ORIGINAL ARTICLE
SILVA, Carlos Eduardo Gomes Da [1]
SILVA, Carlos Eduardo Gomes Da. Dimensioning of the staff of the municipal hospital, Outpatient and UPA of the Municipality of Araguaína – TO. Multidisciplinary Core scientific journal of knowledge. 04 year, Ed. 11, Vol. 01, pp. 145-167. November 2019. ISSN: 2448-0959, Access link in: https://www.nucleodoconhecimento.com.br/health/municipal-hospital
SUMMARY
The present work seeks to discuss the reduction of costs in the staff of the Municipal Hospital from the Specialty Outpatient Clinic and the Public Health Emergency Units offered to users of the Unified Health System – SUS of the municipality araguaína-TO and region from the partnership between the municipality and a Social Organization (OS). Among the questions that the present study seeks is the following question: is it possible to offer better quality in such an essential service to the community by spending fewer resources? How to measure the productivity of a service as complex as the health area itself being public or private? Thus, we will make a diagnosis about the current situation, thus seeking to answer whether it is possible to reduce costs without compromising the efficiency of the process. Therefore, the methodology used was exploratory descriptive research in the case study modality. Data were collected through technical visits made in-place, through semi-structured interviews, meetings and observations that were confronted with the survey of the existing technical literature. The results obtained indicate, at first, the dimensioning of the staff of the units followed by the proposal of resizing within the parameters used aiming at cost reeducation without the loss of the quality of services.
Keywords: Cost reduction, personnel resizing, health.
INTRODUCTION
In the midst of an increasingly competitive business scenario, the managers of organizations are faced daily with the need for management tools that assist them in the administration of available resources in achieving operational activities. Despite this context, health institutions are also included, which, generally, because of their essential character, is almost imperceptible by the issue of competitiveness. Since they compete broadly in the same scenario where other organizations seek, with great effort, their perpetuation and/or simply the guarantee of their own existence. On the subject, thoroughly clarifies Matos (2005) when he says: “… companies in this business segment live with the same challenges as a growing demand for professional management, without which the viability of health organizations will not be able to make possible, not to mention the very maintenance of survival” (MATOS, 2005, p. 19 ).
It is in this challenging scenario of public health in Brazil that the present study intends to contribute. To this end, it seeks solutions to one of the most challenging problems of any organization, namely the management of increasingly scarce resources, be it these material, financial or human resources. Originally, the present study was carried out at the request of a Social Organization (O.S.) that concludes a management contract with the municipality of Araguaína in three units Municipal Unified Health System namely: Municipal Hospital of Araguaín[2]a (CNES no. 3663051), Ambulatory of Specialties (CNES no. 6216420) and Emergency Care Unit (CNES no. 6886345). In the search for the optimization of the management of available human resources, the first question arises: it is possible to better serve the population that consumes daily the service offered by the municipality from the Social Organization using an amount of human resources less than currently available in the organizational structure?
One of the most relevant factors in the search for this response is exactly the complexity of the study area. Because it is such an essential area for the individual, no technique of reduction or optimization of resources should be applied without first understanding the context, implications and risk involved in such intervention. Similarly, the theme is also justified by the complexity of the subject, that is, due to its social relevance, because a decision-making of this size directly affects a very expressive sample of the population. In order to answer this type of questioning, this article has as its general objective to identify the possibility of optimizing the use of human resources in health units administered by the Social Organization (O.S.), through a contract of management with the municipality of Araguaína-TO considering the following aspects:
a) Analyze the current dimensioning of the staff of the health units administered by the Social Organization with the municipality; And
(b) submit a proposal for the adequacy of the framework.
It is noteworthy that the main agent acting within this process is a recent model of shared management. In it, the government celebrates a partnership with private institutions, in this case with social organizations, also known as OS’s. In order to rescue a very close past, we must remember that, in Brazil, social organizations emerged on May 15, 1998, regulated by Law 9,637. Barbosa and Elias (2010), report that since the mid-1990s, the expression of this term was taking traction through the State Apparatus Reform Master Plan (PDRAE), proposed by the Ministry of Administration and State Reform (Mare), still in the first FHC government (1995-2002). The central issues of this debate permeated the sphere of the implementation of new forms of management and provision of public services in the area of non-exclusive services of the State. According to the PDRAE:
Social Health Organizations (OSSs) are defined as entities of interest and public utility, non-profit association, arising from the qualification of legal entities governed by private law, in teaching activities, technological research, technological development, protection and preservation of the environment (1990, p. 60).
