SOUSA, Eliane Maria de [2]
SOUSA, Eliane Maria de. Public Policies and Social Inclusion of Down Syndrome. Multidisciplinary Scientific Journal. Edition 05. Year 02, Vol. 01. pp 987-1050, July 2017. ISSN:2448-0959
ABSTRACT
Down syndrome is a genetic anomaly, where people who have this syndrome are considered to be people with special needs, this syndrome causes mental retardation, between the mild and moderate ranges. The inclusion of people with special needs has been gradually advancing in recent times, with the purpose of promoting community and diversity and equality for all. This work of Conclusion of course aims to address through Public Policies the Social Inclusion of people with special needs, and regarding their rights within society, highlighting Down Syndrome. The research has qualitative and exploratory characteristics, bibliographically, aiming to have more knowledge despite living with people with special needs, and with an interview with the Director of the institution CECOF II located in São Vicente – SP, a school for people with special needs, and with interviews of the parents of a Down Syndrome student. In the interview it was clear that inclusion, still finds a barrier, and that inclusion will only be possible, when there is no prejudice and when people learn to live with differences.
Keywords: Public Policies, Down Syndrome, Social Inclusion.
INTRODUCTION
The world has evolved in relation to people with disabilities, including Down syndrome in both physical, mental and intellectual aspects.
According to Sassaki (1997, p.15), the expression special needs, accompanying the word person with, or bearer of, does not replace the specification of the quality of being with special needs.
This research will mention the history of the discovery of down syndrome, genetic cause, behaviors, characteristics and care of people with Down syndrome.
According to Melero (1997, p. 205), which underlies the concept of disability in the different phases of history, there is a theory that underpins and influences the way of considering or treating the disabled person.
Therefore this study is about the inclusive policies both in the school and in the social life of people with DS.
Integration and inclusion are based on the principle of standardization, which does not mean making a person with disabilities normal, but creating the conditions for the child to have the same opportunities and rights, making use of them by his own resources. It means, therefore, to recognize and attend to their needs respecting their rights as a person and a citizen. (Werneck, 1997, p.50).
This study deals with the origin of PP in Brazil, the beginning, and what is the role of the State in relation to people with disabilities. Public policies today want the inclusion of children both in schools and in society, and have the opportunity to grow with autonomy and hope in the future.
According to Mazzota (1989, p. 4), “care should not be given due to limitations, but mainly to the capacity for development and change of the human being.”
The methodology will be qualitative, will be based on interviews, where will be approached the behavior of children both in school and in the family.
Inclusion is understood as the adaptation of society to include people with special needs in their general systems that prepares them to assume their roles (Sassaki 2003: 41).
Wernec[3]k (1997, 53) explains that inclusion implies a “total and unconditional insertion” of the disabled person in society, while in integration “the insertion is partial and unconditional to the possibilities of each person.”
This work has two parts, where the first is based on a theoretical and bibliographic study, describing down syndrome, characteristics, diseases, the role of the State and the rights of people with special needs.
The other part of the research shows the importance of inclusion both in the school and in the family and social environment, ending with interviews and final considerations.
The purpose of this work is knowledge, and through interviews there is still prejudice and the lack of professional qualification is the path to inclusion, according to the interview with the parents and the Director of the educational institution.
And that this work can contribute and show through research and studies a little about Down syndrome, and social inclusion, rights and duty of the State, and show that without prejudice and empowerment, the name deficient becomes love, love to the next and love to God.
Character and intelligence can impress people, but it is the love we give to someone who makes us bright and unforgettable in their life … Because love makes people indispensable. So if you want to light a smile, light up a heart or wake up to hope someone needs to remember one thing: people rejoice with their intelligence, appreciate your character, but really need is your love! The Holy Spirit makes us look at others in a new way, seeing them always in Jesus as brothers and sisters that we have to respect and love (Pope Francis).
1. WHAT IS DOWN SYNDROME
The history of Down Syndrome emerged in the seventh century with the records of Anthropologists finding a Saxon skull that presented structural modifications typical of people with Down Syndrome.
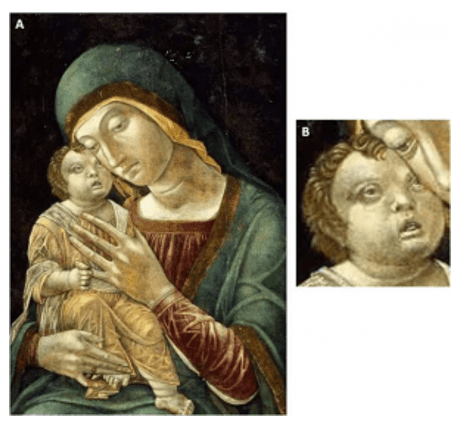
Andrea Mantegna, a 15th-century artist, was a painter and painted several pictures of Madonna with the boy Jesus and the characteristics of the boy, were identical to the child with SD as in the painting Virgin and Child.
In 1618, another painter Jacob Jordaens in his painting “Adoration of the Shepherds” also has a child with characteristics of SD.

According to Schwartzman (1999),
The Olomeca tribe, who lived in the Gulf of Mexico between 1500 BC and 300 CE, according to archaeological findings, have sculptures, drawings among other fossils that show similar physical characteristics to those with Down Syndrome.
In the Olomecas region, sculptures and drawings of adults and children that were found had the characteristics of people with DS. And according to the belief of the Olomecas people with SD was the crossing of an ounce and a woman at a later age.
In the Middle Ages the disabled were discriminated against and even abandoned and were not considered as human beings but monsters and of another species, and were the result of the union between the demon and the woman. In the sixteenth century Luther ordered the mother and the disabled son to be killed.
According to PESSOTI (1994, pp. 6-8) confinement or exclusion became the expression of the charity-punishment ambivalence as a benevolent attitude of guarantee of survival. In this way, society was spared the inadequate conduct of the handicapped.
In 1866 an English physician named John Langdon Haydon Down worked in a clinic with children with neuropsychomotor retardation in Surrey, England, was the first to describe the physical similarities and mental retardation in certain children where the term “mongolism” and ” Mongoloid idiocy “because of the inadequate condition and similarity of the eastern peoples. And according to the doctor explained that SD was a state of regression in evolution.
It was in 1959, Jerome Lejeune discovered that the cause was genetic and named the genetic disorder as Down Syndrome to honor Dr. John.
Dr. John deserved credit for distinguishing children with SD from those with mental disabilities and for recognizing physical characteristics, and their influence came from Charles Darwin’s book, “The Origin of Species.”
“It is a representative of the great Mongolian race. When they stand side by side it is hard to believe that they are not children of the same parents … The eyes are situated obliquely and the inner commissures of the eyes are more than normal. The eyelid cleft is very narrow. The lips are large, thick and with transverse folds … “(Down, apud Pessotti, 1984, p.143)
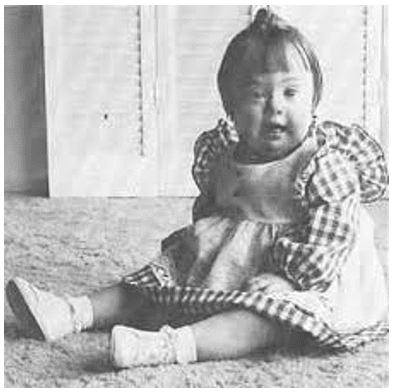
1.1 CHARACTERISTICS OF DOWN SYNDROME
What differs from a normal child to a child with Down syndrome is the physical and medical characteristics of the child because of the diagnosis.
Smaller head and slightly flattened (whitening) and rounded that differs from a normal child. At birth the fontanelle (molleiras) are larger and take longer to close in some cases. And to cases of partial alopecia (hair failure) or total alopecia (total hair loss);
The face has a flat contour, the nasal bone is sunken, small nose and narrow nasal passages;
Eyes: Narrow, oblique eyelids, palpebral fold (skin fold) in the corners of the eyes as babies, and irises with white markings (Brushfield spots);
Small ears, and upper edge of the ear (helix), and narrow ear canals;

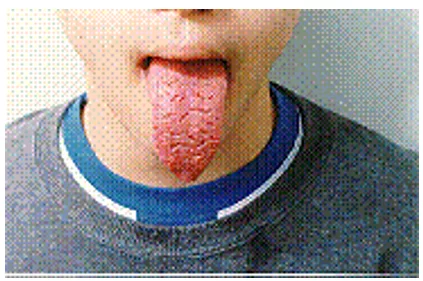
Small mouth, some children are left with their mouth open and their tongue projected, tongue streaked in older people, lips cracked in winter, palate narrower, milk teeth that are slow to project, absence of tooth or tooth with different shape, small jaws causing stacking of permanent teeth and lower index of dental caries;
Wide and thick neck and in babies loose folds of skin on the sides of the neck disappearing with the growth of the child;
Thorax (tapered) sunken pectoral bone or pectoral bone dove (designed) and globose breast when the child has enlarged heart because of congenital heart disease. Children born with heart problems are called high heart murmur, it is due to malfunction of a valve.
Some babies have underdeveloped (hypoplastic) lungs, and children who have congenital heart disease have increased blood pressure in the pulmonary vessels causing pneumonia.
Generally the muscles of the abdomen of the children are weak and may have a protuberance, present a rupture in the region of the navel (umbilical hernia) and in some cases do not need surgery closing as the child grows, but in some cases are surgical.
The genitals of the girls are underdeveloped, such as: the lips and clitoris; ovulate normally but their menstruation is irregular and the male genitals are small and the testicles are not in the scrotal sac and can be found inside the abdomen or groin.
The feet and hands are small and thick and the fifth finger is curved inward, and there is a fold across the palm or both hands. The child’s toes with SD are short and have a large space between the big toe and the second finger and a fold in the sole of the foot between them.
![FIGURE 7 - Characteristics of the hand of a child with SD: fold in the plama and a single fold in the little finger. Source: Page "Syndromes and evils" [4]](https://www.nucleodoconhecimento.com.br/wp-content/uploads/2017/08/f7-caracteristica-da-mao-de-uma-crianca-com-sd-prega-simea-na-plama-e-uma-so-dobra-no-dedo-minimo.png)
Not all children with down syndrome have all the physical characteristics mentioned above, and not all have similar appearances, some are more pronounced than others, and some change over time.
And even with all these physical characteristics mentioned do not interfere in the familiar coexistence or in the social life.
Melero (1999)[4] believes that intelligence does not define, but constructs itself, not being fixed and constant throughout life. It emphasizes that the person with DS is much more than their genetic load, it is an organism that works as a whole, and genetics is only a possibility. This way of functioning as a whole can compensate even its genetic load, through development processes, as long as the contexts in which the person lives (family, social and school) improve.
1.2 CAUSE OF DOWN SYNDROME.
Down Syndrome is an accident that occurs in the first division of the zygote cells.
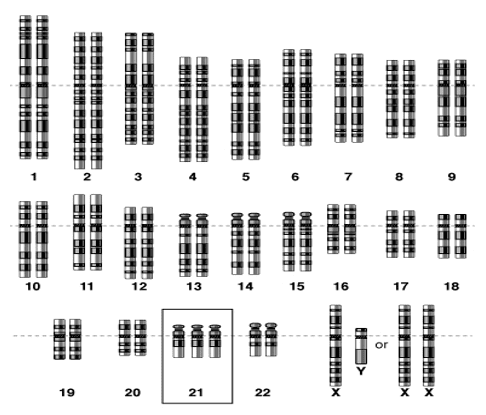
SD is a chromosomal disorder, that is, a syndrome “whose overall clinical condition should be explained by an imbalance in the chromosomal constitution”, in this case, the presence of an extra chromosome in pair 21, characterizing the trisomy 21 (Brunoni, 2003) .
The trisomy means that there is an anomaly in the cell because a person who has normal cells the chromosomes add up to 46 where 23 are from the mother and 23 are from the father occurring from 1 to every 800 births.
