REVIEW ARTICLE
BESSA, Vicente Alberto Lima [1], BESSA, Maria Fátima de Sousa [2]
BESSA, Vicente Alberto Lima. BESSA, Maria Fátima de Sousa. The electrolifting as an alternative in the treatment of stretch marks. Revista Científica Multidisciplinar Núcleo do Conhecimento. 04 year, Ed. 07, Vol. 11, pp. 67-78. July 2019. ISSN: 2448-0959
SUMMARY
Striae are acquired skin atrophies that arise when the elastic and collagen fibers rupture and form “scars”. They can cause an impact on the emotional state, in addition to the aesthetic damage. There are several types of treatments that can be employed by the beautician to treat stretch marks, among them: Electrolifting. Therefore, a bibliographic review study was carried out with the objective of investigating the morphofunctional benefits that can be obtained in the treatment of stretch marks by the application of electrolifting. And it can be inferred that the electrolifting improves the vascularization, increases the number of young fibroblasts expanding the synthesis of proteins, besides facilitating the migration of keratinocytes and macrophages, and has antioxidant and antidyslipidemic effect. These phenomena result in tissue repair and minimize the aspect of the stria.
Keywords: stretch marks, electrolifting, Microgalvanopunture.
1. INTRODUCTION
The World Health Organization in 1948 established a concept of health that has been in effect today. She considers that health involves the physical, mental and social well-being of the person (BRASIL, 1997). Although stretch marks do not generate a health threat, they can be psychologically distressing. (BERGFELD, 1999). Thus, the presence of stretch marks may pose a threat to the emotional integrity of the person and thus compromise self-esteem.
It is noteworthy that there are several procedures that can be used in the treatment of stretch marks, among them microdermabrasion, laser, carboxytherapy, radiofrequency, Vacuotherapy, peelings, percutaneous induction of collagen with the microneedling and Electrolifting (Moreira et al, 2013, MCCRUDDEN et al, 2015).
Nowadays, many seek to treat stretch marks and one of the procedures used is electrolifting, which promotes an inflammatory process that will stimulate the regeneration of tissues and thus soften the stretch marks and make them less perceptive. (SILVA, ROSA, SILVA, 2017).
Knowing that the electrolifting can be applied to treat people with stretch marks, arose the following problem situation: What will be the morphofunctional benefits that this procedure can promote.
2. GENERAL OBJECTIVE
- To investigate the morphofunctional benefits that can be obtained in the treatment of stretch marks by the application of electrolifting.
3. SPECIFIC OBJECTIVES
- Determine the causes of the appearance of stretch marks and their types.
- Describe the morphofunctional benefits promoted by Electrolifting when treating stretch marks.
- Identify electrolifting techniques that can be applied in the treatment of stretch marks.
4. JUSTIFICATION
Stretch marks are scars that form due to tissue lesions that produce an aesthetic aspect. This condition can generate a low self-esteem in the person, who feels the need to resort to medical, physiotherapeutic and aesthetic treatments.
Destarte, it is up to the aesthetician to elect the pertinent procedures to slow down the stretch marks, since besides the organic benefits it will be able to have psychological effects. There are several aesthetic treatments intended for this purpose, among them, the electrolifting that consists of the use of galvanic current applied through the active electrode that promotes a dermal microlesion. In this way, there will be localized tissue inflammation that may allow skin regeneration. (SILVA, ROSA, SILVA, 2017).
The present study was justified in that the use of electrolifting can represent an odd procedure in the treatment of stretch marks, minimizing organic disorders and, consequently, the psychological ones.
Therefore, this study can help to broaden the information concerning the employment and benefit of this type of treatment in person with stretch marks.
5. RESEARCH METHODOLOGY
The study will be based on explanatory bibliographic research, which can be characterized by being based on books and databases obtained in Europe PUC, Pubmed/Medline, Lilacs, Scielo, Scholar Google in the months of January to June 2019. For this purpose, we sought the keywords (descriptors): Stretch marks, electrolifting, Microgalvanopunture.
It will be explicative because it will “identify the factors that determine or contribute to the occurrence of phenomena” (Gil, 2007, p. 42).
Therefore, the study will seek to investigate the effects that electrolifting promotes in the treatment of stretch marks.
6. DEVELOPMENT
6.1 STRETCH MARKS: CONCEPTS AND INCIDENCE
The word stria vascularis originates in 1898, striae distensae, of Latin etymology can be translated into Portuguese as extended stria, but is commonly known only as Stria. (VAZIN, 2011).
The Stria is an acquired tegumentary lesion that generates a parallel linear atrophy, most often following the cleavage lines of the skin. There is a decrease in the activity of fibroblasts in the production of good quality extracellular matrix, in addition to rupture of existing fibers. This type of elementary skin lesion has a benign characteristic and its coloration varies according to the evolutionary phase. It represents an aesthetic alteration in the skin that can cause much discomfort and even low self-esteem and depression. (MAIA, 2011; VANZIN, 2011).
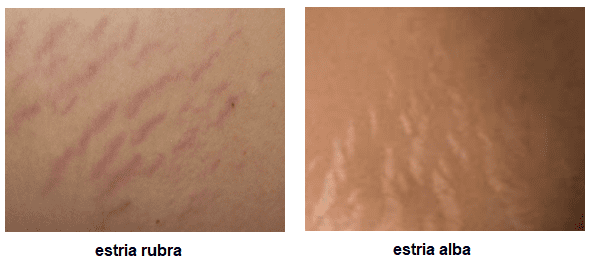
It is known that the stria has its color variation according to the time of evolution. In the beginning, it has a pinkish to reddish color and is therefore designated as a rubra stria (Stria rubrae), because it is an inflammatory response associated with vasodilation. With its evolution, the stria has a reduction of the microcirculation resulting in loss of collagen and elastic fibers and as a consequence, it presents a rough aspect and with whitish coloration and becomes known as Stria Alba. (AGNES, 2017).