It is observed that the above concept deals specifically with social organizations in the health area, considering that this was the first model implemented in Brazil, then coming to the other areas, and, finally, as widely disseminated in the media of communication, the OS’s migrated to education. For Ribeiro (2017), this concept is expanded and reaches a more philosophical level defined by him in this way: “The idea of social organization is linked to the social process, the idea of change, of arrangement of the behavior of individuals in the construction of life social.” After the debates and avoiding the controversies, the fact is that social organizations are increasingly present in public administration, and thus occupy the gaps that the state cannot fill.
It is exactly in the midst of this scenario that the object of our study discusses which will be presented from its development presenting, for this, reflections on the dimensioning of the current four of collaborators. This work was divided parts, and in the first, the characteristics of the municipality of Araguaína were raised in relation to the health sector. In the second, there is a description of the methodology used for the development of the proposal to refit the staff. The third part of the study consists of parameters and concepts used in the present study and in the fourth situational diagnosis of the health units object of the research. In the last stage, the proposal for resizing within the parameters used was presented and, at the end, the considerations listed on the possible difficulties that may exist in the implementation phase of the proposed dimensioning were made.
2. CONSIDERATIONS ABOUT THE MUNICIPALITY OF ARAGUAÍNA
The municipality of Araguaína is located in the State of Tocantins, in the Northern Araguaia Middle Health Region, with a population of 170,183 inhabitants (IBGE, 2015) and is a reference for the population of the Centro Norte Macroregion, composed of the Bico do Saúde Regions Parrot, Middle North Araguaia and Cerrado Tocantins Araguaia, covering a population of 652,103 people (IBGE 2015), which corresponds to 43.03% of the total inhabitants of the State. In Araguaína there are 196 health establishments registered in the National Register of Health Establishments – CNES, of the Ministry of Health, thus classified:
Table 1 – Type of health facilities
| Type of establishment | Amount |
| General Hospital | 4 |
| Specialized hospital | 1 |
| Medical offices | 125 |
| Emergency Service | 1 |
| Other | 65 |
| Total | 196 |
Source: Ministry of Health, DATASUS, CNES, 2016
The four general hospitals held in 2015 and 2016, 20,385 and 9,032 hospitalizations, respectively, approved by the SUS Hospital Information System – SIH/SUS:
Table 2 – Number of hospital admissions approved per establishment
| Establishment | Year | |
| 2015 | 2016* | |
| Hospital Regional de Araguaína | 8.924 | 3.554 |
| Hospital Dom Orione de Araguaína | 7.993 | 3.864 |
| HDT – Hospital de Doenças Tropicais de Tocantins | 1.226 | 651 |
| Hospital Municipal de Araguaína | 2.242 | 963 |
| Total | 20.385 | 9.032 |
Source: Ministry of Health – SUS Hospital Information System (SIH/SUS), 2016 * until competence Jun/2016
In addition to the hospital units mentioned above, specialized medical consultations are also performed at the Specialty Outpatient Clinic and the Emergency Care Unit. The number of 181,507 and 62,999 of visits was totaled in 2015 and 2016, respectively.
Table 3 – Number of specialized medical consultations approved per establishment
| Establishment | Year | |
| 2015 | 2016* | |
| Instituto de Doenças Renais do Tocantins | 304 | 100 |
| APAE de Araguaína | 706 | 506 |
| Hemocentro Regional | 335 | 148 |
| Hospital Regional de Araguaína | 46.227 | 11.704 |
| Hospital Dom Orione de Araguaína | 3.083 | 1.730 |
| HDT – Hospital de Doenças Tropicais de Tocantins | 16.051 | 7.695 |
| Hospital Municipal de Araguaína | 1.214 | 370 |
| Ambulatório de Especialidades | 11.857 | 7.445 |
| UPA Anatólio Dias Carneiro | 101.730 | 33.301 |
| Total | 181.507 | 62.999 |
Fonte: Ministério da Saúde – Sistema de Informações Ambulatoriais do SUS (SIA/SUS), 2016* até a competência jun/2016.
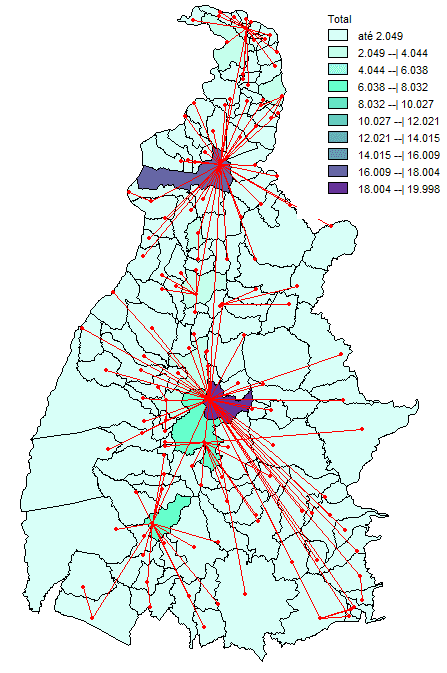
Specialized medical consultations carried out in health units administered by the Social Organization correspond to about 64.25% of the total procedures performed in Araguaína. Intrastate transit of patients can be visualized through the routing map constructed based on the records contained in hospitalization authorizations – AIHs with registration in datasus of the Ministry of Health. When analyzing data from the State of Tocantins it is possible to note that the largest flow of patients is to the cities of Araguaína and Palmas (Figure 1), which demonstrates that the first is a city in the health sector, which also reflects on the composition of human resources available levels in the city.