There are three trisomies of the 21:
- Simple trisomy is the non-chromosomal disjunction (separation of the chromosomes that does not occur correctly and the two 21 chromosomes remain united and this means non-disjunction) and occurs in 95% of the cases of Down Syndrome. When Down syndrome is caused by simple trisomy, its origin is a chromosomal defect that occurs in the language of the reproductive cells of one of the progenitors (not pre-zygotic disjunction) or in the initial cell of the affected zygote (non-disjunction post zigotica)
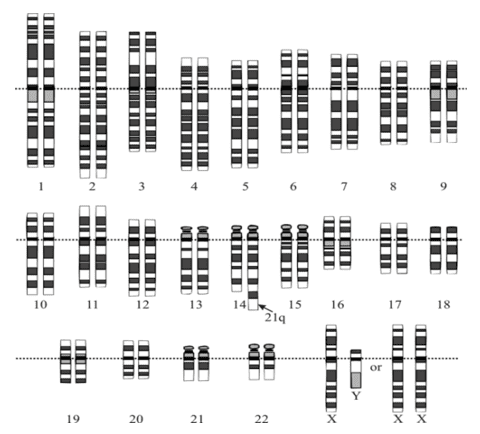
- Translocation trisomy occurs when the pair of chromosomes 21 is stuck on another chromosome, the person has the 46 chromosomes and yet the person is a carrier of Down’s syndrome and occurs in about 3% of the cases. If a child is born with Down Syndrome by translocation parents have a chance of having another child with Down Syndrome.
The extra chromosome 21 is superimposed or translocated to another chromosome, usually about 14,21 or 22. If the translocation is found in a child with Down syndrome, it is important to examine the paternal chromosomes, since in one third of cases a parent may be responsible for the translocation. (PUESCHEL, 2000, p.1-2)
- Mosaic trisomy occurs when the person has the normal cells that are
the 46 chromosomes and the trisomic cells, that is, 47 chromosomes and occurs in 2% of the cases of Down Syndrome.
According to Epstein et al. (1995), it is now possible to correlate Down’s genotype / phenotype, making it possible to prevent or minimize its incidence with this clarification.
1.3 RELATED DISEASES
Many children with DS are born with congenital anomalies and some can be life threatening and life threatening.
Congenital cataracts occur in about 3% of children with DS. And if it is not detected and removed from the eye, the child may become blind.
In the gastrointestinal tract occurs the blockage of the alimentary tube (atresia of the esophagus), a connection of the alimentary tube (esophagus) with the tube of air (trachea); narrowing of the output of the stomach (pyloric stenosis); blockage of the intestine adjacent to the stomach (duodenal atresia); absence of certain nerves in some parts of the intestines (Hirschsprung’s disease); absence of anal opening (anal imperforation), and other anomalies. This occurs in about 12% of children with Down syndrome.
Congenital heart defects occur in about 40% of children with DS. The problem that most occurs is in the central part of the heart between the holes in the walls and between the chambers, and abnormal functioning of the heart valves where it is called the endocardial defect or atrioventricular canal.
Children with DS often have respiratory infections in childhood and especially those with congenital heart disease; ear infections, and some adolescents have skin infections mainly on the thighs and buttocks.
There have been reports of increased gingival disease in children with Down syndrome.
In 8% of people with SD have some type of seizure disorder. Children between 5 and 10 months of age have infantile spasms; and older people may develop seizures that may be associated with Alzheimer’s disease.
It has also been reported in children with various SD sleep apnea records is due to some obstruction in the fundus of the throat by large tonsils and adenoids.
50% of children with DS have visibility difficulties, to see by far and 20% to see up close. Some children have obstructed tear ducts; some are vesgas (strabismus); have inflammation of the eyelids (blepharitis); and sometimes rapid eye movements (nystagmus), some people with DS may develop cataracts during adult life.
60% to 80% of children with DS have mild to moderate auditory deficits, increasing auditory canal wax, frequent ear infections, and sometimes drainage from the middle ear to the throat due to upper respiratory infections, congestion, large adenoids or dysfunction of the Eustachian tube (the connection between the middle ear and throat).
Most people with DS have thyroid problems. The dysfunction occurs when there is an increase in thyroid hormone (hyperthyroidism) or when it is below the thyroid hormone (hypothyroidism).
Skeletal anomalies are common, but the most worrisome are the ligaments that are easily stretched. Most children with DS have hyperextension of the joints (loose or double joint) and may lead to increased subluxations (incomplete or partial displacement) and displacement of the knee and hip.
1.4 CARE FOR PERSONS WITH DISABILITIES.
At the end of the last century the first thyroid hormone medicine given to the child with Down syndrome was reported. In 1940 glutamic acid and its derivatives were used; researchers reported positive results at baseline, and in recent studies did not support the initial findings.
In Europe has been used the treatment of dry leaves (sicca cells),[5] are injections of cells prepared from organs of animal ferns, claim to stimulate growth. In an investigation done in the United States, it was questioned that, the injections do not have the expected effect. And scientific publications have reported that this component when injected into humans can trigger severe allergic reactions (anaphylactic shock) or slow viral illnesses several years later.
If it is a single disease, but a complex set of syndromes of the most varied etiologies and different clinical conditions, the only common denominator of which is insufficient intellectual, the problem of mental deficiency involves a huge range of different aspects, from its (Stanislau Krynski, 1999). In this context, it is important to note that there are two types of biological and social factors: biological, psychological, social, and social problems.
And several medications have been used for the treatment of Down syndrome, such as: minerals, vitamins, enzymes, hormones and substances called U-series, and have been used by Henry Turkel. And in 1964 with the study called Double-blind revealed that they had no effects and no differences in the intellectual function of children with DS. Pituitary extract was also used in the treatment of children with DS, but it was found that it did not benefit the intellectual and social development.
According to Amiralian (1997, p.35), Depending on the disability, there may be peculiarities related to their organic condition and, being congenital, physical or mental, have implications for the development or adjustment of the child.
It does not yet have specific treatment, any child who has mental, intellectual or motor deficiency needs to be stimulated as soon as possible.
Children with DS when stimulated depending on the intellectual level may attend regular schools, colleges and work normally.
According to Canning and [6]Pueschel (2012), the mental development and intellectual abilities of these children span a wide range between severe mental retardation and close to normal intelligence. ”
It also has professionals who can help parents in early stimulation, not only for SD as for other disabilities such as: physiotherapists, speech therapists and psychologists. It is through them that parents can cope and help children with disabilities to live a better life and to live in society.
According to Casarin (1999, p.284):
[…] there are no specific psychological assessment instruments for a person with Down syndrome, so the procedure is the same as for other people. The difference lies in the interpretation of the results that should consider the changes present in the syndrome.
Physical therapy is a fundamental treatment for the stimulation of children with DS because of motor development, it is through physical therapy exercises that it allows inclusion, in their independence and in social life. And the sooner you begin your physiotherapy treatment, the better the outcome will be.
According to Melero (1997, p. 206), the condition for defining and analyzing the person with mental disability, according to psychology, depends on the paradigms in which it is supported.
Pueschel (1995) Schwartzman (1999) and Voivodic (2007) state that significant delay in motor development occurs in all individuals with Down Syndrome. But the environment in which they live can influence this development, bringing great progress.
Speech-language pathology treatment [7]is because children who are born with it have hypotonia (musculature of the face and soft mouth), and can impair breastfeeding and development. This professional takes care of the following problems: Eating difficulties, such as sucking, chewing and swallowing; Articulation of sounds, oral language, reading and writing.
The work of psychology in the child with DS consists of several ways such as: evaluating and psychologically monitoring not only the child but also the parents in order to guide them in different situations.
Through personal experiences of their meanings of deficiencies, the psychologist will be able to review their emotions, affections, learn from their denials, being able “to gain the perception of disability as a shared object and to provide our client with a warm and facilitating conditions for their acceptance of this condition, favoring and enabling their own development “(Amiralian 1997, 34).
And the objective of the work is to: Accompany the students’ learning; to guide teachers in student development; encourage parental involvement in the development process of their children; advising parents or guardians on the development of their children; refer students to complementary care, such as: clinical care, psychotherapy, psychiatry and neurology; participate in meetings in schools of Regular Education, conducting guidelines to the professionals of these schools when necessary; accompany students sent to Regular Teaching; carry out reevaluations of students; participate in meetings with the team of professionals of the school, whenever necessary; participate in Class Councils and Parent Meetings; to hold a Parent Group or responsible, promoting greater involvement of these with the school, social interaction, exchange of experiences and work on self-esteem; insertion of people with Down Syndrome in the labor market; promote training on topics related to inclusion in the schools of Regular Education; to perform groups with adolescents and adults with Down Syndrome on topics specific to their needs of the member using the assumptions of analytical psychology.
From this point of view, the role of the psychologist in the care of the mentally ill is widened. It goes from simply pointing out and quantifying the degree of deviation, to pursuing strategies that promote internal growth, autonomy, and personal independence. Special attention should be given to the development of behaviors and skills that facilitate the adaptation of this individual to social norms, increasing their chances of social and professional interaction (Ferreira, 1993).
The care and assistance depend on several concepts, which implies from an act of caring, to providing basic health care services. It is a type of activity with ethical, psychological, social and demographic dimensions that takes into account clinical, technical and community aspects. The demands of the caregiver can be evaluated and investigated, where the level of quality of life can be investigated. When it comes to caring for people with special needs, it is common to find either a paid caregiver or a lay caregiver, or a therapeutic follow-up.
People with physical disabilities have groups of caregivers such as: primary caregiver who is financially responsible; the f[8]amily caregiver; the paid caregiver, with or without kinship. The paid caregiver depends on the financial situation.
Second researches point out that the caregiver who involves people with diversified tasks, get good results. Excessive care with people with mental disabilities is a sign of overprotection. And overprotecting, hinders development, and its autonomy, because of its own limitations due to its deficiency.
Although it is not easy, some demarcation lines must be taken into account so that the mental deficiency is no longer seen as a specific pathology and is considered as a complex complex whose common sign would be in the intellectual deficit of variable etiology and dependent on biopsychosocial factors (Cavalcante, 1987, p.17).
2. PUBLIC POLICY
In recent years, Brazil has advanced in the social promotion of the rights of people with disabilities through public policies respecting their differences.
Economic and social policy actions must guarantee universality and respect for differences, be they gender, disability, ethnic-racial or any other difference.
According to Jairnilson Paim (2002: 269):
You do not do politics without guys. We do not implement policies without power resources. We can not be enlightened, impunity, our whole life. If we want to formulate and implement effectively new health policies, or we resort to power resources that originate from their recipients, they will not be alternatives, let alone new ones.
In order to ensure the participation of Brazilian society in government decisions about persons with disabilities, two National Conferences on the Rights of Persons with Disabilities were held in 2006 and 2008.
In Brasilia on May 12-15, 2006, the first National Conference on the Rights of Persons with Disabilities was held, where the participation of civil society and the public authorities and the three spheres of government were institutionalized. of social policies, aimed at people with disabilities. The CNDPD was promoted by the Special Secretariat for Human Rights, and the National Council for the Rights of Persons with Disabilities (CONADE).
According to the federal gover[9]nment, CONADE was created so that this population can participate in the process of defining, planning and evaluating policies for people with disabilities through articulation and dialogue with other social control authorities and administration managers (Ministry of Justice, 2009).
The second National Conference on the Rights of Persons with Disabilities [10]took place in December 2008 in Brasilia, with a deliberative character. It is the objective of the CNDPD to evaluate the progress of Public Policies and the integration of people with disabilities and of the proposals that propose the social inclusion of people with disabilities.
- International Treaties and the Merger in Brazil
It took place in 1985, with the recognition and consolidation of human rights and has as context the process of redemocratization of the country, and the construction of a new Federal Constitution of 1988. Where it was known like period of democratic transition and that the New Republic was instated. The debate on human rights became part of the political agenda.
With the end of the Cold War, the issue of human rights in the international community has become a global issue. The country was coming to the end of 20 years of authoritarianism, and they demanded urgent actions in the direction of its affirmation.