Figure 1: Types of stretch marks.
It is noteworthy that stretch marks may appear in both sexes, but there is a higher incidence in women (60%) Compared to men (40%). (SAMPAIO, 2018). It is known that they are one of the most common alterations in body aesthetics and can affect 90% of women and 15% of men from 30 years of age. (GUIRRO e GUIRRO, 2004). They are also frequent in pregnant women.
6.2 STRETCH MARKS: ETIOLOGY
It is known that stretch marks are acquired Tegumental atrophies and its basic etiology is idiopathic, however, there are factors that contribute to its manifestation, and endocrine disorders are the most determinant. (WHITE et al, 2008). There are other authors who also emphasize endocrine factors as being the most determinant of the appearance of stretch marks, although they affirm that there is a lot of etiological indefinition and controversy. (BRAVIM e KIMURA, 2007).
However, there are three fundamental theories that try to explain the appearance of stretch marks, namely: the mechanical, endocrinological and infectious theory. (FACUNDO, 2014; WHITE et al, 2008; GUIRRO e GUIRRO, 2004).
The mechanical theory explains that the emergence of the stria would be due to excessive stretching of the tegument and this fact could rupture the skin and generate loss of elastic fibers. The main causes of skin stretching are obesity, growth rate at puberty, excessive muscular hypertrophy when practicing physical exercise, prolonged use of corticosteroids and Cushing’s syndrome. (FURLANI et al, 2010). Another common factor is the mechanical stretching of the skin during pregnancy. (MAIA et al, 2009).
The endocrinological theory explains that the appearance of the stria may be related to hormonal dysfunction. It is known that the steroid hormone interferes in the action of fibroblasts and its imbalance is present in all forms of appearance of stretch marks during the adolescence, pregnancy and obesity phase. (BRAVIM e KIMURA, 2007; BONETTI, 2007; GUIRRO e GUIRRO, 2004).
It is noteworthy that stress hormones, adrenaline, noradrenaline, adrenocorticotrophic hormone and glucocorticoids are also pointed out as triggers of stretch marks associated with stressful physical activity, as well as only states Stressful. (GUIRRO e GUIRRO, 2004).
The infectious theory is poorly defended in the literature, however there are some adherents who believe that infectious processes can generate data in the elastic fibers. This fact would explain the appearance of striae in young people with rheumatic fever, typhoid, chronic liver diseases and Marfan syndrome. (FURLANI et al, 2010).
It is believed that stretch marks can also have genetic influence where the expression of the determinant genes 24 for the formation of collagen, elastin and fibronectin would be diminished in people with atrophic striae. (FACUNDO, 2014).
Another important fact that predisposes the appearance of stretch marks is skin dehydration, since the drier skins are more prone to stretch marks. (VANZIN, 2011).
There is very little study concerning the pathophysiology of skin striae and most researches have prioritized the etiological factors and treatment procedures to the detriment of the development of the disease. It may be that the difficulty in conducting laboratory studies explains the scarcity of research on stretch marks. (CORDEIRO; MORAES, 2009).
Stretch marks are installed when there is a cutaneous degeneration as a consequence of decreased fibroblast activity in the production of extracellular matrix and subsequent interruption of continuity of existing fibers. It is known that when comparing with healthy skin, the skin with Stria has less amount of fibrilin, collagen and elastin. In addition, the skin with Stria has altered coloration due to dysfunctions of the activity of melanocytes and the microcirculation and the defense reactions of the organism. When the stria has a recent inflammatory reaction due to excessive stretching of the skin that breaks both the skin and the capillaries is called rubra or rosy Stria. In this case, there may be pain and even intense itching. On the other, the Albas or white or pearl stretch marks have in addition to the rupture of the elastic and collagen fibers, fibrotic lesions, dysfunction in the sweat and sebaceous glands and in the development of the hairs. They can still be atrophic striae that have disorganization of the fibers, a hypochromic characteristic, yet with preservation of the skin attachments. (BRAIT, 2018).
6.3 ELECTROLIFTING: MORPHOFUNCTIONAL BENEFITS
It is known that the unaesthetic aspect that stretch marks generate can cause emotional impacts, in addition to physicists and therefore, many seek for aesthetic treatments to minimize and even prevent the appearance of stretch marks.
It is imperative to resave that there is a cosmetological arsenal and various equipments that in an isolated or associated way are used to treat people with stretch marks and among them, the electrolifting.
Electrolifting is a treatment procedure that was developed by the French dermatologist Humberto Pierantoni, in 1952, to fill grooves and stretch marks. This technique is also known as Galvanopunture or Microgalvanopunture and consists of a technique that uses galvanic current in the order of some microamps (µA), that is, microgalvanic, and the electrode with or without the needle (active electrode) always should be connected to the negative pole. Pierantoni observed that electrical stimulation allowed the attenuation of grooves and stretch marks. (DAL GOBBO, 2010).
It is known that the electrolifting has its physiological effects distributed in four phenomena: electrochemical, osmotic, vasomotor and alteration in cellular excitability. (Bragato, Fornazari e Deon, 2013). Skin stimulation will promote active hyperemia and increase the quantitative number of young fibroblasts, promote the migration of keratinocytes and macrophages and develop neovascularization and thus regenerate the subepidermal tissue. (DAL GOBBO, 2010).
