ORIGINAL ARTICLE
SANTOS, Ada Marinho dos [1], BARBOSA, Andressa Oliveira [2], GOMES, André da Silva [3]
SANTOS, Ada Marinho dos. BARBOSA, Andressa Oliveira. GOMES, André da Silva. Manifestations of COVID-19 in public health collaborators from Açailândia – MA. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 06, Ed. 08, Vol. 01, pp. 89-122. July 2021. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/manifestations-of-covid-19
ABSTRACT
COVID-19 affects different people and its action acts differently, so most infected people do not need to be hospitalized. The most common symptoms are: fever; dry cough; tiredness. In this bias, the fundamental question of this study is to find out what was the behavior of the symptoms of COVID-19 in public health collaborators from Açailândia – MA. This study aims to provide a survey of data of employees followed with symptoms of COVID-19 from April to October 2020 on the behavior of symptoms of COVID-19 in health professionals of a Public Institution. This descriptive study is a documentary, quantitative research, based on secondary data, based on the period from March to October 2020, with a sample of 256 employees (129 answered the questionnaire) from a public institution located in the municipality of Açailândia/MA. It is worth informing that in the months of greatest contamination there were no specific protocols and medications, and because it is a recent disease, drug therapy and guidance were used by the benefit risk. In addition, an important factor is due to the fact that most professionals start treatment early. The results showed that most professionals who presented symptoms of COVID-19 are female, totaling 82.9%. Azithromycin (79.8%), dipyrone (63.6%), ivermectin (64.3%), among others, stands out for medications used during treatment. Most workers, i.e., 62.8% did not have any chronic disease. In addition, it was found that 92.2% did not need to be hospitalized for complications after COVID-19. Finally, it is concluded that if treatment is started early and when there is adequate follow-up the risks of complications are reduced. Regarding symptomatology, the main complaints were: fever; dry cough; headache; nasal secretion/sneezing; sore throat; respiratory distress; pain in the body; absence of taste or bitter mouth; weakness; insomnia; chest pain; pain in the lumbar region; pain when urinating; reduction of sexual libido, among others.
Keywords: COVID-19, Behavior, Symptoms, Treatment, Health Professionals.
1. INTRODUCTION
At the end of 2019, more precisely in the city of Wuhan in China began to appear a very high number of cases of pneumonia, which later drew the world’s attention to this new disease. From this period on there has been much discussion about the new coronavirus (SARS-CoV-2) and the disease it causes (SANTOS et al., 2020).
According to the World Health Organization (2020) there are currently confirmed cases of COVID-19 spread across all continents. The official terms for the new coronavirus and COVID-19 were published through the World Health Organization on February 11, 2020, defined as follows: Disease – COVID-19 (“Coronavirus Disease” 2019); Virus – Severe Acute Respiratory Syndrome Coronavirus 2 .
According to Brasil (2020), even most people affected by COVID-19 have mild or uncomplicated symptoms, others already develop severe disease that requires oxygen therapy (14%), and approximately 5% need treatment in the Intensive Care Unit (ICU). In addition, in relation to critically ill patients, the vast majority need mechanical ventilation.
With the emergence of several doubts about this disease and its mutation, accompanied by a very varied range of information on the subject, it is necessary to give the necessary focus to well-informed nursing and prepared to act in the care of new cases of the disease in specialized care and at all levels of care in a safe way (OLIVEIRA et al., 2020).
COVID-19 affects different people and its action acts differently. A good part of the infected people practically do not need to be hospitalized. Thus, the most common symptoms are: fever; dry cough; tiredness. On the other hand, there are other symptoms that can be considered: headache, diarrhea, sore throat, pain, loss of taste or smell, conjunctivitis, discomfort, skin rash and discoloration of the fingers or toes (TEIXEIRA et al., 2020).