Table 4 – Number of professionals per profession and place of activity
| Profession | Number of professionals* | ||
| Tocantins | Araguaina | % em Araguaína | |
| Social worker | 438 | 51 | 11,64% |
| Nurse | 2320 | 427 | 18,41% |
| Farmacêutico | 619 | 160 | 25,85% |
| Fisioterapeuta | 579 | 66 | 11,40% |
| Médico | 2081 | 381 | 18,31% |
| Técnico e Auxiliar de enfermagem | 6302 | 1404 | 22,28% |
| Técnico de radiologia | 326 | 54 | 16,56% |
Source: Ministry of Health, National Register of Health Establishments (CNES), 2016 * competence Jun/2016
Figure 1 – Map with patient referral flow within the State of Tocantins in 2015 and 2016*
3. METHODOLOGY
The methodology used in this work consisted of the survey of existing technical literature, legislation and work and studies on quantitative indicators of personnel in hospitals. Studies of personnel dimensioning published by the Getúlio Vargas Foundation, by the São Paulo State Department of Health, academic papers and scientific articles were used, all listed in the bibliography at the end of the work. Data on the current staff dimensioning of health units were requested and on-site visits were made to know the work processes, physical facilities and directors and heads of sectors were interviewed.
The data provided were confronted with those collected on site as well as a study on sizing. For this, the historical series of production of the health unit as well as the average occupancy rate was considered. Some conditions were also considered that directly interfere in the dimensioning of the staff as: social organization personnel policy, profile of the users served, working conditions offered to employees, level of complexities of the services offered, degree of technology incorporated by the hospital, physical plant, facilities and building conservation.
4. PARAMETERS, INDICATORS AND CONCEPTS USED
For the studies to be carried out and a better understanding of the technical terms used in it, a theoretical rescue accepted by the specialized technical literature was carried out. In this theoretical survey, one of the authors conceptualizes:
Indicators are data and/or information obtained in specific realities that characterize these organizations in the necessary professional aspects. They allow to make some comparisons and analyses in other contexts, taking into account differences and similarities. Parameters are numerical relationships found in the quantification of people by sectors, professions in relation to production. They are validated and accepted nationally and are valid for the population under analysis (PICCHIAI (2009, p. 40).
The work presented focused primarily on optimizing the staff, including, intends, based on the readjustment of the number of people per sector, to indicate alternative forms of hiring to reduce costs. To achieve this goal the use of other concepts must be explained for the understanding of the formulas and parameters used. The concepts are the same adopted by Picchiai (2009) who thus presents them:
Intensive care: severe and recoverable patients with imminent life risk, subject to instability of vital functions, requiring permanent and specialized nursing and medical care.
Intermediate care: stable patients from the clinical and nursing point of view, requiring medical and nursing evaluations with partial dependence of nursing professionals to meet basic human needs.
Minimum care/self-care: patients stable from the clinical point of view of nursing, but physically self-sufficient in order to meet basic human needs.
Complexity: Which covers or terminates elements or parts. Hospitals, due to their complexity, are characterized as secondary, terciaries and quaternaries, according to the assistance provided, technology used and services developed.
Small hospital: hospital unit with up to 50 beds;
Medium-sized hospital: hospital unit with 51 to 149 bed;
Large hospital: hospital unit that has more than 150 beds;
Hospital indicators: instruments used in the evaluation of hospital performance, involving its organization, resources and work methodology;
Information: a given with knowledge; management instruments are important, serving as support for planning and decision-making. It is the act or effect of reporting, communicating, questioning. Represents data or knowledge evaluated for specific uses.
Index: everything that indicates or denotes some quality or characteristic; relationship between values of any measure or gradation; dimensional number that can serve for the compilation of dysfunctional phenomena in different times or situations.
Functional bed: bed available to be used in hospitalization.
Busy bed: the bed effectively occupied by a patient.
Care model: methodology established in the systematization of care.