The Federal Constitution had a special commitment to support the disabled. A percentage of public jobs were reserved for people with disabilities, and the law should define the criteria for admission. In this way, the integration of the disabled is sought both in the public service and in private companies (Pinto Ferreira, v. II, 1991).
After the Constitution, in 1992, there was ratification of the human rights treaties, the International Covenant on Civil and Political Rights, the International Covenant on Economic, Social and Cultural Rights and the American Convention on Human Rights. Brazil in two Optional Protocols to the American Convention on Human Rights, 1998 recognizing the competence of the Inter-American Court of Human Rights, consolidating Brazil’s position on international forms of protection and rights.
The position that Brazil has assumed in defense and protection of human rights shares the agreements and efforts of the international arena.
2.1 SOURCE OF PUBLIC POLICIES IN BRAZIL
The PP in Brazil originated during the colonial period where people with disabilities were excluded from the society, confined by families, collected from the Holy Houses or prisons. The arrival of the Portuguese Court in Brazil and the beginning of the Imperial period changed that reality.
When entering this universe of information, it is observed that, in antiquity, people with disabilities were not even considered human beings, being rejected by society (Corrêa, 2005).
However, if the child looked “ugly, misshapen and shabby,” indicating some kind of physical limitation, the elders kept the child and, in the name of the state, took her to a place known as Apothetai (meaning “deposits”) . It was an abyss where the child was thrown, “for they had the opinion that it was not good for either the child or the republic to live, since from birth it was not well built to be strong and govern throughout his life “(Plutarch’s Licurgo apud Silva, 1987, p.105).
2.1.1 INSTITUTES IN THE EMPIRE
During the Regential period in 1835, Counselor Cornélio Ferreira França of the Legislative General Assembly proposed that each province have a first-class teacher for the deaf and blind and how Brazil was going through a troubled political period, and was only 13 years old that Brazil was independent, the matter was only resumed in 1850.
Brazil was the first in Latin America to care for people with disabilities, where in 185[11]4 the Imperial Institute of the Blind Children (now Benjamin Constant – IBC), E 1856, The Imperial Institute of the Mentally Deaf Deaf-INES).
Although Brazil was the first in the service, restricted numbers of vacancies were offered during the Regulative Period. The only deficiencies that were recognized in Brazil in the nineteenth century were blindness and deafness. And the institutions were based on European experience, and were within the structure of public administration. And institutions were classified as educational institutions.
- The Institute of Blind Boys
In 1854, the IMC was created by Emperor Dom Pedro II to teach blind children, the institution was located in Rio de Janeiro and had as its model the Institute of Blind Boys of Paris, where its teaching methods were the most advanced. And the speech of the young blind man and ex-student of the Institute of Paris Jose Alvares de Azevedo, convinced the emperor to institute it.
The IMC in the first year only served two provinces, Rio de Janeiro and Ceará. And until the end of the regency period, he received boys and girls from several provinces such as Alagoas, Bahia, Espírito Santo, Minas Gerais, Pará, Piauí, Rio Grande do Sul, Santa Catarina and São Paulo. And students were only accepted upon authorization from the Minister and Secretary of State for Business of the Empire.
- Institute of the Deaf-Mutes
In 1856, the Institute of the Deaf-Mutes was created by the Frenchman Hernest H[12]uet, deaf teacher and former director of the Deaf-Mute Institute of Bourges. The first activities were funded by donations and ended in 1857, and with Law No. 939 of September 26, 1857, the budget law allocated public resources and transformed the private subsidized institution, and Huet directed the institution five years, and in In 1861, the institute distorted its objectives.
In 1856 the institute only attended three people. And with the passage of time the service expanded, and the students were: Alagoas, Bahia, Ceará, Rio Grande do Sul, Rio Grande do Norte, São Paulo, Maranhão, Minas Gerais, Paraná, Pernambuco and Santa Catarina.
In 1868, the head of the Section of the Secretariat of State, Tobias Rabelo Leite, made an inspection of the institute’s activities and conditions. And in his report, he verified the deviation of his intentions, transforming himself into asylum of deaf people. Tobias Leite became director of the institution until 1896, and was promoted as a reference in the education of the deaf in Brazil.
And the teaching consisted of some secondary school subjects. And vocational education consisted of agricultural techniques, and most of the students were from poor families and the rural milieu. In 1870, professional dressing and shoemaking workshops were installed.
2.1.2 CIVIL SOCIETY INITIATIVES
In 1889, with the proclamation of the Republic, the institutes changed their denominations. With the fall of the monarchical regime, the name of the “Imperial Institutes of the Blind Boys” was renamed “Institute of the Blind Boys”. And in 1890, for National Institute of the Blind, and in 1891, for the Benjamin Constant Institute (IBC), in honor of its director. The Imperial Institute of the Deaf-Mutes also ceased to be an imperial institution, and became known as the Institute of the Deaf-Mutes until 1957, after which it became known as the National Institute for the Education of the Deaf (INES).
In the Republic the action of the State in relation to people with disabilities has not changed much. In 1926, the São Rafael Institute was founded in Belo Horizonte; in 1929, the institute of Blind Father Chico, in São Paulo; in 1959, the London Institute of Deaf Education (ILES) in Londrina, and all still work.
In 1920, industrialization and urbanization began, and was deepened between 1940 and 1950, where a civil society emerged, and new organizations focused on people with disabilities. And new organizations focused on other types of disabilities and different forms of work, for non-restriction in education and health work.
Without information and without financial resources, involved in a context where survival is the main struggle, disabled people are forgotten in a corner by the family, the community and the authorities. They are marginalized from social life, without citizenship, without dignity. (RESENDE, 1996, p.16)
2.1.3 REHABILITATION CENTERS
The first rehabilitation center in Brazil was the Brazilian Benefit Rehabilitation Association (ABBR), which was founded in 1954 by architect Fernando Lemos, whose son had polio sequelae, ABBR had financial support from entrepreneurs, Percy Charles Murray was the president of the association, and was a victim of poliomyelitis.
ABBR[13] created a rehabilitation school to train professionals such as: physical therapists and occupational therapists, due to the lack of these professionals. In April of 1956, undergraduate courses in Physical Therapy and Occupational Therapy began, with the curricular molds of the School of Rehabilitation of Columbia University. And in September 1957, the rehabilitation center was inaugurated by the President of the Republic, Juscelino Kubitscheck.
Several philanthropic organizations emerged because of the outbreak of poliomyelitis epidemics such as: the Sao Paulo Association of Assistance to Defective Children (AACD), and today called the Association of Assistance to the Disabled Child, and was founded in 1950; In 1956, the Bahian Institute of Rehabilitation (IBR); 1958, The Fluminense Association of Rehabilitation (AFR). Hospitals have also become centers of reference in the rehabilitation of people with polio sequelae, such as: Hospital da Baleia and Hospital Arapiara, located in Belo Horizonte – MG. AACD only began to serve people with special needs in 1963, even though it was founded before ABBR.
In Brazil in 1960, the profile of the people who used the rehabilitation centers, due to urbanization, industrialization and society, and the national vaccination campaigns, had two effects: reduction of cases of sequelae by poliomyelitis, and increased disability due to violent causes, automobile accidents (car and motorcycle), diving and firearms. With the beginning of physical rehabilitation, the medical model of disability appeared, according to which the problem was attributed only to the person with disability. The difficulties in disability could be overcome with the intervention of specialists such as: physicians, physiotherapists, occupational therapists, psychologists, social workers and others.
The model represented the advancement in care for people with disabilities and was based on the pathological clinic of the disability. Disability is seen as the cause of inequality and disadvantage experienced by people.
From the Empire until 1970, they are part of the history of people with disabilities, who did not yet have the autonomy to decide their own life. And for people with disabilities, it was a period of need for organizing movements willing to fight for their rights and autonomy, standing out as paramount, caring and deciding their own lives.
Decree No. 82, dated July 18, 1841, was founded on December 9, 1852, the first hospital, for the treatment of the alienated, the Dom Pedro II Hospice, which was linked to the Santa Casa de Misericórdia of Rio de Janeiro . In 1854, the Imperial Institute of the Blind Boys was founded, and in 1856 the Imperial Institute of the Mute Deaf.
In 1904, the first space was installed, for children with disabilities, the Bourneville Pavilion-School.
From 1940 to 1950, new organizations for people with disabilities emerged at the initiative of civil society. The new organizations were aimed at other types of disability in the form of work.
The initiative to meet the people with intellectual disabilities were the Pestalozzian and Apaeano[14]s movements[15]. And until the middle of the nineteenth century, the intellectually disabled were considered crazy and treated in hospices.
According to Figueira (2008, p. 115):
If until now the disabled person walked in silence, excluded or segregated in entities, from 1981. International Year of the Deprived Person – becoming aware of himself, began to organize himself politically. And, as a consequence, to be noticed in society, reaching significant achievements in little more than 25 years of militancy.
At the beginning of the 20th century, research on intellectual disability began, and the first studies were conducted in Brazil during the Republic. The first scientific work on intellectual disability in Brazil was a monograph written by the physician Carlos Eiras in 1900 about education and pedagogical medical treatment of “idiots”.
In short, Brazil will no longer back down in promoting and defending the human rights of people with disabilities. And it will always have a strong and committed social movement to impel the State to deepen these achievements. May this fight go forward! (Paulo Van)
2.2 RIGHTS OF DEFICIENCIES AND DUTY OF THE STATE.
Deficiency is any loss or abnormality of a psychological, physiological or anatomical structure or function that generates incapacity for the performance of activity, within the standard considered normal for the human being (art. 3, I, of Dec. No. 3,298, December 1999).
The law should not be a source of privilege or persecution, but an instrument regulating social life that needs to treat all citizens equally. This is the political-ideological content absorbed by the principle of isonomy and juridicizado by the constitutional texts in general, or anyway assimilated by the normative systems in force. In short: doubt does not suffer that, in complying with a law, everyone covered by it will receive parified treatment, and it is certain, even, that it is forbidden to deference to different disciplines for equivalent situations.
(Flag of Melo, 1981, pp. 236-237).
The World Health Organization, in 1976, classified as deficient the person with IQ below 70. It establishes for the classification of the person with mental deficiency the following levels: Slight subnormality – IQ 50-69; Moderate subnormality – IQ 20-49; Subnormal severity – IQ 0-19 (Fonseca1987, page 45).
I – One of the rights is the Continuous Benefit Benefit, which guarantees a minimum wage per month for the disabled person of any age, incapacity for independent living and for work, and for the elderly from 65 years. And to obtain this benefit they can not obtain means for their survival. The benefit is regulated by Organic Law of Social Assistance No. 8,742, dated December 7, 1993 (LOAS), and regulated by Federal Decree No. 6,564, of September 12, 2008, regulated by Joint Ordinance MDS / INSS nº 1, of 29 of May 2009.
II – Disability retirement is a benefit granted to workers in the event of: illness or accident, when they are considered by the Social Security expert, incapacitated to perform their activities, or any other type of service that guarantees their livelihood. According to Federal Law No. 3,048, of May 6, 1999.
And in order to be entitled to this benefit, you must have contributed to Social Security for at least 12 months, in case of illness, in the event of an accident, no grace period is required, but you must be enrolled in Social Security.
When you already have the disease or injury, when you begin to contribute to the INSS, you can not retire due to disability, except for the worsening of the disease or injury.
III – The free pass is a right of persons with special needs, if it is considered to be needy, with income equal to or less than a minimum wage, and gives the right to gratuity also for the companion, according to Federal Law No. 8,899, of 29 of June 1994.
IV – Reserves of public seats in public transport companies should reserve preferential seats and be duly signaled for the use of persons with special needs or reduced mobility, elderly people aged 65 or over, pregnant women and people with infants , in accordance with Federal Laws 10,048 of November 8, 2000 and 10,098 of December 19, 2000, regulated by Decree No. 5,296 of December 2, 2004, and State Law 887 of September 10, 1985 and Municipal Laws 317 of April 12, 1982 and No. 3,107 of September 18, 2000.