Health professionals actively represent a risk group for Covid-19 because they are exposed daily to infected patients, which causes them to be susceptible to a large viral load (millions of virus particles). In addition, they are exposed to a high burden of stress when examining these patients, as many are in serious condition, in inadequate situations (SANTOS et al., 2020).
It is necessary to highlight that the health workforce is not homogeneous, because the difference in gender, race and social class stands out, structuring access to the various levels and courses of professional training, acting in the same way of work relations in health services at the same time as opportunities for insertion in the labor market (TEIXEIRA et al., 2020).
Health professionals and workers are directly at the forefront, with a higher risk of contagion, the difference that defines these health agents determines different forms of exposure, both to the risk of contamination and to the factors associated with working conditions (TEIXEIRA et al., 2020).
In this bias, the fundamental question of this study is to find out what was the behavior of the symptoms of COVID-19 in public health collaborators from Açailândia – MA.
Finally, the aim of this study is to provide a survey of data of employees followed up with symptoms of COVID-19 from April to October 2020 on the behavior of COVID-19 symptoms in health professionals of a Public Institution.
2. METHODOLOGY
This descriptive study is a documentary, quantitative research based on secondary data.
According to Gil (2011, p. 51), “documentary research is based on materials that have not yet received an analytical treatment, or can be reelaborated according to the objectives of the research”. Therefore, through a letter sent to the person responsible for the Public Health Institution, follow-up can be carried out with professionals who presented symptoms of COVID-19, acquiring information pertinent to the treatment of each professional.
On the other hand, for Richardson (1999), a quantitative research is characterized by employing elements of quantification in the collection of information and in the treatment of them through statistical techniques. Thus, Google forms doc was used to elaborate graphs, facilitating the visibility of information to present the situational picture of said search.
The municipality in question is Açailândia/MA, where the inhabitants are called açailandenses. The municipality extends for 5,806.4 km² and had 113,121 inhabitants in the last census (2020). The population density is 17.92 inhabitants per km². Close to Cidelândia and São Francisco do Brejão, the city of Açailândia is located 64 km north-west of Imperatriz. It is located at 231 meters of altitude, the geographical coordinates of Açailândia: Latitude: 4° 57′ 14” South, Longitude: 47° 30′ 7” West.
The climate is tropical. In winter, there is much more rainfall than in summer, being classified as Aw. The average annual temperature in Açailândia is 25.9 °C. 1334 mm is the average annual rainfall.
The study was conducted with 256 employees (only 129 answered the questionnaire) all followed by the period from March to October 2020. The employees were: nurses, nursing technicians, radiology technicians, receptionists, porters, maqueiros, general services, administrative sector, nutrition service, biochemists, social worker, laboratory assistant, maintenance service, drivers and pharmacy assistant.
Therefore, it is important to highlight the inclusion and exclusion criteria of this research. The inclusion criteria were: professionals who presented symptoms of COVID-19 and who were working at the Public Health Institution in the municipality of Açailândia/MA. Exclusion criteria were: professionals who did not present symptoms of COVID-19 and who were not crowded in the Public Health Institution in the municipality of Açailândia/MA.
The instrument used was the documental analysis, through Google forms doc, where information was collected from employees, such as age, gender, symptoms presented, month that initiated the symptoms suggestive of COVID-19, medications consumed, vitamins used, etc. Thus, the archives of the institution containing the information about the guidelines used in pandemic situations were indispensable to respond to the problem and objectives.
The research was carried out after approval by the Research Ethics Committee (CEP), and respected the research standards involving human beings, Resolution No. 466/12 of the National Health Council.
The data were recorded and analyzed through descriptive, percentage and distribution, using the Excel Program 2013®, for its elaboration. For the descriptive analysis of the variables, simple frequencies and percentages were used, as already mentioned.
3. RESULTS AND DISCUSSIONS
Given the world scenario experienced with the Pandemic by the New Coronavirus (SARS-CoV-2), it was necessary to take numerous prevention and control measures to prevent or reduce transmission within a Public Institution as much as possible in order to prevent the spread of the virus among employees and patients.