Management model: comprises the administrative activities developed. Model: allows the size of hospital staff adequately for satisfactory patient care; of a normative nature, seeks to meet the medical and hospital needs of patients, and the resulting support and administration services.
Number of hospitalizations (per day per month): the number of patients who were hospitalized in the period considered.
Pattern: object that serves as a model to the making of another; official model of weights and measures; Model. It is the documented commitment used in common and over and over and over again by all the people involved.
Standardization: the systematic activity of an organization, to establish and use patterns.
Size: determined by the installed capacity of beds, according to the definition of the Ministry of Health.
Hospital departure: It is the patient’s departure from the discharge hospital unit (cured, improved or unchanged), evasion, treatment withdrawal, internal transfer, external transfer or death. Internal transfers are not considered outs for calculations of hospital statistics
Services: set of medical specialties, sick, psychological etc. offered to the patient, whose characteristics may be influenced by the maintaining entity, length of stay, among others.
Rate: ratio between the variations of two quantities of which the first is dependent on the second.
Occupancy rate (daily, monthly, per clinic, general): a percentage relationship between the number of beds occupied and the number of beds available.
Average length of stay: the number of days that the patient was hospitalized, calculated by the mean of patients hospitalized in the month in focus.
Variable: which can present several distinct values; collected interest characteristic (PICCHIAI, 2009, pp. 41-42).
It is observed that the use of the description in full by the author is justified according to the complexity of the subject studied that deserves a highlight with regard to the integrity of the technical terms used. Throughout the work, these concepts and parameters appear and, thus, for the preparation of a study that serves to guide the decision-making process of an organization it is necessary to ensure, at the very least, that communication is precisely established.
5. DIAGNOSIS OF THE CURRENT SITUATION
5.1 MUNICIPAL HOSPITAL OF ARAGUAÍNA
The Municipal Hospital of Araguaína – HMA is a medium-sized hospital that performs low and medium complexity procedures. The unit has 56 beds, 46 pediatric clinical beds, 9 surgical beds and 1 isolation bed. The unit serves the local and referenced population, as agreed in the Scheduled and Integrated Agreement – PPI and is a regional reference for the urgent, emergency and elective procedures, of low and medium complexity, in ophthalmology specialties and Pediatrics. HMA has a stabilization room, two operating rooms, two nursing clinics, medical offices where the Specialty Outpatient Clinic, laboratory, kitchen, laundry and administrative facilities operate.
Within the unit are also located the headquarters of the Municipal Regulatory Center and the Treatment Service Outside the Home – TFD. The hospital has old and worn physical facilities. The building has two floors and, at the ground level, are located the medical offices, stabilization room, laboratory, pediatric beds, nursing rank 1, kitchen, laundry and administrative facilities. On the upper floor are located the operating room, the recovery room after anesthesia – RPA, surgical beds, nursing rank 2 and, provisionally, the hospital file. The management contract signed between the Social Organization and the Municipality of Araguaína has quantitative and qualitative goals to be met monthly by the social organization, highlighting:
- 300 hospital departures
- 2083 outpatient consultations
- 60 emergency/ophthalmologic consultations
- 30 pediatric surgeries
- 90 ophthalmology surgeries
- 1,100 clinical analysis procedures
- 162 x-ray
- 31 ultrasounds – USG
- 08 electrocardiograms – ECG
The parameter used to calculate the hospital exit target (hospitalization) is an occupancy rate of 75% and average permanence rate of 4.1 days. In August/2016 the unit had the following number of employees: 01 general director, 01 technical director, 01 nursing manager, 03 visiting physicians (prescribers), 02 physicians working in the emergency/surgical emergency on a warning basis, 08 physicians in the pediatrics sector (doctors are hired on duty, totaling 60 shifts/month, with, carrying, variation in the number of people according to month and scale). 12 nurses, 45 nursing technicians 01 physiotherapist, 01 pharmacist, 01 pharmacy assistant, 01 nutritionist, 02 social assistants, 06 biochemists, 02 faturists, 14 cup assistants, 03 cooks, 10 administrative assistants, 07 agents of ordinance, 06 laundry assistants, 04 drivers and 04 receptionists.
5.2 EMERGENCY CARE UNIT
The Emergency Care Unit Anatolian Dias Carneiro is a pre-hospital component of the UPA Porte 2 modality, according to the classification described in Ordinance GM/MS no. 104/2014. The unit has 11 observation beds and 04 medical offices. THE UPA has all the equipment and services required by Ordinance No. GM/MS 104/2014 and, thus, the unit has conserved physical facilities, requiring only a repainting of the outside. The management contract provides that the social organization should perform 24-hour care and serve, monthly, 8,000 users of the SUS, 2,800 pediatric visits and 5,200 medical clinic, with an observation rate of 15% of the patients treated and 30% of patients referred.