V – Qualification for persons with special needs, persons with special needs may obtain or renew their National Driver’s License, in accordance with Resolution 80 of November 19, 1998, of the National Transit Council (CONTRAM), but must be approved in physical and mental fitness exams, and psychological assessment exams. In Annex I, item 10.3, it prohibits the driver of adapted vehicles, engage in remunerated activities, and was revoked in accordance with Deliberation 61 of December 14, 2007, of CONTRAM. And with Resolution 267, of February 15, 2008, of the CONTRAM, the adaptations were regulated, where they should be made in vehicles for the use of persons with special needs qualified in the professional categories C, D, and E.
VI – Right to Health, according to Law 7,853, dated October 24, 1989, and regulated by Decree 3,298, of December 20, 1999, guarantees to persons with special needs an adequate and priority treatment, without prejudice to other persons, and with the following measures: creation of health care services, rehabilitation of people with special needs, at all levels of complexity, along with social, educational and work services.
Access to public and private health care, and appropriate treatment for people with special needs, is about appropriate technical standards and standards of conduct. Also having home health care, when the deficiency is serious and not hospitalized.
The technical aids that are: hearing aids, visual and physical; orthoses; equipment, machinery and work equipment adapted; elements that facilitate communication, information and signage; pedagogical material suitable for special education, training and recreation; adaptation of the environment which guarantees free access; collecting bags for ostomates, and high-cost medications.
According to State Law 3,411, dated May 29, 2000, all health establishments must provide full-time conditions and permanence, of persons accompanying in cases of hospitalization of persons with special needs, and in case of absolute medical necessity, prohibit the stay of the companion, the responsible doctor must report in the patient’s medical record.
All persons with special needs are entitled to a medical report on their disability. It is a document that proves its deficiency, and has legal value.
The medical report should describe the type of disability and the International Code of Disease (ICD) corresponding to disease and sequelae. The medical report shall be issued by the public health network and agreed with The Unified Health System (SUS).
2.2.1 CHARACTERISTICS OF DEFICIENCIES, ACCORDING TO (ART. 4 th DEC. No. 3,298, DE DECEMBER 1999).
I – PHYSICAL DEFICIENCY
Full or partial alteration of one or more segments of the human body, causing the impairment of physical function, presenting as paraplegia, paraparesis, monoplegia, monoparesis, tetraplegia, tetraparesis, triplegia, triparasia, hemiplegia, hemiparesis, amputation or absence of limb, cerebral palsy, limbs with congenital or acquired deformity, except aesthetic deformities and those that do not produce difficulties for the performance of functions.
II – HEARING DISABILITY
Partial or total loss of auditory auditory possibilities, varying in degrees and levels as follows: from 25 to 40 decibels (db) – mild deafness; from 41 to 55 db – moderate deafness; from 56 to 70 db – pronounced deafness; from 71 to 90 db – severe deafness; above 91 db – deep deafness; and anacusis.
III – VISUAL DEFICIENCY
The visual deficiency that characterizes of equal or less than 20/200 in the best eye, after the best correction, or visual field inferior to 20º (table of Snellen), or simultaneous occurrence of both situations. And in cases where the sum of the visual measurement in both eyes of the visual field is equal to or less than 60º.
IV – INTELLECTUAL DISABILITY
Significantly lower intellectual functioning, with manifestation before the age of eighteen and limitations associated with two or more areas of adaptive skills, such as: communication, personal care, social skills, community use, health and safety, academic skills, leisure and work .
The diagnosis of intellectual disability can only be realized if the person has a significant lower than average intellectual functioning and presents limitations associated with two or more areas related to adaptive behavior, which refers to communication, personal care, social skills, community use, academic abilities, independence in locomotion, self-care, leisure and work (Luckasson et al., 2002, apud Shmidt, 2009, 27).
V – MULTIPLE DEFICIENCY
Multiple disability – association of two or more deficiencies
For Henri Wallon “The individual is social not as a result of external circumstances, but by virtue of an internal necessity”.
Social inclusion has been studied and debated over time, with the involvement of several professionals, researchers and workers. What we hear most, especially in the media about social inclusion.
According to Hannah Arent “The essence of human rights is the right to have rights.”
With the Universal Declaration of Human Rights, a new cycle has emerged in the lives of all humanity and in almost every country in the global world. The UDHR, of 1948, had two characteristics that reaffirmed the earlier rights that it was: Universality, which was intended for all men; and positivity, which defended the protection of the right that was intended even against the State.
According to Mader (1997, p.47) “Inclusion determines how legitimate all members of society are.”
In Scotland in June 1994, a group of young adults with DS signed the first statement of rights of people with SD.
We have the right: to life; namely that we have Down Syndrome and what it means to us; of not being treated as a child; of being treated as adults, with respect and equality; to vote and to participate in society; to date, to have sex, to marry or to live with someone, if we wish; to have children; to control our money; employment and education; to be independent and, at the same time, to request support, whenever we want; to talk about us; to do what we think is right and not what others think is right; to take advantage of our professional chances; of saying no. (Werneck 1997, 227).
The rights of persons with disabilities were also ensured by the 1988 Federal Constitution.
According to Silva (2005, p.2[…]00); life, besides being a fundamental right of the individual, is also an interest that, not only to the State, but to humanity itself, due to its conservation, must be preserved.
It is the duty of the State and the family, the moral and legal obligation to do something, and assert the rights of children and adolescents.
“Duty is a very personal thing; stems from the need to take action, not from the need to insist on others to do anything. ” (Mother Tereza of Calcutta)
According to Sontag, Smith and Sailor (1977):
The educational emphasis for these groups of children began seriously around 1970. Today, each type of disability is defined by special conditions inherent to each individual that interact with the specific requirements of the environment. From this, in the education of children with disabilities, the ecological functional model, which perceives the child in complex interactions with the environmental forces, emerges.
- EDUCATION AND INCLUSION
With regard to inclusive education, which historically special education has been tied to erroneous views. This view was often related to demonic or supernatural possession, since until the eighteenth century the notions of disability were basically linked to mysticism and occultism, there being no scientific basis for realistic notions (Drago 2005, p.271) .
The Salamanca Declaration (apud MEC, 1994) has as its principle:
- Every child has a fundamental right to education, and must be given the opportunity to attain and maintain the appropriate level of learning;
- Every child has unique characteristics, interests, abilities, and learning needs;
- Educational systems should be designated and educational programs should be implemented to take into account the wide diversity of such characteristics and needs;
- Those with special educational needs should have access to the regular school, which should accommodate them within a child-centered Pedagogy, able to meet such needs;
- Regular schools with such inclusive orientation are the most effective means of combating discriminatory attitudes by creating welcoming communities, building an inclusive society and achieving education for all; in addition, such schools provide effective education for the majority of children and enhance the efficiency and ultimately the cost effectiveness of the entire education system.
The principle of equality is one of the most difficult legal remedies. This is due to the interweaving existing in its bunch of right ingredients and legal target elements. Substantial equality posits the uniform treatment of all men. It is not, as we see, an equal treatment of the law, but of a real and effective equality before the goods of life (Celso Roberto Bastos, v. II, 1989).
Inclusion is a matter of citizenship. Including also means having access to information and dealing with rights and duties (Werneck, 1997, pp. 40 and 171).
Social inclusion in Brazil began in 1996 with the approval of the Law on Guidelines and Bases of National Education 9,394 / 96 in Art. 58, where it says: that special education, for the purposes of this Law, the modality of school education, is offered preferentially in the regular network of education, for people with special needs.
In order for human diversity to be present as a universal value, the school must take on the role of constructor of equality, in order to include in the social fabric those that have been systematically excluded. (Jesus, 2004: 38).
The school inclusion of people with DS plays a fundamental role in the development, and enables among other things such as: social interaction, psychomotor development, language development, learning in writing, participation in play activities, establishing limits, and learning daily life, as basic acts of survival and social integration, for example, body care.
Thus the school must act, working with the possibilities through the inclusion of reducing the boundaries between the school space and the world, in an attempt to weaken the preconceived ideas about the differences, since, the school has never been a space of equals. And with that, to contribute to discriminatory representations being deconstructed making room for respect for differences (Rodrigues, 2007).
As the author relates, the school has participation and action, in boosting both people with special needs and also those who do not have them.
The basic function of the school is to equip individuals to be, on the one hand, competent users of the reading and writing system, that is, fully literate people and, on the other hand, capable of interacting with the knowledge accumulated by the various scientific disciplines and the way of constructing knowledge that is proper to science (Oliveira, 1996, p.
The LD[16]BEN, predict the beginning of schooling, for ages 0 to 6 years, performed in day care centers for people with mental disabilities, starting after birth.
“To take advantage of the phase of acceleration of the myelination that occurs in the first moments of human development, when the neural networks grow and structure”, according to the stimulation received (Fonseca 1987, p.53 and 18).
For people with SD, education does not begin in day care, because of the care they require, in view of their commitments. Soon after having been diagnosed with SD, they receive a special care as soon as possible.
According to Franco (1995, p. 3), to provide children with bio-psycho-social and educational experiences that allow them to reduce their deficits and assist them in developing their abilities in the first years of life.
A program with a multidisciplinary team consisting of physiotherapist, social worker, psychologist, occupational therapist and speech therapist, with integrated planning in the areas of child development, is a suitable program for babies with DS.
According to Franco (1995, p.9): “This service was implemented in the APAE of São Paulo from 1975, by a Dutch pedagogue”.
School inclusion has the function of preparing, equipping the child for life and providing the development of physical abilities and social skills; and to help children with SD achieve a sense of self-respect, satisfaction, and self-esteem.
According to Oliveira (1996, p.99):
[…] the basic function of the school is to equip individuals to be, on the one hand, competent users of the reading and writing system, that is, fully literate people and, on the other hand, capable of interacting with the knowledge accumulated by the various scientific disciplines and the way of building knowledge that is proper to science.
Children with DS have the ability to learn if they attend regular classes according to their needs.
According to Martin and Marchesi (1995: 30).
Students with learning disabilities or language problems, as well as those with learning delays due to behavioral disturbances or social maladjustment, are advised by the teacher: “in[…]teractive social learning situations, through which the student internalizes the mechanisms of control and planning of their own behavior. ”
For Mazzotta (1982, p.16): […]education consists in a rational work to favor, by the diversity of opportunities, each individual so that he becomes a person, in the highest meaning that can be attributed to the term.
The chronological age of the child with DS is different from the functional age, so we should not expect an identical response to the response of children without the syndrome.
The fact that the child has not developed a skill or demonstrates immature behavior at a given age, compared to others with identical genetic condition, does not mean an impediment to acquiring it later, as it may slowly mature. (SCHWARTZMAN, 1999: 246).
These difficulties occur mainly because the nervous immaturity and non-myelination of the fibers can hinder mental functions such as: Ability to use abstract concepts, memory, general perception, abilities that include imagination, spatial relationships, body schema, ability to reason, transference in learning. The deficiencies and weaknesses of these functions mainly hamper school activities.
Among other deficiencies that have repercussions on the neurological development of the child with Down syndrome, we can determine difficulties in making decisions and initiating an action; in the elaboration of abstract thought; in the calculation; in the selection and elimination of certain informative sources; in the blocking of perceptual functions (attention and perception); in motor functions and changes in emotion and affect. (Schwartzman, 1999: 247)
Therefore, the child born with DS has the ability to develop and do daily activities, acquire professional training, evolve language and activities as reading.
According to Troncoso (1998, p.69): “Young people with SD today, compared to those of previous generations, have reading skills that allow them to access written information in general, thereby improving their personal interaction possibilities and their social skills” .
If we truly want a fair and equal society in which all people have equal value and equal right, we need to re-evaluate the way we operate in our schools to provide disabled students with the opportunities and skills to participate in the emerging new society Stainback 1999, 29).
3.1 SCHOOL BEHAVIORS
Children with DS have no behavior problems, their behavior is related to the level of their development. SD children grow up experiencing difficulties, and are expected to fulfill their daily lives, being difficult to perform because of problems with speech and language, short-term auditory memory, delayed motor coordination and learning. At first, the behavioral problems of children with the syndrome are low compared to other students. So they tend to be anxious and frustrated more easily.