At first, it began with the organization of the Health Service and guidance to employees following technical note GVIMS/GGTESS/ANVISA no. 04/2020. Guidelines for Health services: prevention and control measures that should be adopted during the assistance of suspected or confirmed cases of infection by the new Coronavirus (SARS-CoV-2).
The guidelines on measures were emphasized in March 2020:
- Standard Precaution (Hand hygiene, use of gloves and aprons, glasses and surgical mask);
- Contact Precaution (Hand hygiene, apron, gloves and private room);
- Guidelines on the placement and removal of EPI;
- Attendance with criteria for screening respiratory symptoms to those who traveled abroad or had contacts with people with suspicion or positive for COVID;
- Mandatory use of mask in the premises of the Public Hospital of Açailândia and care measures;
- Availability of surgical mask to all respiratory symptomatic patients who tolerate the use of the mask;
- Adequate transport to patients with suspected or confirmed COVID;
- Coronavirus State Contingency Plan (State of Maranhão).
The educational activities began between March 13 and 14, permanent education together with CCIH developed pandemic-related guidelines for the health institution of COVID – 19. The frequency of the educational activity passed on to prove presence was suspended following the guidelines of the ANVISA Protocol, suspending activities that maintained increased contact and agglomerations among employees. The face-to-face activities of Permanent Education, internships from all sectors in the premises of the Public Hospital of Açailândia that were scheduled were suspended as a control measure. Thus, it began with guidance by electronic means (WhatsApp, official Instagram of the city), radios, TV among others.
The guidelines to the employees were clear and objective in order to reinforce the importance of measures to prevent the transmission of Coronavirus within the Hospital and Home Institution. The protocols of the Ministry of Health, Technical Notes GVIMS/GGTES/ANVISA, Epidemiological Bulletin n°08, Joint Technical Note 01/2020 were used as scientific theoretical basis: use and distribution of rapid tests for COVID-19 (CONASS- National Council of Health Secretariat) and measures were taken to strengthen surveillance and health care to all.
At the end of March came the first suspicious case in the municipality, with this was further reinforced the guidelines on prevention and control measures to avoid or reduce the transmission as much as possible, since then began to organize the flow of care within the institution according to demand. All employees who made trips interstate, outside or had contact with positive cases were isolated to comply with home isolation.
In April 2020, the first confirmed case of COVID-19 was identified among professionals of the Public Hospital of Açailândia. With this, the contact measures through the reduction of agglomerations were more rigorous, changing the entire context of the guidelines.
The flow of care within the Hospital Unit was reorganized according to the symptoms presented by each employee, such as self-assessment, rapid test schedules for COVID-19, visits to the doctor and other guidance. In order to better serve everyone and avoid complications all guidelines and flowcharts were delivered to the coordinators of each sector of the Public Hospital of Açailândia, Emergency mobile care service, Transport Sector, some employees of the Health and City Hall secretariat.
With the rapid growth in the number of suspected and confirmed cases of COVID-19, it peaked at the end of April and the entire month of May, beginning to regress to suspected or confirmed cases in June.Continuing Education was relocated throughout the pandemic period, supporting professionals via cell phone (calls and messages via WhatsApp), symptomatology monitoring with the objective of reducing complications, rapid test schedules for COVID, schedules for medical evaluation (at the beginning of the symptomatology, receiving the test result and at the end of isolation), cases observed with symptoms suggestive of complications were instructed to seek the Reference Center in the Municipality of origin.
At first, the rapid test for COVID-19 was made available to active health professionals (care and management services), public safety professionals (Fire Department Team, police officers, among others) and their families (with home contact) and symptomatic elderly. It is worth noting that the tests available at the time were antibodies, so the deadline for performing them began to be scheduled on the 8th day after the onset of symptoms according to the CONASS protocol, however it was observed that the symptomatic employees were presenting negative testing and for safety and return to service began to test them on the 14th day after the date of the first symptoms and it was observed that some who negatively tested them in the 1st test, positive in the 2nd test, so we chose to schedule only for 10 days after the date of the first symptoms. As the rapid test for COVID-19 (SARS-CoV-2) with IgG and IgM was not available, it was used on the basis of return of professional activities at least 72 asymptomatic hours, according to epidemiological bulletin n°08.