This technique can be obtained through a galvanic current that will generate an inflammatory process in the skin and stimulate a tissue regeneration, because the trauma promoted by the needle along with the electric current promotes the increase of the metabolism to Recomposition of collagenous tissue, which may fill the treated area. (SILVA, ROSA e SILVA, 2017).
It is known that the electrolifting should cause a small lesion in the skin that will result in edema and hyperemia that arise due to the release of chemical mediators vasodilators. The lesion is filled by an inflammatory exudate merged with leukocytes, erythrocytes, plasma proteins and fibrin fascias. The epithelialization of the injured area is simultaneous and, thus, epidermal cells invade the site in which the insertion of the needle or the tip was made. One of the phenomena that stimulate the invasion of epidermal cells is the formation of fibrin originated by the hemorrhage of the microlesion. There will also be an increase in the number of young fibroblasts in the region, in addition to a new microcirculation and the return of pain sensitivity due to tissue repair that can close the stretch marks and give a better appearance of the skin. (SANTOS e OGATA, 2012).
In a master’s thesis in Cellular and Molecular biology performed at the Pontifical Catholic University of Rio Grande do Sul entitled “Treatment of Albic stretch marks with galvanopunture: beneficial for aesthetics, oxidative stress and lipid profile” if it can To verify the benefits of this treatment. The study consisted of applying electrolifting in the gluteus of 32 volunteers with an average age of 25 years, once a week over a period of ten weeks. Venous blood was collected before and after the sessions and was performed to analyze the plasma concentrations of CRP, TNF-α, NO, TBARS, oxiated LDL-C, HDL-C, total cholesterol, CAT and uric acid. The result of the biochemical analysis of the blood samples determined that the galvanopunture does not induce any systemic inflammatory process, but remarkably decreases the oxidative stress. Since the analysis of plasma concentrations found that the total cholesterol concentration was not altered, while HDL (high density lipoproteins) increased and the oxidation of LDL (low density lipoproteins) decreased, i.e., There was the protection of plasmatic lipids from the oxidative lesion without systemic inflammatory response. Therefore, the data presented in the study indicated that electrolifting has an antioxidant and antidyslipidemic effect. (BITENCOURT, 2007).
There are studies that report satisfactory results in the treatment of stretch marks with the use of electrolifting. One of these studies was carried out in order to evaluate the effects of microneedling in relation to microgalvanopunture in the treatment of atrophic striae. For this purpose, an uncontrolled quasi-experimental study was conducted, in which 10 volunteers with ages ranging from 20 to 44 years with Atrophic Striae participated. A photographic evaluation and a classical and digitized planning were performed, in addition to a subjective questionnaire for the analysis of the sensation of improvement. The volunteers were treated 1 time per week for 4 months and received the microgalvanopunture techniques on the right side and microneedling on the left side. The study concluded that there was improvement with both techniques and no significant difference between them and the satisfaction of the volunteers. (SILVA, ROSA, SILVA, 2017).
Another study titled “Comparative between Galvanopunture and Microneedling” had as general objective to evaluate the effect of galvanic current and microneedling. To compare the microneedling was applied to treat stretch marks on the right gluteus and electrolifting in the left gluteus of only one volunteer, 31 years with Phototype IV and without having undergone aesthetic interventions in the area. The study was qualitative and was performed at the Universidade Tiradentes, Aracaju-SE. The volunteer signed the Informed consent form and underwent an anamnesis, in addition to having been photographed in the region before and during the treatment evolution. For the application of Galvanopunture was used the Neurodyn Esthetic, Ibramed with intensity of 100, µA and with the technique of piercing the epidermis straight in the direction of the stria lifting it for 3 seconds and with weekly treatment. For the microneedling the FDR Derma Roller with 540 needles of 0.5 cm with the technique of 15 vertical movements, horizontal and right and left diagonals, being the treatment performed twice a month in a total of four sessions. The study concluded that the galvanopunture was more efficient when compared to the microneedling, because in the second session there was an improvement in the appearance of the Stria, but the fifth session the evolution was stagnoed. With the microneedling, no difference was found in the stretch marks. (SILVA et al, 2016).
It is known that the treatment of Albas stretch marks requires more aggressive intervention, such as electrolifting. In order to evaluate the efficacy of electrolifting in the improvement of the appearance and sensitivity of albas stretch marks of the gluteal region, a quasi-experimental study was carried out in volunteers. The study was approved by the Research Ethics Committee of the Faculty of Medical Sciences of Minas Gerais and the volunteers signed the Informed consent form. The six healthy volunteers were aged between 18 and 28 years with Phototypes II, III and IV and were submitted to an evaluation through an interview and a questionnaire adapted by Guirro to evaluate the stretch marks. They were exposed to one session per week for a total of six weeks lasting thirty minutes. The device used was STIMULUS FACE of the HTM brand and the puncture was performed with a disposable needle of three millimeters and with intensity of 150 µA in the first two sessions and 100 µA in the following four. It was found that 34% of the sample did not have significant improvement and 66% obtained moderate to accentuated improvement in the appearance of the stretch marks. As for the pain scale, an improvement in sensitivity was confirmed through evaluation with a stadiometer and as to the degree of satisfaction, 83.3% of the volunteers were satisfied or very satisfied with the treatment. It can be inferred that the electrolifting promoted a satisfactory treatment and as improvement in the visual aspect of the stretch marks, besides improving the local sensitivity. (COSTA e SILVA, 2018).