The development of the individual carrying the SD is as much as that of any non-bearer, resulting from social, cultural and genetic influences; including expectations regarding their potentialities and abilities and the affective-emotional aspects of learning (Bissoto, 2005, p.87).
One of the behavioral problems is the use of manipulation strategy, and research shows that many children with SD tend to adopt these strategies, hampering the learning process, and some of them use social behaviors to distract the attention of adults to avoid learning. Therefore it is good to be attentive to the manipulation strategy, separating immature behavior from inappropriate behavior.
The difficulties of adaptation found by the intellectual handicapped are presented according to social and cultural life situations, where each one is required to meet the criteria expected by the age group (Coelho, 2001 apud Sousa, 2009).
The behavior of children has as characteristics: to do tantrum in the face of frustration demonstrates feelings like shame, fear or nightmares, needing understanding and support from parents and teachers.
Their inappropriate behavior is motivated by: attention, confusion or uncertainty, anger and frustration, need for control, immaturity.
In this way, it refers to the mechanistic view of Descartes, in which man is compared to a clock. And a normal individual is a well-made watch and an abnormal one would be the defective watch. Thus, within this mechanistic view of man, people with special educational needs are seen as abnormal because they do not conform to the norms of normality imposed by society (Micheletto, Serious, 1993).
Here are some strategies for children with DS: clear rules; the student has to understand what is expected of him; the team has to know that the child has to be disciplined just like his colleagues; clear and short instructions and body language for reinforcement; distinguish what can, what does not; always encourage positive behaviors, with an image that stimulates good behavior; good connections with parents and discuss behavioral strategies with them.
I- Support
All students with SD will need at some point, in support, not specifically of an extra or specific team.
It should be pointed out that the family and the school are institutions that also exert great influence on the development of the individual and form their social representations. These institutions have a point in common, to prepare individuals to act in society, since they are born in a world already structured by social representations and through which they will develop and become part of a systematic set of social relations and practices (Duveen, 1999).
School staff members should be aware of the student’s needs and work well with them, giving support when needed, but can not be helped at all times. The important thing is that they are inserted and motivated in the group to overcome their limits. Support can be given by your own colleagues.
The point is to provide these students with the services they need, but in an integrated environment, and to provide teachers with an update of their skills. The school features in times of great social transformation are changing, and teachers need to acquire new skills to work with academically and socially different students (Scholoss, 1992, p.242 apud Stainback, Stainback 1999, p.25).
The strategy of working in small or double groups brings better results for the learning of all. And students who are withdrawn from the learning group, and are supported by professionals, may have difficulty working together, becoming independent and separating from socializing.
Students with intellectual disabilities like any student need to develop their creativity, the ability to know the world and themselves, not only superficially or through what the other thinks. Our greatest mistake is the mental endowment of people with disabilities on an always very low level. From this mistake, all educational actions derive from the fact that each person is a person, who has different backgrounds, experiences of life and is always capable of learning and expressing his or her thinking. (Batista, 2005: 27)
II – How to support
Support is the responsibility of the entire team, and all members must be integrated to: plan, communicate, feed and monitor.
The sensitivity of the professional to perceive how the person with down syndrome places himself before these instruments, interpreting the results from a dynamic observation (Casarin, 1999, 285)
III – Specific learning
People with SD are delayed in their development, and have program needs facilitated. And your characteristic learning profile are strong and weak.
This definition marks a new age in terms of definitions for mental deficiency by emphasizing the educational focus, demonstrating a concern with development, learning and social adjustment (Fonseca 1987, 44).
And each child has their own characteristics, and the learning style according to their special educational needs.
Given this assumption, if an individual has a special educational need, it does not mean that he will be deprived of interacting with the social environment, but rather will have a particular way of appropriating knowledge and it is the sociocultural environment to provide mechanisms for this learning and development (Vigotsky, 1997).
The characteristics are typical of many people with down syndrome, some with physical and other cognitive implications, and many have both.
- Visual impairment
About 70% of children with DS are born with visual impairment, and need to wear glasses before seven years, and go unnoticed as a result of their disability.
Some signs can be identified at school as indicators of low-vision behaviors, such as: watery eyes; pupil tremor; the hesitant gait; constant stumbling; difficulty in finding the direction of objects, not being able to deviate; approximation of objects to the face; annoyance and intolerance to clarity and sensitivity. You may observe repetitive movements of moving or turning, swinging your body back and forth at a time, rubbing your eyes and moving your hands and fingers before your eyes. These are the clues that teachers can observe and replace activities, of use of senses, such as touch.
It is, therefore, the verification of visual acuity a process in which it is sought to establish functional capacity of the eye, representing it by a numerical expression that, in essence, is the result of an angular measurement. Such measurement is obtained by subjecting the printed eye of increasing magnitudes, from those that are present from one minute to those of tenfold angular values, to the discrepancy of the eye. These symbols, figures or letters, are called optotypes, both smaller and more acute the angles and, therefore, the greater the visual acuity, which allows us visual acuity to grow in an inverse ratio of the angle that measures it (Paiva Gonçalves, 1979. P.31).
And for children with DS, it is good to suggest in a general way: to alert parents to periodic visual exams and glasses when necessary; students always in the first row in the classroom; figures and texts with larger print; text written with pen in black ink and yellow and not white paper.
When the child has low visual index: use pencils 6b or 3b or even a watercolor pen; contoured and highlighted drawings; touching and looking at objects; use capital letters.
- Hearing deficiency
Children with DS often have some hearing loss at birth, and many of them develop recurrent otitis because of fluid build-up caused by respiratory tract infections. The Ministry of Health guidelines for people with DS indicate that annual auditory acuity assessment is required.
As for degree of vision impairment, it can be applied to hearing. Alongside people with no hearing, there will be those with mild hearing impairment. There will always be, therefore, the need to analyze the concrete case to verify if the individual with little hearing finds difficulty in adapting to the social reality he lived (Baker, 1950, vol. I p.29).
And the strategy for discovering auditory deficit is to: place the child close to the adult in group work; talk to the child; emphasize the beginning and end of sentences; reinforce speech with facial expressions, signs or gestures; reinforce speech with visual support; reformulate and repeat the answers and phrases that may not have been well heard.
Although the concept of incapacity for the purpose of granting social security benefits differs from the concept of incapacity for the purpose of protecting the disabled person, the concept of ‘hearing impairment’ is independent of that of incapacity (Revista …, 2001, pp. 60-70)
- Delay in gross and fine motor skills.
With low muscle tone (minimal contraction of a muscle), the children present motor retardation in their development, they present loose ligaments, meaning high flexibility and variation of movements. And with the flexible thumb joint, along with the low tonus in the fingers and wrist, and with smaller fingers and less friction, can disrupt writing.
Strategies to help: Rest your feet on a solid surface when the child is seated; use a sloping board or book, to maintain a straight posture; extra practice; varied activities and multisensory materials; manual exercises; exercises to strengthen the wrists and fingers; coordination exercises between eyes and hands; cutting exercises; like wielding a pencil; lines marked by mark-text for writing.
- Difficulties in speech and language.
Children with SD have some degree of speech and language deficiency and many of them only begin speaking at the age of three. And all can communicate early, even without the use of language, but through gestures, use of signs and body language.
A learning disability refers to a retardation, disorder, or slow development in one or more processes of speech, language, reading, writing, arithmetic or other school areas resulting from a disability caused by a possible cerebral dysfunction and / or change emotional or behavioral. It is not the result of mental retardation, sensory drainage or cultural and instructional factors. (Kirk, 1962 p.263, Apud in Garcia, 1998).
Language delay is caused by combinations of physical factors, and perceptual or cognitive difficulties. Delay in learning and understanding, and using language, lead to cognitive delays. Receptive skills are greater than expressive, that is, they understand more than they speak.
Some traits that are common in language acquisition: difficulty in understanding instructions; minor vocabulary; difficulty in learning grammatical rules; difficulties in learning in social language.
Garcia (1998) states that for many, many years, it was assumed that all students with learning disabilities had experienced some sort of brain damage. But according to the author himself the difficulty does not stem from the brain damage.
Some strategies to help learning: give time to process language; listen carefully; face to face and eye contact; simple and familiar language, short and concise sentences; ask the child to repeat the instructions; avoid ambiguous vocabulary; reinforce speech with visual expressions, gestures and signals; avoid closed questions; encourage the child to speak loudly; use concrete materials.
3.2 INCLUSION AND ADAPTATION
Sassaki (1997, p.170) highlights some guiding principles of inclusion:
Celebration of differences; right to belong; valuing human diversity Equal importance of minorities; citizenship with quality of life.
Every child has the right to education, so it is necessary, to do everything possible so that everyone can progress and learn. It is necessary to look for means and educational methods that allow students to learn.
Learning arouses several internal processes of development, which are able to operate only when the child interacts with people in their environment or in cooperation with their peers (Vygotsky, 1988, p. 101).
Education imposes on itself the duty to make each of us a person with an identity well defined by the canons of normality, the canons that mark what must be habitual, repeated, right in each of us (Perez de Lara Ferre, 2001: 196).
The child with SD has the capacity to learn, but has difficulty learning and adapting. As a result, relevant educational adaptation (objectives, methods, assessments, etc.) is intended to achieve progressive progress.
The Disabled Persons Integration Act (LISMI) in 1982 underwent a change where it was defined that disabled people should integrate into the general system of general education, receiving the support programs and all the resources they need. And on the other hand, for those who find it impossible to school in special education centers.
The General Education System (LOSE) Law in 1990 establishes that the whole educational system must have the necessary resources so that the child with special educational needs can achieve the goals set for all students.
Teachers must be prepared, the educational centers must be organized and with the physical and material resources to favor the students’ learning. It is necessary for teachers to make the necessary curricular adjustments so that the students achieve the appropriate education.
In order for these advances to be effective, it is necessary to ensure the training of all school professionals, curriculum adaptation and parental support (Voivodic, 2004)
I – Curriculum
It is a project that determines the objectives of school education, selects everything that is possible to teach, what it will teach in the school environment, specifies how and when to teach, and how to evaluate. The curriculum is flexible, so that all centers adapt on a particular basis.
[…] in order to allow and promote the productive participation of students with special needs in the teaching and learning process in the regular school, together with their peer partners (peers of the same age group). They are called Small Porte (Not Significant) because its implementation is within the scope of responsibility and action of the teacher, not requiring authorization, nor depending on action of any other higher instance, in the political, administrative, and / or technical areas (Mec, Live Playbook, fasc.6).
There are two types of curricular adaptations that should be based on principles:
– Standardization Principle: which favors and benefits students, whenever possible, from the largest number of ordinary educational services.
– Principle of individualization: Provide the student based on their interest, motivations and depending on their ability and disability, learning rhythms, the educational response to form each person according to their time.
Building a curriculum that addresses people with SD means, above all, understanding the Rousseauian orientation that says: “the child has a way of seeing, thinking and feeling that is his own, […]s[e que, portanto, o seu conselho para os professores era]tart studying your students, because you certainly do not know them at all “(Rosseau, apud Piaget, 1998: 143).
II – Curricular adaptations
Curricular Adaptations of Curriculum Access:
They are the modifications of space, material, personal or communication resources that can facilitate the students with special educational needs and develop the ordinary curriculum, or in the particular case, the adapted curriculum. Students with motor and sensory disabilities, curricular adaptations can be of two types:
– Physical Access: elimination of architectural barriers, adequate lighting and sound, adapted furniture and support of specialized teachers.
– Access to Communication: technical and technological support, complementary communication, specific teaching materials and alternative systems such as Braille, magnifiers, telescopes, computers, recorders and sign language.
III – Individual Curricular Adaptation:
They are adjustments and modifications of the educational proposal, in order to meet their special educational needs, the student with educational difficulties and can not share with other students.
The curriculum is built on the pedagogical project of the school and enables its operationalization, guiding the educational activities, the ways of executing them and defining their purposes. Thus, it can be seen as a guide, suggesting “what, when and how to teach”; “What, how and when to evaluate” (Carvalho, 1999).