In addition to the clinical evaluation of the employees who were followed by cell phone daily, directions were made to each situation presented regarding home isolation, guidelines to which place to look for signs of complications. Some employees tested negative in the first test and later when performing Chest TC presented pulmonary involvement with approximately 25 to 35%, with a matte glass aspect suggestive for COVID because it correlates with the employee’s clinic.
The medical team responsible for accompanying the employees were instructed to follow the protocols for care of health professionals, even though it was not a reference of care for COVID-19, we sought to make the first care to start drug therapy, request for rapid testing for COVID and, if necessary, complementary tests. The second evaluation was on the day of the rapid test for COVID-19 for examination delivery and reassessment of the employee. The third evaluation was scheduled for the end of the professional’s leave and the consultation with prior appointment with the Medical Board of Workers’ Health.
The rapid testing of COVID-19 for family members in home contact of employees was also scheduled in the laboratory of the Public Hospital of Açailândia, and as this unit is not considered as a reference for COVID medical follow-up began to be scheduled in the Basic Health Units of reference for mild cases, and for more severe cases were directed to UPA, Campaign Hospital or ICU in the premises of the Public Hospital of Açailândia.
With daily monitoring of health professionals, the need for medical evaluation was classified according to the symptomatology of each one, when complications were observed, they were referred for evaluation at the UPA (observation or even hospitalization), and could be referred to the isolation beds of the Public Hospital of Açailândia , Hospital Campaign with cases of moderate symptoms, and ICU severe cases.
The return evaluation was scheduled with 15 days or more, according to the protocol for three days of asymptomatic to return to the service, as we did not have a rapid test (SARS-CoV-2) with specific IgG and specific IgM available or even serology to be performed before the return, we decided to use the protocol of return of health professionals to the CONASS service.
The entire management team, committees and coordinators mobilized in order to better serve and guide all employees. The attested were not being delivered by hand, only by e-mail and we had the support of the medical staff of the Hospital Unit and Work Doctor, all had a huge contribution in the evaluation of employees and delivery of medical certificate to complete the period of leave.
It is notepoint that even in view of all the orientations given to professionals, anxiety, anguish, despair and fear of contagion by the new Coronavirus can be observed, fear of contaminating a loved one, fear of death, because they are directly involved in the process of illness and care, from this finding we sought to offer psychological follow-up to employees who required qualified listening and obtained mental health support with the psychologist crowded in the CAPS (Psychosocial Care Center).
Topics addressed in April, May, June and July in Continuing Education:
- Guidelines for health services: prevention and control measures that should be adopted during the assistance of suspected or confirmed cases of infection by the new Coronavirus (SARS-CoV-2);
- Hand washing, videos via WhatsApp;
- Public Health Emergency of National Importance for Coronavirus Disease 2019;
- Mental Health and Psychosocial Care in the COVID-2019 pandemic;
- Technical Note regarding the care of the nursing team in obstetrics, neonatal and pediatric in the face of a suspected or confirmed case;
- Mental Health and Psychosocial Care in the COVID-2019 pandemic. Recommendations for Managers;
- Mental Health and Psychosocial Care in the COVID-2019 pandemic. Recommendations for the care of children in hospital isolation;
- Recommendations for Cardiopulmonary Resuscitation (RCP) of patients diagnosed or suspected for COVID-19;
- Guidance on the correct use of the mask;
- Guidelines on the placement and removal of personal protective equipment (PPE);
- Recommendations for Cardiopulmonary Resuscitation (RCP) of patients diagnosed or suspected for COVID;
- Informational banner about Coronavirus: learn how to prevent yourself;
- Monitoring of public health events: Technical note on recurrence of clinical picture of COVID-19 in health service professionals.