In addition to the visits, the UPA should perform 4,400 clinical analysis procedures, 2,833 x-rays and 100 ECG monthly. In August/2016, the unit had the following number of employees: 240 medical shifts working in urgency/emergency, 01 nursing coordinator, 12 nurses, 28 nursing technicians, 02 social assistants, 01 pharmacist, 02 pharmacy assistants, 06 cup auxiliaries, 08 receptionists, 05 concierge agents, 01 model and 04 drivers.
5.3 SPECIALTY OUTPATIENT CLINIC
The Specialty Outpatient Clinic is integrated with the Municipal Hospital of Araguaína and has 05 medical offices, air-conditioned reception and area of collection of material for examinations. Also in August/2016 the unit had the following number of employees: 05 nursing technicians, 01 nurses, 02 reception attendants (administrative agent) and 04 receptionists.
6. SIZING PROPOSAL
After the survey and the diagnosis of the current situation, the time has come to propose the improvements and readjustments that can lead to better management of human resources employed in the activities mentioned with the guarantee of not losing efficiency in the processes, or why not say, improve the efficiency of these processes by relocating and optimizing available resources. Thus, the analysis of the collected data presented the possibilities per unit, as can be observed below.
6.1 MUNICIPAL HOSPITAL IN ARAGUAÍNA
For the proposal of dimensioning in this unit, it was considered as an average stay of hospitalization 4 days, according to a serious historical year of 2016:
Table 5 – Average historical series of permanence – 2016
| Month | Average stay |
| January | 3,7 |
| February | 3,6 |
| March | 4,2 |
| April | 4 |
| May | 4,2 |
| June | 3,9 |
| July | 4,1 |
| Total | 4 |
Source: Ministry of Health – SUS Hospital Information System (SIH/SUS), 2016
The occupancy rate in 2016 ranged from 33% to 49% of installed capacity, with an average of 39%, well below the 70% recommended in the management contract:
Table 6 – Frequency of invoiced nights and occupancy rate – 2016
| Month | Installed Capacity | Produced | Occupancy rate |
| January | 1.650 | 592 | 35,88% |
| February | 1.650 | 684 | 41,45% |
| March | 1.650 | 593 | 35,94% |
| April | 1.650 | 685 | 41,52% |
| May | 1.650 | 813 | 49,27% |
| June | 1.650 | 619 | 37,52% |
| July | 1.650 | 547 | 33,15% |
| Total | 11.550 | 4.533 | 39,25% |
Source: Ministry of Health – SUS Hospital Information System (SIH/SUS), 2016.
For the nursing sector, the workload of 40 hours/weekly and a technical safety index of 15% and 5.6 hours were considered, because it is a health unit that performs low and medium complexity procedures, pursuant to COFEN Resolution No. 293/2004. Regarding the number of professionals in the nursing sector, the parameter presented by Picchiai (2009) was adopted, namely 20% of the sector composed of nurses and 80% by nursing technicians. Scaling is obtained by applying the following formula:

Table 7 – Parameters for calculating the number of employees for the nursing sector – pediatrics
| Description Value | Value |
| Number of beds | 46 |
| Occupancy rate | 0,3 |
| Hour-care | 5,6 |
| Days of the week | 7 |
| IST | 0,15 |
| Weekly journey | 40h |
Total people for the nursing sector of Post 1 (pediatrics): 18 + 3 of STIs, totaling 21 people, 4 nurses and 17 nursing techniques. These professionals should divide into two shifts of 12h. For surgical beds:
Table 8 – Parameters for calculating the number of employees for the nursing sector – surgery
| Description Value | Value |
| Number of beds | 9 |
| Occupancy rate | 0,39 |
| Hour-care | 5,6 |
| Days of the week | 7 |
| IST | 0,15 |
| Weekly journey | 40h |
Total people for the nursing sector of Post 2 (surgery): 4 + 1 of STIs, totaling 5 people, 1 nurse and 3 nursing techniques. Considering the low number of surgeries performed in the unit, it is possible that the nurse responsible for post 1 assumes responsibility for post 2. Regarding the operating room, the historical series of the unit demonstrates that it is enough to maintain a team formed by 1 nurse and 2 nursing techniques, which will also be responsible for the sterilization sector. In the outpatient clinic, it is due to use 1 nurse for every 10 offices and 1 technician for every 3 offices. For the medical picture of the hospital, the number of diarist physicians, also called hospital is, visitor or prescribed should be considered. This professional is responsible for performing the horizontal coverage of patients, with daily performance.