It can be of two types:
– Not Significant: These are adaptations of activities, methodology, techniques, and evaluation tools. At any given time any student may have special needs.
The school is treating the handicapped as an eternal child: its programming is always a program of Early Childhood Education-clippings, collages, connecting figures, painting boundaries, training the motor coordination as a prerequisite for writing and reading, discriminating what is the same , what is different, repeat, follow the model, again and cut, paste, sing songs (the diminutive is purposeful), clean the tables, wash the face, brush the teeth, comb the hair, button, tie, paste, trim , to mount … “(Padilha, 2005, pp. 122 and 123).
– Significant or Very Significant: These are previous modifications after psychopedagogical evaluation, which affect the prescriptive elements of the official curriculum and these adaptations may consist of: Adequacy of objectives, contents and evaluation criteria; Prioritize certain objectives, content and evaluation criteria; Change the timing of evaluation objectives and criteria; Eliminate objectives, contents and evaluation criteria of the corresponding level or cycle; Introduce the content, objectives and criteria for assessing levels.
Inclusion of all without distinction of linguistic, sensory, cognitive, physical, emotional, ethnic, socioeconomic or other emotional conditions and requires planned and organized educational systems that take into account the diversity of the students and offer adequate responses to their characteristics and needs (Brazil 1999: 17).
According to Torres Gonzales (2002), flexibility and openness of the curriculum should characterize the planning and development processes, aiming to rationalize the resources, in order to allow the curricular adaptation to the individual needs of the students. As the author says the curriculum should be appropriate for each student according to their needs and abilities.
And continuing with the author’s conception: “the response to diversity materializes in our educational system through the concept of adaptability of the curriculum” (p.132).[17]
The main challenge of Education today is to guarantee to students, regardless of their socio-cultural diversity, access to academic content important for the exercise of citizenship, thus expanding their possibilities of participation in society (Ribeiro[18], 2006)
4. THE INCLUSION OF PERSONS WITH DISABILITIES IN THE LABOR MARKET.
All people with special needs should be treated equally, anywhere and especially at work.
According to Bobbio (1992: 17): “The rights of man are those that fit man as a man.” In this way all men must have the same rights, regardless of their differences.
In Brazil, the constitution aims to seek the welfare of all specials without any discrimination and the Brazilian Penal Code is punishable by criminal acts and disrespect.
In this sense, inclusion is a bilateral process, in which excluded people and society seek, in partnership, to solve problems, make decisions for their solution and make equal opportunities for all possible (SASSAKI, 1997).
People with disabilities when hired should be treated the same as anyone, and what is expected of the worker: professionalism, dedication and assiduity; that is, independent of handicapped or not.
There are many companies that need the most rudimentary jobs, which do not require dexterity, need motor coordination, or sharp reasoning skills (Ribas, 1985, p.88).
Access to the job market for people with special needs is very important, and the concern of family and friends is due to the way they are treated and the low expectation in their relationship with society.
One should always seek to listen to those who will have their lives affected by professional actions and the proposal of inclusion. Although professionals can offer poor people an awareness of their psychosocial condition and instrumentation to seek better living conditions for themselves, professionals can not alone determine what these conditions are, or even the best ways to achieve them. because they will not effectively break down barriers and live those lives. (GLAT, 1995, p.43).
The limitations or deficiencies found in the health examination may not be impeded from joining or continuing to provide services, provided that the ability of the exceptional person to perform the tasks for which the examination is performed.
People need to speak for themselves, because they know what they need their expectations and difficulties as any citizen. But it is not enough to listen to them, it is necessary to propose and develop actions that will modify and guide the ways of thinking about inclusion itself. (AZEVEDO, 2008, p.50).
To think of a society in which the disabled live better is to think not only of the unique situation in which they find themselves, but also of the mechanisms that absorb and circumscribe all people (Ribas 1985: 98).
And people with SD when they are not working, tend to have depression and low self-esteem. And when they are working, it helps them gain responsibility and develop group relationships, helping to develop cognitive, mechanical and adaptive skills.
According to Law nº 8.213 / 91, art. 93, companies with 100 or more employees have the obligation to fill a portion of their positions for people with special needs. And the name of the reserve of positions is known as the Quota Law.
According to affirms (Joaquim Barbosa Gomes, 2001, pp. 35-38).
[…] Afimative actions, in the first instance, encouraged and encouraged public authorities, without compelling them, to make decisions in favor of groups that were blatantly excluded, considering the race, color, sex and national origin of the people, factors that, until then, considered are irrelevant. The organized pressure of these groups highlighted injustices and encouraged the stimulation of compensatory public policies for access to education and the labor market. In the 1960s and 1970s, in view of the lack of compliance with the norms of mere instigation, and taking into account the increased pressure of the discriminated groups, rigid, compulsory quotas were adopted, which came to be composed in schools, in the labor market and in other sectors of social life a more representative picture of the diversity of peoples.
4.1 RESERVATION OF CHARGES AND LAWS OF QUOTAS.
The quota system has little efficiency when the company does not want or can not admit people with disabilities. The most varied subterfuges, including legal, are used to avoid hiring. Some companies hire lawyers to come up with sophisticated arguments that justify not hiring. Others, more pragmatic, simply raise the qualification requirements to fill the vacancy. As a result, they severely restrict the number of disabled people who can apply for that job (Pastore, 2000, p. 184).
According to Law nº 8.213 / 91, art. 93 the Quota Law, there is a certain percentage, where companies are required to fill positions with people with special needs, and has as the proportion, according to the Law establishes, as:
I – from 100 to 200 employees ……………………………….. 2%
II – from 201 to 500 …………………………………….. ………….. 3%
III – from 501 to 1,000 …………………………………….. ………. 4%
IV – from 1,001 onwards …………………………………….. … 5%
The guarantee of access to work for people with disabilities is foreseen in both international and Brazilian legislation. This conquest stimulated the organization of groups in the sense of seeking varied forms of representation to act in search of new rights (PASTORE 2000).
However, while it is possible to enforce laws that oblige companies to accept people with disabilities, there is no law guaranteeing the best way of living together (GLAT, 1995).
Conditions for proving that the person has a disability: Medical report of the work of the company, where it certifies the legal framework of employment to integrate the quota, and in accordance with the definitions established in ILO Convention 159, Part I, art .; of Decree No. 2398/99, arts. 3rd and 4th with the changes given by art. 70 of Decree nº 5.296 / 04. The award must specify the type of disability and the employee’s authorization to use the same for the company. And Certificate of Professional Rehabilitation issued by the INSS.
Brazil ratified almost all these international treaties and conventions, and in 1988 the Brazilian Federal Constitution incorporated guarantees for persons with disabilities, having as one of its fundamental principles the principle of equality or equality, which prohibits arbitrary differences and absurd discrimination, so that people should be treated unequally as they become unequal (COSTALLAT, 2003).
4.2 THE POSITIVE SIDE OF INCLUSION IN THE LABOR MARKET
The importance of the hiring of disabled professionals, as well as the generation of employment, and the inclusion of people with disabilities in the labor market, contributing to bring dignity to these people, and by including them, we not only offer a salary, but the opportunity of social and psychological rehabilitation.
As we can see, the great transformations that humanity has undergone, especially since the 90s, recognized as the process of globalization in the world, has brought new challenges to reflect, among these challenges is the relationship of the social subject with the work (SILVA, 2000).
The professional exercise brings with it the interaction with other people, the possibility of making friends, the feeling of being a productive citizen, finding a love, and belonging to a social group. And your behavior towards your family changes for the better. The presence of people with special needs in the labor market contributes to further humanising companies and enriching the environment and diversified experiences.
According to Eugênia Augusta Gonzaga Fávero (2004. P. 37-38):
In integration, society admits the existence of social inequalities and, in order to reduce them, allows the incorporation of people who can “adapt” themselves, on their own merits. Still, integration presupposes the existence of distinct groups that may come together. Whereas, to include, means, above all, to “stop excluding”. It assumes that all are part of the same community and not distinct groups. Thus, to “exclude”, inclusion requires that the Public Power and society in general offer the necessary conditions for all. Therefore, unlike integration, one does not expect the insertion of only those who can “adapt”, but guarantees the adoption of actions to avoid exclusion. And, given the inequality already present, it requires that positive measures be used, quotas associated with public policies, for example, to reduce them.
The inclusion of people with disabilities in the job market, is a new group of consumers, with income generation, consuming willingly, because it has many needs, realizing desires, such as the purchase of tablets and smartphones. And with the income, the people with special needs, circulate more and have the greater conviviality with people without special needs.
The lack of structure, social and governmental movement that allow the qualification and professional qualification of people with disabilities; b) the paternalistic or merely assistential view that has been created around these people; c) the stigma of the disability as a sign of incapacity or inability to work; d) the refusal of society and companies to adapt their physical conditions in such a way as to enable them to move; e) absence of these associations or class entities with force for the defense of their rights; f) the high degree of dispersion that people in this category have; g) diversification of the nature of the deficiencies (visual, motor, sensory, psychological, auditory, etc.) and complexity of studies and adaptations for all of them in the work environment; h) massive employment of these people in the informal economy or in underemployment, etc. (Ronaldo Lima, 2003, pp. 151-2).
And the inclusion of professionals with special needs at work creates opportunities for companies to generate more business. A person with a disability is more likely to deal with more difficult situations and solve problems, and in addition to having a different vision, contributes to the process of creation or decision making.
4.3 SOCIAL INCLUSION IN THE PUBLIC SECTOR
According to the legislation, the disabled person is entitled to apply for a public tender, under equal conditions with the other candidates, to fill a position and job whose duties are compatible with the disability of which he is a carrier, being reserved at least the percentage of five percent in face of the classification obtained, competing in all vacancies (art. 37, and its first paragraph, of Dec. n. 3,298 / 99).
[…] at any time, any citizen (including the bidder) may exercise the right of petition to the Public Authorities, ‘in defense of rights or against illegalities or abuse of power’ (Art. 5, XXXIV, ‘a’, of the Federal Constitution), and the Administration, faced with some invalidity of the edict, will have no alternative but to cancel the contest (Celso Antônio Bandeira de Mello, 2001, p.525).
According to Law No. 8.112 / 90, regarding reservation of vacancies in civil public services of the union, municipalities and federal public foundations, where article 5 and paragraph 2 establishes that persons with special needs are guaranteed the right to if you write in a public tender to fill positions, whose attributions are compatible with your special needs; where up to 20% of the vacancies offered in the competition will be reserved.
[…] everything will be solved in the competition itself. If it is a type of position that requires proof of physical ability, this candidate, if he is old enough, will probably not fill it; but if his performance in the physical capacity test is satisfactory, why can not he fill the position? (Minister Néri da Silveira)
According to art. 39, I, II, III and IV of Decree no. 3,298 / 99, the notices shall inform the number of existing vacancies and the total corresponding to those for persons with special needs, the duties and tasks essential to the position, the anticipation of adaptation of the tests, of the training course and of the probationary stage, according to the special need, and in the act of enrollment the presentation of medical report attesting the species and the degree or level of disability.
According to Larissa Fontes de Carvalho (2007):
The 1988 Constitution inaugurated an order in which, despite the recognition of injustice and existing inequality, the goal is to adopt policies aimed at achieving the goals adopted, touching on the State an active, positive and not prohibition of discriminatory attitudes. For these reasons, we understand that the affirmative actions developed with the aim of achieving the goals set by the Federative Republic of Brazil are not only authorized by the constitutional order, but fostered, desired by the constituent.
According to Law 8112/1990, the probationary stage is intended for all who work in the public sector, who has passed all the procedures of the public contest and in the exercise of their functions, people with special needs are assessed as to their abilities, suitability and performance of the position, observed by the attendance, discipline, capacity of initiative, productivity and responsibility.