In August 2020, suspected or confirmed cases for COVID-19 began to reduce considerably, even though the follow-up of all employees was continued because they realized the continuity of some symptomatologies, however, with less intensity. In order to better monitor everyone and continue the service, a post-COVID-19 questionnaire was elaborated to identify possible complications.
The questionnaire was prepared in accordance with the Google forms doc program, with the theme: Evaluation of Employees with Symptomatology of COVID-19. Only the employees of the Public Hospital of Açailândia who were followed from March to October received a link containing the option with answers with multiple choice and some open for better explanation of the information. As they were being answered and had some option or annotation with a complicated signal, the employee was contacted by message via WhatsApp or call.
All cases identified as possible complication were referred for evaluation with thoracic surgeon/pulmonologist, general surgeon/vascular surgeon, orthopedist and clinical cases to physicians on duty of urgency and emergency.
It is also emphasized that the coordinators of each sector of the Hospital Unit had a huge contribution to a better follow-up of each employee.
According to follow-up performed with professionals who presented symptoms of COVID-19, the following results stand out:
Graph 01: What is your gender identity?
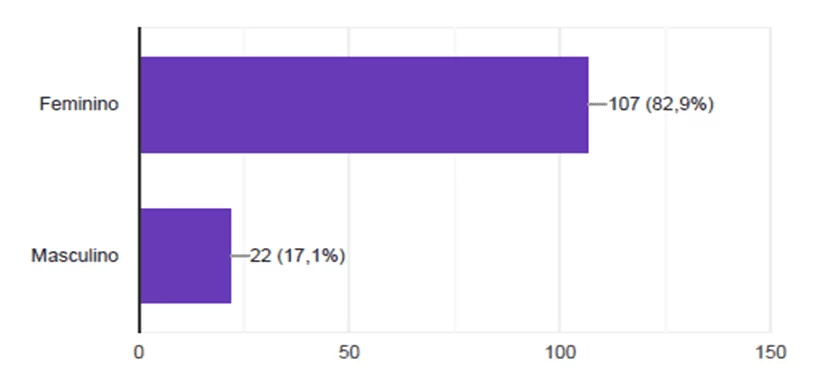
According to the first graph presented, it is noted that the vast majority of professionals of the Public Hospital of Açailândia who presented symptoms of COVID-19 are female, totaling 82.9%, and males were 17.1%. This information confirms what studies in general have been affirming for many years, in nursing women exercise great predominance.
According to Neves (2020), the nursing team is still predominantly female, being composed of 84.6% of women. It is important to emphasize, however, that even though it is a female category, it is the presence of 15% of men.
Graph 02: How old are you?
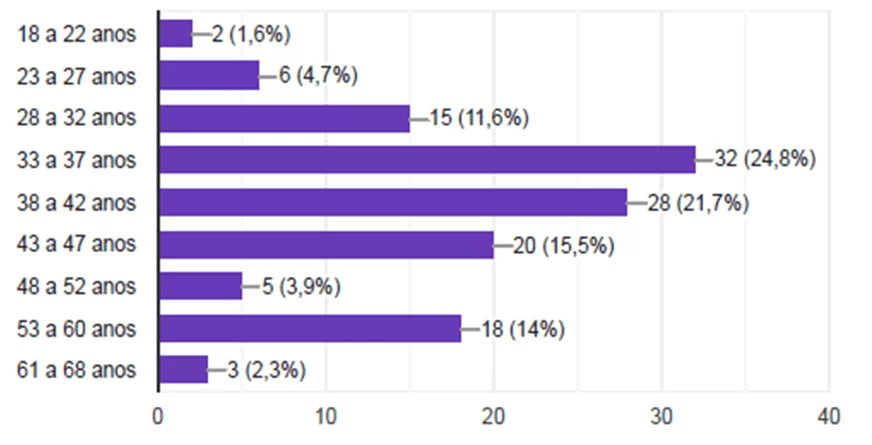
With regard to age, emphasis is placed on people aged 33 to 37 years (24.8%) and 38 to 42 years (21.7%). At the beginning of the pandemic, the news was that the symptoms more affect the older people, and over time a new context was observed. The World Health Organization (WHO) warned that Covid-19 does not only affect the elderly. Prevention and treatment measures should be employed by governments and people also in the case of healthy adults and even children (VALENTE, 2020).
