos da Acupuntura. Acupuntura Clássica Chinesa, p. 14 – 16. Cultrix, 2006.
WANG, B.. Cap 27 – Zhou Bi. Princípios de Medicina Interna do Imperador Amarelo. P.: 638. São Paulo: Ícone, 2001.
WD, 29/4/11. Prevalence Statistics for Types of Connective tissue disorders. Disponível em: <http://www.wrongdiagnosis.com/c/connective_tissue_disorders /prevalence-types.htm>. Acesso em: 7/5/11.
YAMAMOTO, T., YAMAMOTO, H. e YAMAMOTO, M. M., 2007. Cap 6 . Diagnósticos Abdominal e Cervical da Nova Craniopuntura de Yamamoto. Diagnóstico Abdominal da Nova Craniopuntura de Yamamoto. P. 3, 6, 70, 71, 72, 80. Ed.: Roca.
YAMAMURA, Y. Pontos de Acupuntura. Cap.3. Acupuntura Tradicional: A Arte de Inserir, p. 39. São Paulo: Roca, 1995.
YAMAMURA, Y., Introdução. Cinco Movimentos, a Natureza e o Ser Humano; Cap 16. Diagnóstico. Acupuntura Tradicional: A Arte de Inserir, p. L, 181, 182. São Paulo: Roca, 1996.
APPENDIX – FOOTNOTE REFERENCE
3. N.A.: Although Yamamoto (2007:72) recommends the use of disposable needles 25×40 mm, direct objection to its reuse is not made. During the research, several times the needles were changed, as needed and reused were sterilized.
4. N.A.: Despite the indication of several punctures on the same points (WANG, 2001) and Yamamoto recommend the use of pulsed wave, the researcher opted for the continuous wave. This is because the discomfort caused by this type of electrostimulation was great and, moreover, there is no evidence proving the ineffectiveness of the constant wave for the case.
[1] Acupuncture Specialist, academic in Production Engineering, graduated in Physiotherapy and also in Administration.
[2] Postgraduate professor and author of several books on Traditional Chinese Medicine and Avelar dos Santos, Orthomolecular Osteopath physician and Graduate Supervisor Lato Senso in Acupuncture.
Submitted: August, 2020.
Approved: April, 2021.