It is observed that both Picchiai (2009) and Sala (2006) recommend that the ideal is that there are 1 doctor for every 10 beds for pediatric sectors and 1 doctor for every 6 beds. Considering that the average occupancy rate of HMA is 39%, it has that 2 diarist or prescribers doctors are sufficient to meet the demand of the unit. The vertical coverage of the unit is made by on-call physicians, using, as a parameter, 1 doctor for every 50 beds.
Only for obstetrics sectors is that the parameter used is from 1 doctor to 20 beds. To meet hma’s demand, 1 on-call is sufficient for each 12-hour shift, totaling 2 on-call doctors per day. The unit performs emergency, emergency and elective surgeries in pediatrics, in accordance with the management contract signed. When analyzing the historical series of production of the unit, it is observed that the number of surgeries, with the exception of ophthalmologic surgeries, is small and may be covered by a warning physician:
Table 9 – Frequency of surgical procedures – AIH
| Month | Approved | Rejected | Total |
| January | 17 | 16 | 33 |
| February | 21 | 0 | 21 |
| March | 21 | 0 | 21 |
| April | 19 | 1 | 20 |
| May | 18 | 0 | 18 |
| June | 14 | 0 | 14 |
| July | 11 | 0 | 11 |
| Total | 121 | 17 | 138 |
Source: Ministry of Health – SUS Hospital Information System (SIH/SUS), 2016.
Therefore, 1 medical pediatric surgeon is enough to meet the demand of the unit. As for the surgical procedures of ophthalmology, the contractual goal is 90 surgeries month, with the provision of procedures for evisceration of the eye, facoemulsification (cataracts), reconstruction of eyelids, reconstruction of the anterior chamber and pterygium. These procedures are considered outpatient surgeries, that is, there is no need for the patient to remain hospitalized in the unit. To meet the demand of HMA in relation to ophthalmologic surgeries, 1 ophthalmologist doctor is sufficient.
For the other areas of the hospital, considering the size of the unit, simply apply the parameters presented by Picchiai (2009) to obtain the number of people for each area. In the sizing work, the laboratory, imaging, cleaning and cleaning and security services, which are outsourced, were not considered. Thus, it is has to be the dimensioning of the staff for the Municipal Hospital of Araguaína, excluding the administrative part of the Specialty Outpatient Clinic that is integrated into the unit, is as follows:
Table 10 – Number of employees per function – Municipal Hospital of Araguaína
| Function | Amount | Parameter used | |||
| General Manager | 1 | ||||
| Clinical Director | 1 | ||||
| Administrative and Financial Director | 1 | ||||
| Nursing Manager | 1 | ||||
| Nurse | 5 | Described in specific calculation | |||
| Técnico de enfermagem | 20 | Described in specific calculation | |||
| Diarist doctor | 2 | 1 for every 10 beds | |||
| Pediatric son-onologist (shifts) | 60 | 1 for each 12h shift | |||
| Surgeon doctor | 2 | 1 overwarning per turn | |||
| Anesthesiologist doctor (on duty) | 60 | 1 for each 12h shift | |||
| Farmacêutico | 1 | 1 for 50 beds | |||
| Pharmacy assistant | 2 | 1 for every 30 beds | |||
| Psychologist | 1 | 1 for 50 beds | |||
| Physical therapist | 1 | 1 for 40 beds | |||
| Social worker | 1 | 1 for every 60 beds | |||
| SAME Helper | 2 | 1 for every 30 beds | |||
| Billing | 2 | 1 for 40 beds | |||
| Laundry assistant | 5 | 1 for 10 beds – included upa | |||
| Seamstress | 1 | 1 for every 100 beds | |||
| Reception | 3 | 1 for every 50 beds 2 for outpatient clinic | |||
| Driver | 0 | Service must be outsourced | |||
6.2 EMERGENCY CARE UNIT
For the dimensioning of the staff of the UPA, the rules contained in Ordinance GM/MS no. 104/2014 for the body of physicians as well as the specialized literature for other employees should be observed. The ministerial ordinance states that there should be 4 doctors from 7:00 am to 7:00 pm and 2 doctors from 7:00 pm to 7:00 am at UPA Porte II. However, the management contract imposes a goal of 8,000 monthly calls, which generates, on average, 16 calls per hour. Considering that the parameter used for emergency medical consultations is 6 consultations per hour, it is required that, on a 12-hour shift, each doctor could perform a maximum of 72 consultations or visits. The daily goal is approximately 266 visits, which requires the constant presence of 4 physicians per shift.