A randomized clinical trial with blinting titled “Comparative Study between Galvanopunture and scarification in the treatment of white atrophic striae in women between 20 and 25 years” was approved by the Ethics committee in UniSALESIANO and Submitted to the Brazil platform of the Ministry of Health and aimed to verify the effects of galvanopunture techniques and scarification in the treatment of white atrophic striae. This experiment was carried out with six volunteers aged between 20 and 25 years who had white striae in the gluteal region in the body and Essence Clinic in the city of Lins/SP for three months. The follow-up was done through inspection and palpation, photographic records before and after treatment. The volunteers were divided into two groups: Galvanopunture Group and scarification Group. The Galvanopunture group performed 8 treatment sessions with the Ibramed brand Striat, with an intensity of 160 µA and sterile needles. The Scarification group was performed by the superficial scraping technique throughout the length of the stretch marks, in order to provide local inflammation and posterior skin repair. This group was submitted to 8 sessions, but 2 volunteers only received 5 sessions, because they had intercurrences during the treatment. The result of the research highlighted that galvanopunture was more effective than scarification, because the latter resulted in limitations that interfered in the research timeline and in the results. (PEDRO, AUGUSTO e OLIVEIRA, 2015).
The monograph “Use of electrolifting and carboxytherapy for stretch mark treatments” aimed to contextualize the action of Electrolifting and Carboxytherapy and as physiotherapeutic resources for the treatment of stretch marks. This study was developed through a bibliographic review and allowed the conclusion that both electrolifting and carboxytherapy cause effective effects in the treatment of stretch marks. (FACUNDO, 2014).
Another monograph called “Main methods for aesthetic treatment of stretch marks” aimed to analyze which aesthetic procedures most reported in the literature to treat stretch marks, discuss the advantages of these procedures and the methods of greater Choice. This study was conducted through a literature review that addressed as aesthetic procedures galvanopunture, microdermabrasion, chemical peeling, use of cosmeceuticals, organic silicon and Hydroxyproline-methylsilanol aspartate. The author concluded that the Stria has its appearance improved in relation to its thickness/width and coloration when the person is subjected to galvanopunture, microdermabrasion and peels associated with the use of cosmeceuticals. He reported that the techniques cited may also be associated with chemical peeling and it is the professional to evaluate and indicate the most appropriate treatment. (COSTA, 2016).
Another study that purchased the efficacy of Electrolifting was performed with a volunteer of 30 years, sedentary, nulífor, light brown skin, without history of cardiopathy and who used oral contraceptives. The technique was applied in 10 sessions in the Lumbosacral region with the STRIAT apparatus (IBRAMED). On the right side was applied the puncture technique with the current passing and on the other side applied the puncture with the equipment turned off, ie, not passing any type of current. The photographic records confirmed the improvement of the visual aspect of the stria on the side treated with the current passing. (GALDINO, DIAS e CAIXETA, 2010).
The study “use of electrolifting to improve the appearance of the skin” aimed to analyze by means of bibliographic review the effect of the use of electrolifting on the skin. After the analysis of 20 articles, it was possible to contact that seven articles reported the benefits for cell renewal, activation of collagen and elastin, relaxation of the depth and length of the rhytides and lines of expression, thus providing greater Self-esteem and quality of life of customers. Another eleven studies have added that electrolifting causes partial or total dissimulation of the Rhytides and eleven articles affirmed that the electrolifting is an excellent treatment of stretch marks. Two articles do not associate the Electrofacelift with the use of cosmetics, but other nineteen did and affirmed that the association would improve the overall appearance of the skin. (OGLIARI et al, 2016).
An exploratory, experimental, quantitative and qualitative study was developed on two electrolifting protocols for the treatment of albas streaks that emerged during the gestational period using the microgalvanic current and verifying Its effects. Participants were 26 volunteers aged between 20 and 35 years. The participants were divided into two groups and did 15 sessions with 12 days of interval between them and with intensity of 100 µA. Group A was treated by longitudinal puncture and group B by transverse puncture. As an evaluation criterion, the questionnaire was answered about pain intensity, type of pain and satisfaction with treatment, and a physiotherapeutic evaluation was performed at the beginning, after the fifth, tenth and fifteenth session. The stretch marks were photographed and their area, length and width were analyzed using the ImageJ software, manual planimetry and Pachymetry. It is good to emphasize that group A had significant improvement in only 5 sessions while group B took 15 sessions to present similar results. However, the result at the end of treatment was similar in reducing the size of the stretch marks and the degree of satisfaction. (SILVEIRA, 2016).
6.4 ELECTROLIFTING: TECHNIQUES
The treatment is done with the use of an apparatus (Figure 2) that produces galvanic current with microamperage employing two types of electrodes: a negative, pen type, which will come into direct contact with the area to be treated and another positive, rubber and sponge , which will close the electrical circuit. (DAL GOBBO, 2010). Therefore, there is no need for the customer to remove metallic objects during treatment, such as: rings, clocks, earrings or bracelets. (BAENA, 2003 apud FACUNDO, 2014).
Figure 2: Models of apparatus that allow the application of electrolifting.

The application of electrolifting can be divided into two main techniques: one using the electrolifting tip (Figure 3) and the other using the disposable sterile needle (Figure 4).
Figure 3: Electrolifting tip.
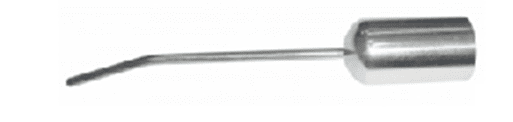
Figure 4: Electrolifting needle.
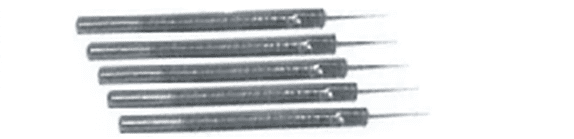
In the first technique, the needle electrolift is used (Figure 5) and is much more aggressive and in this case always use a sterile disposable needle instead of the electrolifting tip. This needle should be thin, sturdy and pointed, constructed in stainless material and with a maximum length of 4 mm in order to penetrate easily into the skin. (BORGES, 2010).