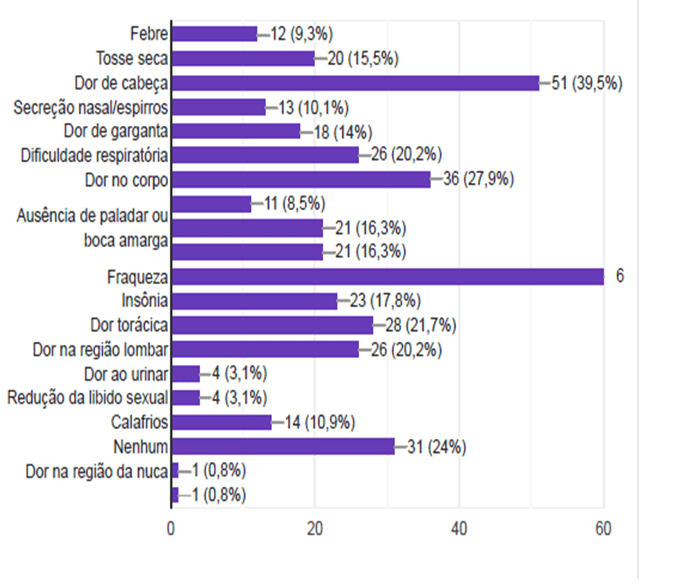
Graph 03: What symptoms did you present suggestive of COVID-19?
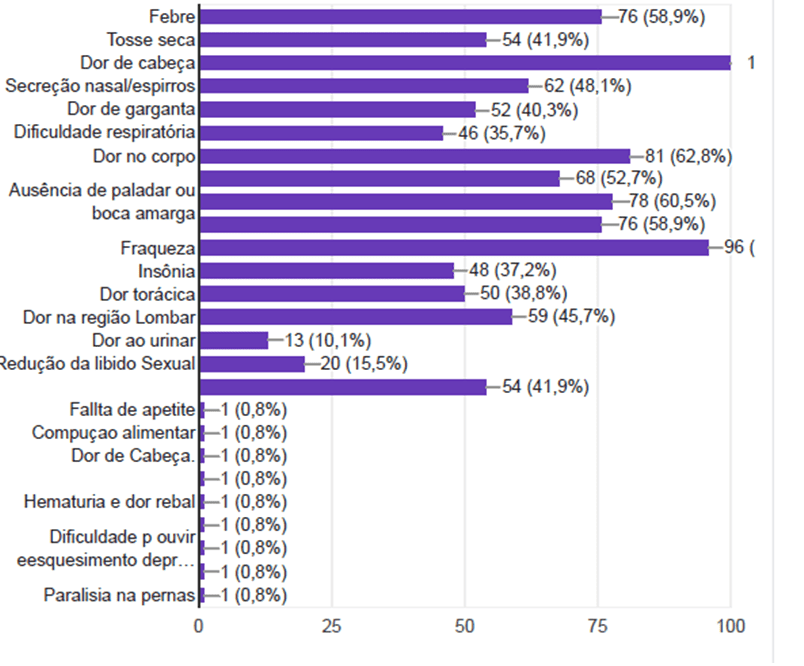
The symptoms presented by the professionals of the Public Hospital of Açailândia are quite varied, some with higher incidence, important to highlight the most common ones such as fever, headache, pain in the cup, weakness, insomnia, absence of taste, among others. According to Leachi; Ribeiro (2020), the infected person may present several symptoms, the most frequent being fever, followed by cough and bilateral pulmonary involvement of the lungs, which can be observed on computed tomography images.