It is the period of exercise of the server during which it is observed and determined by the Administration the convenience or not of its permanence in the public service, by verifying the requirements established in law for the acquisition of stability moral suitability, aptitude, discipline, attendance, dedication service, efficiency, etc. (Meirelles 2003, p.421).
And at the time of registration the candidate can choose whether or not to use the reserved place. And if you choose to use the vacancy you must state your condition about your disability. Publication of the result should not make any distinction between those who opt for the reserved seat, and the list of approved ones will be by general classification order.
According to Luiz Alberto David Araújo:
If, among the first candidates (in the general list), persons with disabilities are appointed, they will occupy their places on the general list, even though they have been registered for the reserved seat. That is, they made the contest, were approved and did not need the constitutional benefit. Reserved places are not used, although they have been registered for them. After completing the general classification, filling in the regular vacancies, filling in the reserved vacancies begins. If there are ten reserved, for example, there are verified, within the reserved vacancy [19]registrations, how many candidates have obtained a mark higher than the minimum required for the competition, that is, the candidates qualified for public service (approved but not yet classified) . These candidates will occupy the reserved places. They will be the highest averages, provided they are above the minimum, and provided they are already on the general list. Thus, we will be giving special attention to people with disabilities who need the benefits and not any disabled person.
Completing with Meireles (2001a, pp. 403-404), on public offices for people with special needs:
Technical means made available to the Public Administration to obtain morality, efficiency and improvement of the public service and, at the same time, provide equal opportunity to all interested parties that meet the requirements of the l[20]aw, set according to the nature and complexity of the position or employment, as determined by Art. 37, II of CF / 88.
According to Sassaki (2006), social inclusion is the process by which society adapts itself to include individuals and groups in their social systems.
According to Stehr (2000), the origin and legitimacy of social hierarchies are always related to the productive process and its organization.
5. METHODOLOGY
This research has the objective of investigating the development and potential of the person with down syndrome, having as trajectory, social and school.
According to Gil (1993, p.19):
Research can be defined as a rational and systematic procedure that aims to provide answers to the problems that are proposed. Research is required when insufficient information is available to answer the problem, or when the available information is in such a state of disorder that it can not be adequately related to the problem.
5.1 OBJECTIVES OF THE RESEARCH
Provide information about the person with DS, in order to better understand and avoid undue ideas, and to make room in school and social life. Show on the restrictions that the person with DS still has, and on the politics of their identity, the behavioral model, the interaction with the family, and the behavior in the school institution. The importance of quality school in the training of people with special needs, and building a more humane society, which respects the differences of people with differences.
And seek to explain a problem from theoretical references and / or literature review of works and documents that relate to the researched topic. It should be emphasized that in any research, it is necessary to review the literature, an instrument of bibliographic research, which allows to know, understand and analyze existing cultural and scientific knowledge about the subject, subject or problem investigated (Mattos; Rosseto Jr; Blecher, 2004, p.18).
5.2 TYPE OF RESEARCH
This work consists of a qualitative, exploratory or descriptive approach and semi-structured interviews.
According to Alves-Mazzotti (1991: 54), qualitative research “has the disadvantage of suggesting a false opposition between qualitative and quantitative, which must be discarded at the outset: the issue is one of emphasis rather than of exclusivity.”
In the search for the understanding and meaning of a fact, and to understand the interrelations, it arises from the context in which the phenomenon occurs.
According to Ludke and André (1986, p.57 and 69), they point to the possibility of raising some clues or initial intuitions that are starting points for the study.
The data must be numerous and descriptive, and oriented “for apprehension and description of the cultural meanings of the subjects” (André, 1998, p.45). It means that they will not be interpreted only in relation to the messages of the text and also their interrelationships.
The characteristic flexibility will allow for revisions, evaluations and reformulations that may lead to the search for meaning and understanding of reality (André, 1998, p.45).
5.3 PERSONS INVOLVED IN THE RESEARCH
This work is based on research, and on the development and potential of the person with DS, taking as a social and scholastic trajectory. The research took place in the Special School with the name of CECOF II, located in the Municipality of São Vicente, in the State of São Paulo, with the director of the educational institution, and a student with the code name chosen clara, and with the parents of to compare the relationship, school and family.
The director will be represented by the letter (D), the father with the letter (P) and the mother by the letter (M).
The first approach was carried out with the Director of the institution of CECOFF II, on 09/16/2015.
In the first questioning was addressed the time that works with people with special needs,
– D: […]4 years.
In second questioning. What do you think of the social inclusion of special students in regular school?
– D: […]I think it is of great importance, therefore, I believe very much in their potential, but unfortunately it has created a very great barrier, and the lack of professionals is very difficult.
In this sense, according to Sassaki (2003: 42): Social inclusion is therefore a process that contributes to the construction of a new type of society through small and large transformations in the physical environmen[…]ts and in the mentality of all people.
In the third questioning. In your opinion, what barriers still exist for inclusion?
– D:[…] there are several more barriers to main in my concept is prejudice, this is the main taboo, because everyone should work this part.
And second (Carvalho, 2003, p. 25): “But worse than these physical barriers, is the attitudinal barrier, whether by the declared and evident rejection of deficiency and deficient, or by its manifestation of tolerance.”
In the fourth questioning. How do you coexist with special people, especially those with Down Syndrome?
– D: […]I’m suspicious to speak, because I love this world, I love what I do, I try to give the best for the welfare of my students and especially to be able to give them everything wonderful, because their happiness is priceless, because every day of coexistence is an extra learning, and that enriches me as a person and as a human being. “I love the special world”.
Fifth and last. What do you think about the State’s contribution to people with special needs?
– D:[…] precarious, should invest much more in training the professionals and provide learners with conditions wort[21]hy of learning and have, a broad vision to see, that they are able to fly much higher.
The second approach was carried out with the parents of a student studying at the institution of CECOF II, on 09/17/2015.
In the first approach, in order to know and understand if there is relationship, gestation and delivery, the following was addressed:
“How did you get pregnant?[…]” M: The pregnancy was quiet, and nothing abnormal occurred.
– Was the delivery normal, cesarean or had any occurrence? M: the […]birth was normal and nothing happened, of my three children, it was the best gestation and birth occurred.
“After delivery, how was the news that your daughter was special?” M[…]: At first I want to point out that I was scared, because I did not even know what the name down syndrome was, but what it hurt was what the pediatrician spoke in front of everyone who was around, mainly medical interns, – she’ll be a vegetable, will not eat alone and much more, that shocked me.
“And the acceptance?” […]M: at first it was difficult, the more we lived together the more love arose, and today I love it with passion.
According to João B. Cintra Ribas (1985: 52), In general, a couple never have the idea that one day they could have a child born with any type of disability. A family has no idea that a member may one day suffer an accident that makes them disabled.
– How old was the treatment started and how was it for school inclusion? P:[…] She began treatment with speech therapist, psychologist and physiotherapist at six months, due to lack of knowledge in the subject, if she had knowledge and the pediatricians who attended her, had guided her, she would start earlier. And social inclusion in regular schools was a disappointment, she could not adapt, not only the students had prejudices, but also the teachers.
In this perspective, Carvalho (2004) emphasizes three types of professionals in the teacher / student relationship. Those who fear for not feeling prepared, those who tolerate, fulfilling the orders of the inclusive law, but in fact the SD child suffers from abandonment, segregation and exclusion in the classroom, and finally those who reject, claiming they do not give of normal students, placing blame on demotivation and low wages.
– What do parents expect for their daughter in the fu[…]ture? M and P: hopefully, she will forget what happened in the past when she was in regular school, that she lead a normal life, because down syndrome is not a disease and that everyone is aware that not just down syndrome or anyone who have any kind of disability be treated with dignity and respect.
And to complement second (Michels, [22]2006, p. 06) which states:
One can see that the social reality in which one lives today has not incorporated the values of inclusion. All the actions that take place at a certain historical moment are reflected in the inclusive school is nothing more than the reflection of an inclusive society. But, equally, it can be said that an inclusive education has an impact on society, making it more egalitarian, intolerant of prejudice and inclusion.
CONCLUSION
The subject researched was done in addition to learning a little about SD, understanding all aspects that refers to social inclusion and the role of the State.
I realized that with research and interviews, Brazil has taken a big step in the process of inclusion, but there is still much to be done for people with special needs. And the main barrier that still hinders inclusion is prejudice. Inclusion grows every year, and to ensure quality education and for all to accompany growth within a consensus that we must cope with any kind of difference, the State must do its part to: empower all professionals who deal with people with special needs.
In the interview with the director of the educational institution, she reports that there are still barriers and one of them is prejudice. And that the State still has a lot to do in relation to the well-being of all people with special needs, and the main measure is to empower professionals, not only students but also professionals dealing with people with special needs, as reported by mother of Clara.
But what made me excited is to know that beyond prejudice and unpreparedness, there are still people who do not need empowerment, and that love is the best basis for making life better for themselves and for others.
And that the state is striving to improve and provide all people with special needs a decent life, providing employment, inclusive school and their rights guaranteed by C / F 88.
REFERENCES
CECCIM, Ricardo B. Exclusion and otherness: from a press release to a note on mental deficiency. In: SKLIAR, C. (Org.) Education and Exclusions – Social and Anthropological Approaches in Special Education. Porto Alegre: Mediation, 1997.
MULLER, Yára. Counseling with people with disabilities. São Leopoldo: Sinodal, 1999. P. 16.
Brazil, Ministry of Education, Special Education Secretariat. Projeto Escola Viva – Guaranteeing the access and permanence of all the students in the school – Students with special educational needs, Brasilia, C327 2000.
GOMES, Joaquim B. Barbosa. Affirmative action & constitutional principle of equality: law as an instrument of social transformation. The US experience. Rio de Janeiro: Renovar, 2001. P. 35-38.
Move Down. A specific learning profile. Available at <http://www.movimentodown.org.br/2013/05/um-perfil-de-learning-specific/> Accessed on 02 September 2015.
CANEJO, Patrícia Díaz; APODACA, Rosa Ruiz de. Curricular Adaptations (I). Including. Available at <http://www.inclusive.org.br/?p=43> Access on August 28, 2015.
Move Down, What It Is. Available at <http://www.movimentodown.org.br/sindrome-de-down/o-que-e/> Accessed on August 30, 2015.
ABC of Health. Available at <http://www.abcdasaude.com.br/pediatria/sindrome-de-down> Accessed on August 29, 2015.
Citing. Available at <http://www.citador.pt/> access in September 2015.
BANBINO, Leila. Inclusion of Children with Down Syndrome. Available: <http://www.psicopedagogavaleria.com.br/site/index.php?option=com_content&view=article&id=32:inclusao-de-criancas-carriers-of-sindrome-de-down&catid=1:artigos> Access on 28 August 2015.
Ministry of Health. Health care for people with Down syndrome. Brasília, 2012. Available at: <http://bvsms.saude.gov.br/bvs/publicacoes/cuidados_saude_pessoas_sindrome_down.pdf> Accessed on August 20, 2015.
Move Down. Education and Down Syndrome. Available at: <http://www.movimentodown.org.br/educacao/educacao-e-sindrome-de-down/> August 27, 2015.
Move Down. Citizenship and political participation. Available at: <http://www.movimentodown.org.br/direitos/cidadania-e-participacao-politica/> Accessed on August 27, 2015.
BASTOS, Ana Patrícia Beltrão. Inclusion Process of Down Syndrome Patients. Planet and education. Available at: http://www.planetaeeducacao.com.br/portal/artigo.asp?artigo=860. Accessed on August 25, 2015.
Down’s syndrome. Quotes. Available at: <http://sindromededown1a2012.blogspot.com.br/2012/05/cicios-como-uma-atencao-para-essas.html> Accessed on September 15, 2015.
PACIEVITCH, Thais. Social inclusion. Available at: <http://www.infoescola.com/sociologia/inclusao-social/> Accessed on September 10, 2015.
SILVA, Luzia Gomes Da. People with disabilities, equality and social inclusion. Available at: <http://www.ambito-juridico.com.br/site/index.php?n_link=revista_artigos_leitura&artigo_id=10839>. Accessed on 11 September 2015.