The second technique uses a sterile electrolifting tip (Figure 6) fixed to the pen that corresponds to the negative electrode (active) and should be scratched to the logo of the entire affected region until there is hyperemia. The positive (passive) electrode should be close to the region to be treated to close the electric field. This technique is less aggressive and more tolerable by customers.
Figure 5: Electrolifting with needle.
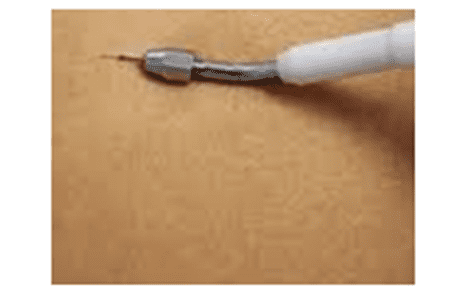
Figure 6: Electrolifting with ferrule.
There are 3 modalities of application, namely (DAL GOBBO, 2010; GUIRRO and GUIRRO, 2004 Apud FACUNDO (2014):
- Punctual or puncture is the introduction of the needle into adjacent points and within the stria and the needle penetration cannot be repeated at the same point. Besides it gives a minimum interval of 15 days for new application in the area.
- Sliding consists of sliding the needle parallel to the stria and the treatment may be weekly;
- Scarification, the needle will be slipped (scratched) in the stretch marks, but should be positioned at 90 degrees, causing a tissue injury. (REBONATO et al, 2012).
There are professionals who divide the technique of application of electrolifting with needle in four forms of application. (RUSENHACK, 2004):
- Punctiform or puncture, and the needle should be inserted in the skin vertically in the stria in the entire extension of the groove with depth of close to 1 mm. This technique has been considered the most advisable, although it is uncomfortable and several needle inserts are made in the same stria. (MEYER et al, 2009);
- In a linear way the needle is introduced obliquely to the stria with circular lifting movements and with depth of about 2 to 3 mm;
- Angularly or “fish scale”, in this case the needle is inserted on the edges of the stria, alternating the sides in an oblique way, being optional the lifting of the skin;
- Cross-sectional, in which the needle will need to lift the entire surface of the stria, going from one edge to the other of the skin, without, however, entering below the epidermis. The permanence of the elevation of the skin for about 2 seconds will increase the desired response.
It is good to emphasize that the techniques may be applied alone or associately depending on the depth, extent, texture of the skin and area to be treated.
It is necessary to emphasize that the electrolifting employs a reduced intensity current to microamperage and the smaller the electrode size, the lower the maximum tolerable intensity and vice versa. (BORGES, 2010). There is no consensus on the intensity of the electrolifting application and this fact can be proven when analyzing table 1, which was one of the results of the master’s thesis in biomedical engineering professional of the graduate program in Biomedical Engineering, Federal Technological University of Paraná. In table 1 The intensity varies from 50 to 150 microamps. (SILVEIRA, 2016).
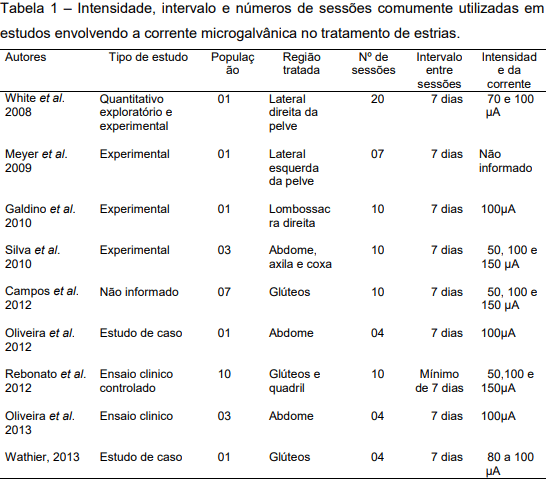
However, it is known that the optimum intensity for treatment of stretch marks ranges from 70 to 100 µA, but varies according to the client’s sensitivity. (GUIRRO e GUIRRO, 2004). However, the intensity of current prescribed in practice, from the current literature, can range from 50 to 100 µA when applying the puncture or up to 150 µA in the scarification technique. (SILVEIRA, 2016).
The intensity may also vary according to skin dysfunction, and for the treatment of stretch marks is between 70 and 100 microamps and for Rhytides is 150 to 200 microamperes, however, it is reiterated that the intensity values will vary according to the sensitivity of C Client. (BORGES, 2010). It is noteworthy that the intensity of the microcurrent is determined by the sensitivity of the client, therefore, it must respect the pain threshold of the client. (SILVEIRA, 2016). Therefore, the beautician should test each area to be treated to make sure of the customer’s tolerance, because each region of the body may have different level of current sensitivity. (DAL GOBBO, 2010).
For some physiotherapists the intensity should not be greater than 300 µA in order to prevent possible lesions or stains on the skin due to the intense action of the galvanic component. (BROGES, 2010). There are those who recommend that better results can be achieved with intensities between 150 and 300 µA. (AGNES, 2017).
It is known that this type of electrotherapy has a low-intensity continuous current (microampéres), so there is no systemic inflammatory effect, both acute and chronic, during treatment. This fact was evidenced by studies and blood tests that measured the markers of systemic inflammation, plasma levels of TNF-α and CRP, before treatment, 24h after the first session (Day 1), before the last session (Day 70) and 24h after the last session (day 71) of 32 Volunteers between 20:30 years with Alba stretch marks in the gluteal region. The study concluded that there were no significant differences in these inflammatory parameters. The multifaceted inflammatory mediator, nitric oxide, presented a discrete but not significant decrease after the first 24 h. (BITENCOURT, 2007).