To meet the need for UPA, at least 240 medical shifts are required from 12:00 p.m. For Sala (2006), the parameter for the dimensioning of nursing staff for the areas of emergency care is 1 professional for every 15 care stb’s in 24/h, with the nursing body composed of 20% of nurses and 80% of nursing technicians, and the STIs of 20% should be increased. Applying the above formula, it has to be used for the nursing sector of the UPA, 21 people are needed, 4 nurses and 17 nursing technicians. For the other areas of the UPA, the dimensioning criterion should be applied for emergency or emergency care sectors. In this study, the cleaning and cleaning, safety, imaging service and laboratory services, which are outsourced, were not considered.
Table 11 – Number of employees per function – Emergency Care Unit
| Function | Amount | Parameter |
| General Manager | 1 | |
| Nurse | 4 | Per turn |
| Nursing technician | 17 | Per turn |
| Nurse reception | 2 | 1 for each turn |
| On-call doctor (shifts) | 240 | 4 for each 12h shift |
| Pharmacist | 1 | 1 for 50 beds |
| Pharmacy assistant | 2 | 1 for every 30 beds |
| Reception | 5 | 3 for day time 2 for night |
| Driver | 4 | 2 for each turn |
| Concierge agent | 4 | 2 for each turn |
| Cup assistant | 4 | 2 for each turn |
| Motorista | 0 | Service must be outsourced |
6.3 SPECIALTY OUTPATIENT CLINIC
The Specialty Outpatient Clinic, despite being inserted in the structure of the Municipal Hospital of Araguaína, has its own dynamics and should be analyzed separately. The contractual goal is 2,250 consultations per month divided into several specialties. The outpatient clinic operates From Monday to Friday, from 7am to 7pm and saturdays from 7am to 12pm. The Specialty Outpatient Clinic has 5 medical offices, with access to the room for collecting material for examinations and access for radiology tests and other hospital facilities. Due to the high number of medical consultations, the hiring of physicians should be made by production, thus not the need to estimate the number of professionals for this sector. Regarding nursing staff, Picchiai (2009) and Sala (2006) recommend that 1 nurse is required for every 10 offices and one nursing technician for every 3 offices. For reception, it is estimated that the time dispensed for each patient is 12 minutes. For the calculation of the number of receptionists and support staff, the following formula applies, according to Picchiai (2009):
Considering that 12 minutes are 0.2 technical hours and, on average, 113 patients are treated daily, in 5.5 days a week and with a journey of 44 hours per week, it is necessary 3 people to work at the reception.
Table 12 – Number of employees per function – Medical Outpatient Clinic
| Function | Amount | Parameter |
| Specialist doctor | – | Hiring by production (consultation) |
| Nurse | 1 | 1 for every 10 offices |
| Nursing technician | 2 | 1 for each office |
| Receptionist and support | 3 | 0.2 technical time for each patient |
6.4 SUMMARY TABLE
To better understand the proposed situation, it follows an explanation of the synthesis framework in order to help understand the proposed dimensioning in the organizational structure, as presented.
Table 13 – Comparative table – Araguaína Municipal Hospital
| Function | Current quantity | Recommended quantity | Minimum Quantity |
| General Manager | 1 | 1 | 1 |
| Clinical Director | 1 | 1 | 1 |
| Administrative and Financial Director | 1 | 1 | 1 |
| Nursing Manager | 1 | 1 | 1 |
| Nurse | 12 | 5 | 5 |
| Nursing technician | 45 | 20 | 18 |
| Diarist doctor | 3 | 2 | 2 |
| Pediatric son-onologist (shifts) | 60 | 60 | 60 |
| Surgeon doctor | 2 | 2 | 1 |
| Anesthesiologist doctor (on duty) | 60 | 60 | 30 |
| Pharmacist | 1 | 1 | 1 |
| Pharmacy assistant | 2 | 2 | 2 |
| Psychologist | 1 | 1 | 1 |
| Physical therapist | 1 | 1 | 1 |
| Social worker | 1 | 1 | 1 |
| SAME Helper | 2 | 2 | 2 |
| Billing | 2 | 2 | 2 |
| Laundry assistant | 5 | 5 | 5 |
| Seamstress | 1 | 1 | 1 |
| Reception | 4 | 3 | 3 |
| Driver | 4 | 0 | 0 |
It is observed, in the table above, that the nursing sector is currently enabling the largest intervention, considering that, for example, the number of nursing technicians is almost three times greater than the minimum allowed, according to the parameters presented. Thus, it is possible to make a significant decrease in this situation without the loss of quality in the provision of service in this area.