It is important to mention that the Hospital has always promoted guidance to the employee in the face of suggestive symptoms for COVID-19, they are: fever; dry cough; headache; nasal secretion/sneezing; sore throat; respiratory distress; pain in the body; diarrhea, nausea or vomiting; absence of taste or bitter mouth and absence of smell.
Graph 04: What month started the suggestive symptoms for COVID-19?
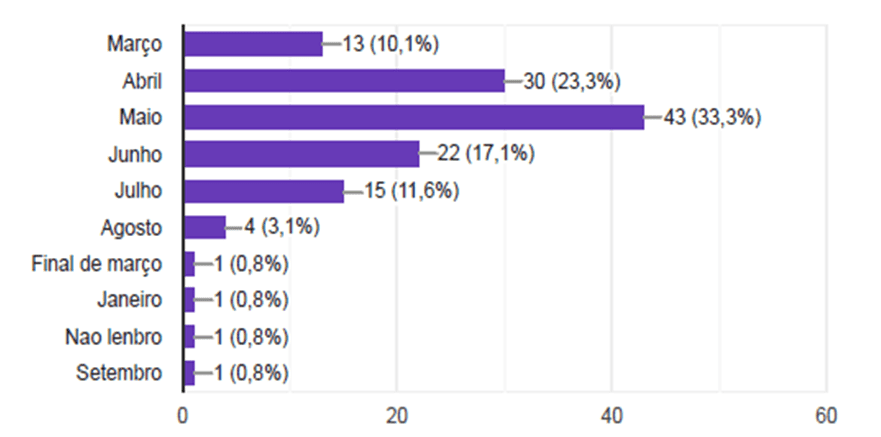
A prevalence of the number of cases was observed in May 2020 (33.3%). An important factor is due to the fact that most professionals seek or start treatment early. Suspected or confirmed cases were followed by trained professionals and within the health institution itself. Cases with less severity continue with home isolation and later receive medical discharge (BRASIL, 2020).
Graph 05: What month did you test for COVID-19?
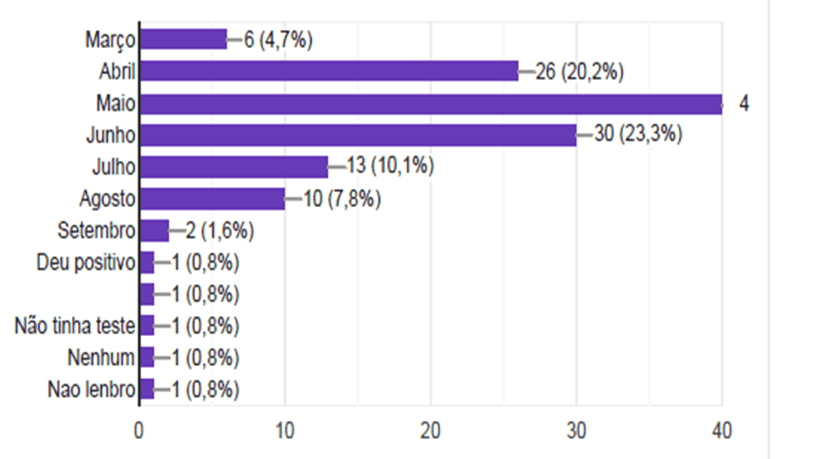
In May, it was the period in which more professionals performed the COVID-19 test because it was the month with the highest prevalence of cases (33.3%), followed by June (23.3%) and April (20.2%). It is important to highlight that only tests can be used in cases notified by the National Health Surveillance Agency, accompanied by an evaluation report from the National Institute of Health Quality Control of the Oswaldo Cruz Foundation (INCQS/Fiocruz). In addition, incubation time is essential for the effectiveness of testing, since infected people, but without yet manifestation of any of the symptoms, can continue to transit through the cities, with the risk of transmission of the virus in this asymptomatic period to contacts, and it is even highly likely that individuals will manifest symptoms, with the progression of the disease (BOLETIM EPIDEMIOLÓGICO 8, 2020).