However, people with alipic skin may present absence of current sensitivity during the first sessions, since the resistance of the skin to the current passage is increased. (GUIRRO e GUIRRO, 2004; BARBOSA e CAMPOS, 2013).
In order to obtain a favorable result, a prior evaluation is necessary to determine the type of stria, size of the stria, skin thickness, skin color, age and exclusion of contraindications, and in this way it can be determined the number of sessions and the intensity of the current. However, it is good to stress that this type of treatment does not yet have a specific protocol in relation to the stimulus, frequency, intensity, time and sequence of treatment. (GUIRRO e GUIRRO, 2004).
Before applying the electrolifting, the area to be treated should be sanitizer, so it is possible to use soap and water for removal of impurities or even the high frequency apparatus with the electrodes cebolão, scallions or rolls. (DAL GOBBO, 2010).
After the application of the electrolifting, it is necessary to keep the skin well hydrated, and to control the oiliness in order to better the response of tissue repair. It is good the use of night depigmenting and sunscreen with FPS above 30 throughout the day, reapplied it every 3 hours. It is important that after treatment avoid sun exposure to prevent the formation of hyperchromies, even if using sunscreen. It can be applied after immediate treatment of antioxidant cosmetics such as vitamin C and growth factors in order to stimulate collagen production. (SILVA et al, 2018).
The electrolifting improves the appearance of the stria, because it decreases the thickness/width and coloration and can avoid the emergence of new stretch marks. It can be applied alone or in association with other treatment techniques, such as: Microdermabrasion and peels associated with the use of cosmeceuticals. (JUNIOR et al, 2013).
However, there are professionals who do not recommend the association of Electrolifting to other aesthetic treatments, because they affirm that it can generate an anti-inflammatory action, however they recommend the use of sunscreen to prevent dyschromies in the skin (BORGES, 2006 Apud SILVA et al, 2018).
However, the response to treatment varies from person to person, as it will depend on the age, gender, physical and nutritional conditions, type and degree of stria, however it is known that the most recent striae will respond better to the treatment.
There are professionals who recommend that the sessions for treatment of stretch marks should have intervals of one week between applications and that the results can be observed between five to fifteen sessions. (BROGES, 2010). The current literature recommends that the interval between sessions may vary from two to seven days. (WHITE et al, 2008; OLIVEIRA, 2013). However, it is not advisable to repeat the treatment before the entire inflammatory process is reabsorbed.
It should be emphasized that the professional who will prescribe the electrolifting should be qualified to apply it in compliance with all the biosafety norms and know how to guide customers regarding Homecare conducts.
6.5 ELECTROLIFTING: INDICATIONS AND CONTRAINDICATIONS
Electrolifting is advised for the treatment of stretch marks, rhytides and expression marks. On the face, it is indicated to decrease the lines of expression, Nasogenian grooves, ritides in the Glabela, Periocular and in the frontal region, typical of the aging process. It is also indicated to obtain the drug delivery effect which consists of the permeation of drugs in the skin through this technique. The cosmetological assets can be associated after the application of the electrolifting, however one should have a good knowledge of the substance used, because it can not contain any anti-inflammatory action to not annul the benefits of treatment.
In addition to the aforementioned indications, electrolifting can also be recommended in hydration treatments; Nutrition and revitalization; Seborrhea and edema. (OLIVEIRA, 2014 apud SILVA et al, 2018).
The main contraindications are the same for most electrotherapeutic treatments, such as: Pregnant women, people with diabetes, neoplasms, pacemaker carriers, heart problems and epilepsy. It is also not suitable for people with haemophilia, vitiligo, Cushing’s syndrome, tendency to keloids and the use of steroid-based medications and corticosteroids. (VENTURA, 2003; BORGES, 2010).
In addition to pregnant women, the treatment of electrolifting after childbirth is also not indicated, and the normal return of hormonal levels prior to pregnancy should be respected (AGNE, 2017).
As there are not enough studies to indicate the use of electrofacelift during puberty, it is recommended that it is not used because it is a period of major hormonal changes. Some authors also believe that it may be one of the etiologies of the appearance of stretch marks. (WHITE et al, 2008; BORGES, 2010).
The fact that there are no defined protocols concerning the type of stimulus, frequency and optimum intensity, time and treatment sequence has limited the treatment of stretch marks. The best result could be obtained with the interaction of the methods and with defined protocols. However, even without defined protocols, it is appropriate to ensure that the use of electrolifting brings evident improvements to the aspect of the treated skin. (MATOS; COSTA, 2019).
7. FINAL CONSIDERATIONS
The electrolifting apparatus is used in the treatment of stretch marks and other skin alterations. Since the stria is a type of acquired tegumentary atrophy and has idiopathic etiology, but some theories have been sustained, such as: Mechanical, endocrinological and infectious. In addition, they can be classified into Rubras and Albas streaks and both can be subjected to aesthetic treatment.
Electrolifting is a procedure that treats stretch marks and allows for unmatched benefits, such as: neovascularization, broadens the number of young fibroblasts increasing protein synthesis, besides facilitating the migration of keratinocytes and macrophages, has an effect Antioxidant and antidyslipidemic that results in tissue repair and minimizes the appearance of the stria.
The application techniques are two: one uses the electrolifting tip, being the least used and the other using the needle of about 4 mm. The application of the needle can be done in a punctual way, by sliding and by scarification. The studies referenced in this study showed no significant difference between the four techniques of application with the needle, but there is less efficacy when the electrolifting tip is employed.