Table 14 – Comparative Table – Emergency Care Unit
| Function | Current quantity | Recommended quantity | Minimum Quantity |
| General Manager | 1 | 1 | |
| Nursing Coordinator | 1 | 1 | 1 |
| Nurse | 12 | 4 | 4 |
| Nursing technician | 28 | 17 | 17 |
| Nurse reception | 2 | 2 | 2 |
| On-call doctor (shifts) | 240 | 240 | 180 |
| Pharmacist | 1 | 1 | 1 |
| Pharmacy assistant | 2 | 2 | 2 |
| Reception | 8 | 5 | 4 |
| Driver | 4 | 0 | 0 |
| Concierge agent | 5 | 4 | 4 |
| Cup assistant | 6 | 4 | 4 |
Undoubtedly, one of the most complex sectors to propose a resizing of personnel is the Emergency Care Unit, depending on the specific ordinance that governs the unit and previously determines the minimum number of personnel. Nevertheless, it is noted that the current nurse scan of 12 professionals can perfectly be reduced to one third of this amount. The team of nursing technicians can also lose 11 employees, and still will be able to meet the demand installed in the unit.
Table 15 – Comparative function picture – Medical Outpatient Clinic
| Function | Current quantity | Recommended quantity | Minimum Quantity |
| Specialist Physician | – | – | – |
| Nurse | 1 | 1 | 1 |
| Nursing Technician | 4 | 2 | 2 |
| Receptionist and support | 4 | 3 | 3 |
Finally, the synthesis of the medical outpatient clinic proposes a 50% reduction in its team of nursing technicians, which is the most impactful intervention for the department. Therefore, because it is a synthesis of the data already widely discussed above, it is unnecessary to re-analyze them, considering that the intention is exactly to bring, from a single graph, information inherent to the current situation, to the recommendations and the minimum amount accepted for each sector.
7. CONCLUSION
During the preparation of the study, it can be perceived that there is an idleness of most of the human resources employed in the three service units. One of the main objectives was whether it was possible to accurately measure a service as complex as that of the health area. And in this, the objective was widely achieving, taking into account the existing technical literature that allowed the application of formulas of production calculations for each area and health sector. After the necessary measurements of productivity, as well as possession of the collected data, it was easy to prove that, by using the calculations, observing their application in full, the sectors that demonstrate excess available labor are likely to reduce to the levels close to the limits established without loss of the quality of the service provided.
The estimate of staff dimensioning made in this study considered the production of the units and the information provided by the Social Organization that operates in that municipality. The numbers presented for the nursing area are considered horizontally, and the nursing scale should be made according to the duty regimen adopted in the unit (12 x 36) or fixed contracting system (30 or 40 hours per week). The specificities of collective agreements or agreements of work as well as the plans of positions and remuneration of the Social Organization were not considered for the study. Finally, the quantity presented refers to a total number of employees, and there should be divisions of the number per working period (day and night, weekday and weekend).
REFERENCES
BARBOSA, N. B., ELIAS P. E. M. As organizações sociais de saúde como forma de gestão público/ privado. Cienc Saude Colet, v. 15, n. 5, p. 2483-2495, 2010.
BORBA, V. R. Administração hospitalar: princípios básicos. 3 ed. São Paulo: CEDAS, 1991.
BRASIL. Portaria nº 104 de 15 de janeiro 2014. 2014. Disponível em http://bvsms.saude.gov.br/bvs/saudelegis/gm/2014/prt0104_15_01_2014.html. Acesso em 16. Mar. 2017.
MALAGÓN-LODOÑO, G. Administração Hospitalar. 3. ed. Rio de Janeiro: Guanabara Koogan, 2014.
PICCHIAI, D. Parâmetros e indicadores de dimensionamento de pessoas em hospitais. Pesquisas e Publicação da Escola de Administração de Empresas de São Paulo. São Paulo: FGV, 2009.
RIBEIRO, P. S. O que é Organização Social? Brasil Escola. 2017. Disponível em http://brasilescola.uol.com.br/sociologia/o-que-organizacao-social.htm. Acesso em: 16. Mar. 2017.
SALA, A (org). Parâmetros para o planejamento e dimensionamento da força de trabalho em hospitais gerais. Secretaria de Estado da Saúde de São Paulo. São Paulo, 2006.
2. CNES – Cadastro Nacional de Estabelecimentos de Saúde.
[1] Postgraduate in MBA Business Management, Controllership and Corporate Finance from the Graduate and Undergraduate Institute (IPOG); Postgraduate in Teacher Training in Didactics and Educational Management from the Graduate and Undergraduate Institute (IPOG); Postgraduate in Municipal Public Management from the State University of Goiás (UEG) and Bachelor of Administration from the Graduate and Undergraduate Institute (IPOG).
Submitted: June, 2019.
Approved: November, 2019.