MIRANDA, Carlos Roberto. Job Opportunities for People with Disabilities. Health and Work. Available at: <www.saudeetrabalho.com.br/download/oportunidades-miranda.doc>. Accessed on 15 September 2015.
Secretariat of Labor Inspection. The inclusion of people with disabilities in the labor market. – Brasília, 2007. Available at: <www.apaeminas.org.br/arquivo.phtml?a=10414>. Accessed on September 10, 2015.
LIMA, Isabel Maria Sampaio Oliveira; PINTO, Isabela Cardoso de Matos; PEREIRA, Silva de Oliveira. Public Policies and People with Disabilities: Human, Family and Social Rights. Salvador: EDUFBRA, 2011. Available at: <http://books.scielo.org/>
PIMENTEL, Susana Couto. Living with Down Syndrome in Inclusive School: Pedagogical mediation and concept formation. Petrópolis, RJ: Vozes, 2012. (Inclusive Education Collection)
SAAD, Suad Nader. Preparing the path of inclusion: dissolving myths and prejudices towards the person with Down Syndrome. 1. Ed. São Paulo: Vetor, 2003.
PUESSHEL, Siegfried (Org.). Down Syndrome: A Guide for Parents and Educators. Trad. Lúcia Helena Reily. 2. Ed. Campinas, SP: Papirus, 1995. (Special Education Series)
LANNA JUNIOR, Mario Cléber Martins. The First Actions and Organizations focused on the person with Disabilities. Bengal Legal, 2011. Available at: <http://www.bengalalegal.com/asprimeiras-historia-pcd> Accessed on 11 September 2015.
MELO, Sandro Nahmias. The right to work of the person with a disability: affirmative action; the constitutional principle of equality. São Paulo: LTr, 2004. P.110.
ARAUJO, Luiz Alberto David. The constitutional protection of persons with disabilities and compliance with the principle of the dignity of the human person. 4. Ed. Brasília, 2011.
FÁVERO, Eugênia Augusta Gonzaga. Rights of persons with disabilities: ensuring equality in diversity. Rio de Janeiro: WVA, 2004. P. 37-38.
News Blog Brazil. Pestalozzi movement. Available at <http://brasilblog.com.br/?p=2622> Access in September 2015.
Association of parents and friends of the exceptional. Who we are. Available at <http://www.apaebji.org.br/sobre-a-apae/quem-somos> Access in September 2015.
PADILHA, A. M. Lunardi. Pedagogical Practices in Special Education: The capacity to signify the world and the insertion of the mentally retarded. 2 ed. Campinas: FAPESP, 2005.
CANNING, Claire D .; PUESCHEL, Siegfried M. Developmental expectations: panoramic view. In: PUESCHEL, Siegfried M. (Org.). Down Syndrome: A guide for parents and educators. 14. ed. Translation by Lúcia Helena Reily. Campinas, SP: Papirus, 2012. P. 105-114.
MENDES, E.G. The radicalization of the debate about school inclusion in Brazil. Rev. Bras. Educ., Rio de Janeiro, v.11, n.33, 2006, p. 387559http: //www.scielo.br/pdf/rbedu/v11n33/a02v1133.pdf> .Access on: 10/24/2015.
MTE, Ministry of Labor and Employment. Inclusion of people with disabilities in the labor market. 3. ed. Brasília, 2009.
CELL THERAPY OR CELLULUERY. Available at: <http://www.down21.org/salud/terapias/terapia_decelulas.htm. Accessed on October 20, 2015.
PORTAL EDUCATION. Down Syndrome: The importance of follow-up by a speech-language pathologist. Available at: <http://www.portaleducacao.com.br/fonoaudiologia/artigos/51796/sindrome-de-down-a-importancia-do-acompanhamento-de-um-fonoaudiologo#ixzz3pXJtw1FT. Accessed October 18, 2015
III National Conference on the Rights of Persons with Disabilities. “A look through the UN Convention on the Rights of Persons with Disabilities: New Perspectives and Challenges.” Brasilia DF. December 2012. Available at: <http://www.pessoacomdeficiencia.gov.br/app/sites/default/files/arquivos/%5Bfield_generico_imagens-filefield-description%5D_4.pdf>. Accessed on October 15, 2015.
DICTIONARY POUNDS. Available at: <http://www.dicionariolibras.com.br/website/artigo.asp?id=2608> Accessed on October 20, 2015.
ANNEX A – Roadmap for semi-structured interviews
SEMI-TRAINED INTERVIEW SCRIPT
1. QUESTIONS TO THE DIRECTOR OF THE CECOFII INSTITUTION
- How long do you work with people with special needs?
- What is your opinion about the social inclusion of special students in regular school?
- In your opinion, what barriers still exist for inclusion?
- How do you coexist with special people, especially those with Down Syndrome?
- What do you think about the Contribution of the State to people with special needs?
2. QUESTIONS ELABORATED FOR PARENTS
- How was the Gestation?
- Was the delivery normal or cesarean, had any occurrence?
- After the birth, how was the news that your daughter was special?
- And how was the acceptance?
- How old was the treatment and how was it for school inclusion?
- What do parents expect for their daughter in the future?
[1] Monograph presented at the Latu Sensu Post-Graduation Course, Specialization in MBA in Public Management and Government Management, as part of the requirements for obtaining the title of Specialist in Public Management and Government Management by Escola Paulista de Direito (EPD).
[2] Specialist in Public Management and Governmental Management
[3] Inclusion requires a transformation of the school, as it advocates the inclusion in the regular education of students with any deficits and needs. Inclusion requires breakdowns. In the educational system of inclusion it is the school’s responsibility to adapt to the needs of the students and not the students to adapt to the model of the school. WERNECK, Claudia: No one else is going to be Nice in the Inclusive Society. Rio de Janeiro: WVA, 1997 p.53.
[4] MELERO, M. L. (1999). Learning to know people with Down syndrome. Málaga: Aljibe Editions.
[5] Cellular treatment for Down’s Syndrome consists of a series of suspensions of base cells from 12 infections administered different parts of the fetal brain, such as the forebrain, midbrain, thalamus, etc., mixed in certain proportions. Injections are given every 5-6 months into adulthood. It is said that in Down syndrome other organs are affected beyond the brain due to a metabolic defect existing on the surface of cells, and that the syndrome is not due to the presence of an abnormal chromosome but, instead, the chromosome supernumerary is another symptom of the disease, and can even be repaired. Therefore, it is recommended that the cell treatments complementary suspensions of other organs are applied.
[6] CANNING, Claire D .; PUESCHEL, Siegfried M. Developmental expectations: panoramic view. In: PUESCHEL, Siegfried M. (Org.). Down Syndrome: A guide for parents and educators. 14. Ed. Translation by Lúcia Helena Reily. Campinas, SP: Papirus, 2012. P. 106.
[7] The professional speech therapist attends the child with DS and also the family of the patient and with the other professionals who deal with him, it is always very clear the principles of the treatment to be performed. It is imperative that everyone involved be aware very early on that the child with DS will always have the desire to communicate, despite the difficulties, and that this will be possible thanks to the treatment with the Speech-Language Pathologist and the participation of the family.
[8] The family that has people with mental disabilities, they always have a primary caregiver, and financially responsible, and if the caregiver works, it also has more caregivers to take to the doctor’s office. Children and youngsters generally spend most of their day in rehabilitation institutions. Characteristic features observed in psychopathological conditions such as autism, psychosis and severe dementia are confused with those of mental deficiency, leading to misunderstandings in their diagnosis (Cavalcante 1997 , p.17).
[9] The National Council for the Rights of Persons with Disabilities (Conade) is a high-level collegial deliberation body created to monitor and evaluate the development of a national policy for the inclusion of persons with disabilities and of education, health, labor, social assistance , transportation, culture, tourism, sport, leisure and urban policy aimed at this social group. Conade is part of the basic structure of the Human Rights Secretariat of the Presidency of the Republic (SDH / PR).
[10] The United Nations Convention on the Rights of Persons with Disabilities was ratified in 2008 by Brazil with the equivalence of Constitutional Amendment, which is the whole struggle of this population. By placing the disability policy on the Human Rights portfolio, the Federal Government recognizes that inclusion is, above all, a right won by this segment of the population from a lot of struggle.
[11] These institutions, which functioned as boarding schools, were inspired by the precepts of the Enlightenment ideology and had as their central objective to insert their students into Brazilian society by providing them with the teaching of letters, sciences, religion and some manual crafts.
[12] The sign language was brought by the Frenchman Hernest Huet in 1857, when he came to Brazil at the invitation of Dom Pedro II, to establish the first school for deaf boys, the Imperial Institute of Deaf-Mutes, Deaf (Ines), in Rio de Janeiro.
[13] Since the installation of a Rehabilitation Center required a highly specialized team, ABBR’s Technical Council and Board initially chose to establish a school for the training of physical therapists and occupational therapists – the first in the country of higher education. In more than half a century of activities, ABBR rehabilitated more than 400,000 people with disabilities.
[14] The beginning of the Pestalozzian Movement in Brazil occurred in 1926 in the city of Porto Alegre with the creation of the Pestalozzi Institute of Canoas, in the State of Rio Grande do Sul, by Professor Thiago Würth. The Institute was transferred three years later to the city of Canoas and was created with a focus on the care of people with learning difficulties.
[15] The Apaeano Movement is a great network that encompasses thousands of people who together fight for the defense of a cause: the improvement of the quality of life of the disabled person. Citizenship, justice, education, union, are the slogans of parents, friends and people with disabilities that unite love and professionalism to reduce social exclusion.
[16] The Education Guidelines and Bases (LDB) Law Defines and regulates the Brazilian education system based on the principles of the constitution. It was first cited in the 1934 Constitution and created in 1961 (4024/61). Based on the principle of the universal right to education for all, the 1996 LDB brought a number of changes from earlier laws, such as the inclusion of early childhood education (day care and pre-school) as the first stage of basic education. (Including also special education)
[17] TORRES GONZÁLEZ, José Antonio. Education and diversity: didactic and organizational bases. Porto Alegre: Artmed Editora, 2002.
[18] RIBEIRO, Julia Cristina Coelho. (2006). Meanings in inclusive school – A study on the conceptions and practices of teachers involved with school inclusion. Thesis of Doctorate, University of Brasilia. Brasilia / DF. Available: http: //repositorio.bce.unb.br/bitstream/10482/3288/1/J%C3%BAlia%20Cristina%20Coelho%20Ribeiro.pdf
[19] According to the Ministry of Labor and Employment (2009, p.17) affirmative action is considered to be “measures aimed at the implementation of mandatory or optional measures, from public or private bodies, whose purpose is to promote the inclusion of groups notoriously discriminated against, allowing them access to social spaces and the enjoyment of fundamental rights, with a view to achieving effective constitutional equality. ”
[20] And in accordance with the Consolidation of Labor Laws No. 5,452 / 43, Art. 2º “It is considered an employer, individual or collective company, who, assuming the risks of economic activity, admits, assaults and directs the personal service provision” and Art. 2º § 1º “For the exclusive purpose of the employment relationship, professionals, charitable organizations, recreational associations or other non-profit institutions, who admit workers as employees, are provided to the employer.”
[21] We need to evolve from the beautiful speeches to the implementation of public policies that result in the guarantee of the rights of people with disabilities, showing that beyond their limits is the consequent possibility of overcoming. Inclusion as a planned, gradual process must be a commitment of the whole society, sharing responsibilities between governmental and non-governmental organizations aimed at guaranteeing the dignity of the human person as the foundation of a free, democratic and just society. (SOUZA, 2006). Available at: <http://jus.com.br/artigos/39159/os-direitos-das-minorias.>
[22] MICHELS, L. R. F. The Concept of Inclusion and its impact on education. In: VI Seminar on Research in Education in the Southern Region – ANPEd Sul, 2006, Santa Maria. VI Seminar on Research in Education in the Southern Region – ANPEd Sul. Postgraduate in education: New issues. Santa Maria: UFSM, 2006. v. 1. P. 1-15.