The indication of electrolifting is to treat different types of stretch marks, but it is also indicated for treatments of hydration, nutrition and revitalization, seborrhea, edema, rhytides, expression marks and drug delivery effect.
The contraindications follow the same of other electrotherapeutic procedures, that is, should not be applied in diabetic, epileptic, people heart problem and cardiac pacemaker, sensitivity disorders, person with cancer, pregnant woman, haemophilia , vitiligo, Cushing’s syndrome, tendency to keloids, and the use of steroid-and corticosteroid-based medications.
It is concluded that electrolifting can add value to aesthetic and physiotherapeutic procedures, while it is not the only procedure to be employed, but part of a set of therapeutic strategies. It was observed the lack of updated studies concerning the topic approached and it is recommended that new studies be implemented to verify other aplicabilities of this therapeutic and aesthetic resource.
REFERENCES
AGNE, J. E. Eletrotermofototerapia. 4. ed. Rio Grande do Sul: Editorial Santa Maria, 2017.
BARBOSA, D. F.; CAMPOS, L. G. Os efeitos da corrente galvânica através da técnica de eletrolifiting no tratamento do envelhecimento facial. Revista Inspirar, Movimento & Saúde, v.4. n.1. ed. 22. jan./fev., 2013.
BERGFELD, W.F. A lifetime of healthy skin: implications for women. International Journal of Fertility and Women’s Medicine, v.44, n.2, p.83-95. mar/abr,1999.
BITENCOURT, S. Tratamento de estrias albas com galvanopuntura: benéfico para a estética, estresse oxidativo e perfil lipídico. 2007. 38 f. Dissertação (Mestrado em Biologia Celular e Molecular). Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, 2007.
BONETTI, V. B. Incidência de estrias em acadêmicos da Faculdade Assis Gurgacz, identificando sua principal causa. Cascavel, 2007. Monografia (Graduação em Fisioterapia). Disponível em: https://pt.scribd.com/document/245108173/Incidencia-de-Estrias-Em-Academicos-Da-Faculdade-Assis-Gurgacz-Identificando-a-Sua-Principal-Causa. Acesso em: 01 abr. 2019.
BORGES, F. S. Dermato-funcional: modalidades terapêuticas nas disfunções estéticas. 2. ed. São Paulo: Phorte, 2010.
BRAGATO, P.E.; FORNAZARI, L.P.; DEON, K.C. Aplicação de eletrolifting em rugas faciais: relato de caso. Revista UNIANDRADE, v.14. n.2, p.131-143, 2013.
BRAIT, D. C. et al. Microagulhamento associado a fatores de crescimento e vitamina C no tratamento de estrias, fibroe dema geloide e flacidez tissular na região glútea. Fisioterapia Brasil, v.19, n.1, p.80-88, 2018.
BRASIL. Saúde da Família: uma estratégia para a reorganização da atenção básica. Brasília-DF, 1997.
BRAVIM, A. R. M., KIMURA, E. M. O uso da eletroacupuntura nas estrias atróficas: uma revisão bibliográfica Brasília, 2007. Disponível em: http://www.portalunisaude.com.br/downloads/eletroacupuntura_nas_estrias.pdf. Acesso em: 01 abr. 2019.
CORDEIRO, R.C.T.; MORAES, A.M. Striae distensae: fisiopatologia. Surgical & Cosmetic Dermatology, v.1, n.3, p.137-140, 2009. Disponível em: <http://www.surgicalcosmetic.org.br/exportar-pdf/1/1_n3_31_pt/Striae-distensae–fisiopatologia> Acessado em: 02 abr. 2019.
COSTA, P.H.V.; SILVA, F.S. Efetividade da corrente galvânica/eletrolifting no tratamento de estrias albas na região glútea. Revista Interdisciplinar Ciências Médicas, Belo Horizonte, Minas Gerais, v2. n.2., p.14-21, 2018
COSTA, R. S. Principais métodos para tratamento estético de estrias. 2016. Monografia (Pós-graduação em Lato Sensu em Biomedicina Estética). INESP e Centro de Capacitação Educacional, Recife – PE.
DAL GOBBO, P. Estética facial essencial: orientações para profissional de estética. São Paulo: Atheneu, 2010.
FACUNDO, D. R. Utilização do eletrolifting e da carboxiterapia para tratamentos de estrias. 2014. Monografia (Graduação em Fisioterapia). Faculdade de Educação e Meio Ambiente, Ariquemes – RO.
FURLANI, L. A. et al. Estrias: fator de risco para distopia urogenital?. Surgical Cosmetic Dermatology, v.2, n.1, p.18-22, 2010. Disponível em: <http://www.surgicalcosmetic.org.br/detalhe-artigo/49/Estrias–fator-de-risco-paradistopia-urogenital>. Acesso em: 01 abr. 2019.
GALDINO, A. P. G.; DIAS, K. M.; CAIXETA, A. Análise comparativa do efeito da corrente microgalvânica: estudo de caso no tratamento de estrias atróficas. Revista Eletrônica “Saúde CESUC”, n.1, 2010.
GIL, A. C. Como elaborar projeto de pesquisa. 4 ed. São Paulo: Atlas, 2007.
GUIRRO, E.C.O.; GUIRRO R.R.J. Fisioterapia dermato-funcional: fundamentos, recursos, patologias. 3. ed. rev. e ampl. São Paulo: Manole, 2004. 560 p.
JUNIOR, A. A. S. et al. Estrias: fisiopatologia, principais tratamentos estéticos. [2013?]. Disponivel em: <https://semanaacademica.org.br/system/files/artigos/estrias_fisiopatologia_principais_tratamentos_esteticos.pdf> Acesso em: 17 abr. 2019.
MAIA, M et al. Estrias de distensão na gravidez: fatores de risco em primíparas. Anais Brasileiros de Dermatologia. Rio de Janeiro, v.84, n.6, p.599-605, 2009.
MAIA, M. Tratado de medicina estética. 2. ed. São Paulo: Roca, 2011.
MATOS, D. M. R.; COSTA, K. L. C. Estrias X recursos fisioterápicos: revisão. Revista Científica Multidisciplinar Núcleo do Conhecimento. a.4, ed.5, v.6, p.05-20, maio 2019.
MCCRUDDEN, M.T. et al. Microneedle applications in improving skin appearance. Experimental Dermatology, abr., 2015. Disponível em: <https://onlinelibrary.wiley.com/doi/full/10.1111/exd.12723> Acesso em: 9 jan. 2019.
MEYER, P.F. et al. Aplicação da galvanoterapia em uma máquina de tatuar para tratamento de estrias. Revista Fisioterapia Brasil, v.9. 2009.
Moreira et al. A Fisioterapia Dermato-funcional no tratamento de estrias: Revisão de literatura. Revista Científica da UNIARARAS, Araras – SP, v. 1, n. 2, 2013. Disponível em: <http://www.uniararas.br/revistacientifica/_documentos/art.3-008-2012.pdf >. Acesso em: 09 jan. 2019.
OGLIARI, M. et al. Uso do eletrolifiting para melhorar a aparência da pele. In: Congresso Brasileiro Interdisciplinar na Promoção da Saúde. 2016. Disponível em: https://online.unisc.br/acadnet/anais/index.php/CBIPS/article/view/15917. Acesso em: 02 fev. 2019.
OLIVEIRA, E. L. Efeito da corrente microgalvânica invasiva em estrias albas: estudo histopatológico. Dissertação (Mestrado em Fisioterapia). Universidade Metodista de Piracicaba – Faculdade de Ciência da Saúde. Piracicaba, 2013.
PEDRO, C. F. P.; AUGUSTO, L. C. S.; OLIVEIRA, L. M. Estudo comparativo entre a galvanopuntura e a escarificação no tratamento das estrias atróficas brancas em mulheres entre 20 e 25 anos. Universitári@ – Revista Científica do Unisalesiano, Lins – SP, a.6, n.13, jul-dez, 2015.
REBONATO, T.A. et al. Aplicação de microgalvanopuntura em estrias cutâneas albas. Revista Movimento e Saúde, v.4. p.1-6, 2012.
RUSENHACK, C. Terapia por microgalvânica em dermato-funcional. Fisio & Terapia, Rio de Janeiro. n.8. p.24-26. 2004.
SAMPAIO, S. A. P. Dermatologia de Sampaio e Rivitti, 4. ed. São Paulo: Artes Médicas, 2018.
SANTOS, M.S.; OGATA, G. O uso da galvanopuntura no tratamento das estrias atróficas: uma revisão bibliográfica. 2012. Disponível em: <http://portalbiocursos.com.br/ohs/data/docs/19/66_-_O_uso_da_galvanopuntura_no_tratamento_das_estrias_atrYficas.pdf>. Acesso em: 20 maio 2019.
SILVA, C. L. C. et al. Comparativo entre galvanopuntura e microagulhamento. A prática interdisciplinar alimentado a ciência. In: 18ª Semana de Pesquisa da Universidade Tiradentes. 24 a 28 out., 2016. Anais… Aracaju, Sergipe: Universidade Tiradentes/Estética e Cosmética, 2016.
SILVA, M. L.; SILVA, V. G.; ROSA, P. V. Análise dos efeitos da utilização do eletrolifting e do microagulhamento no tratamento das estrias atróficas. Revista Biomotriz, Rio Grande do Sul, v.11, n.1, abr., 2017.
SILVA, T.M. et al. Tratamento de estria Alba com o uso de eletrolifting. Revista Terra e Cultura: cadernos de ensino e pesquisa, Centro Universitário Filadélfia. Londrina, PR, v. 33, NESP 67, jun. 2018.
SILVEIRA, C. F. C. Utilização de corrente microgalvânica para o desenvolvimento de dois protocolos para tratamento de estrias albas. 2016. 109 f. Dissertação (Mestrado em Engenharia Biomédica). Programa de Pós-Graduação em Engenharia Biomédica, Universidade Tecnológica Federal do Paraná. Curitiba, 2016.
VANZIN, S. B.; CAMARGO, C. P. Entendendo Cosmecêuticos: diagnósticos e tratamentos. São Paulo: Santos, 2011.
VENTURA, D. B. S. O uso da corrente galvânica filtrada nas estrias atróficas. Revista Fisiobrasil: atualização científica, n. 62, nov/dez 2003.
WHITE, P.A.S. et al. A. Efeitos da galvanopuntura no tratamento das estrias atróficas. Revista Brasileira de Fisioterapia, Rio de Janeiro, v.9, n.1, p.53-58, jan/fev. 2008.
[1] Master in Human motricity Sciences; Specialization in Dermato-functional physiotherapy; Specialization in sports training and Personal Trainner; Specialization in medical gymnastics; Specialization in Portuguese language specialization in advanced topics in physiotherapy; Specialization in innovative teaching of higher education; Graduated in physiotherapy; Technologist in aesthetics and cosmetics; Bachelor and graduate in Physical education; Licensed in letters; Graduated in pedagogy.
[2] Master in Human motricity Sciences; Specialization in medical gymnastics; Graduated in physiotherapy; Bachelor and graduate in Physical education.
Submitted: June, 2019.
Approved: July, 2019.