Graph 06: What medications did you use as a treatment for COVID-19?
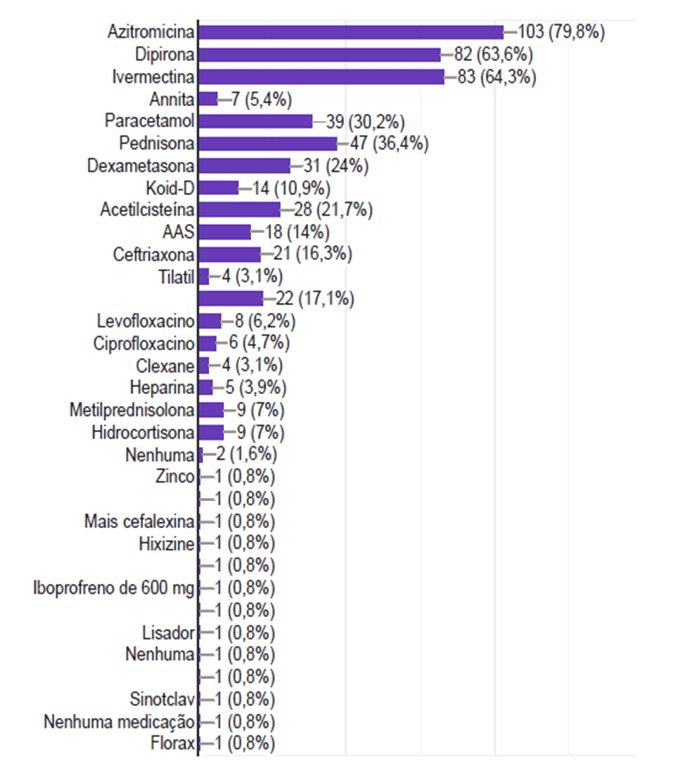
Regarding the medications used during treatment for COVID-19 by professionals, azithromycin (79.8%), dipyrone (63.6%), ivermectin (64.3%), among others, stands out. It is known that there is still a great lack of agreement on these medications for the treatment of COVID-19.
Graph 07: What vitamins did you use during treatment for COVID-19?
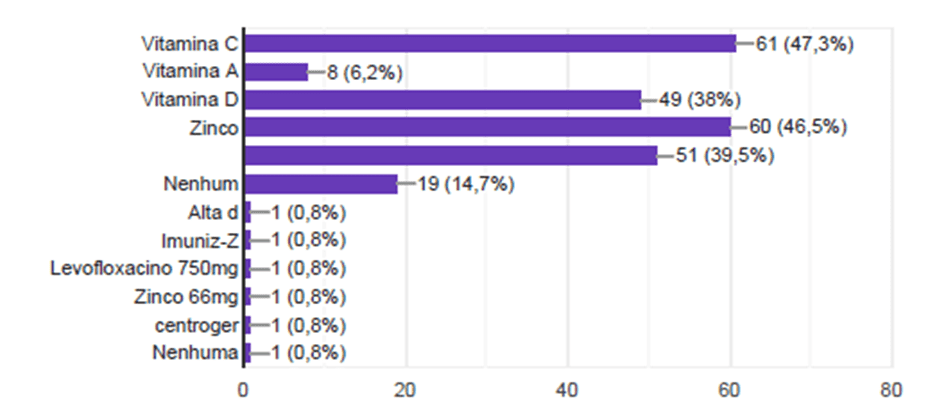
The most used vitamins were Vitamin C, where 47.3% used it, followed by Vitamin D and Zinc, 38% and 46.5%, respectively.
Graph 08: How long have you been away from service?
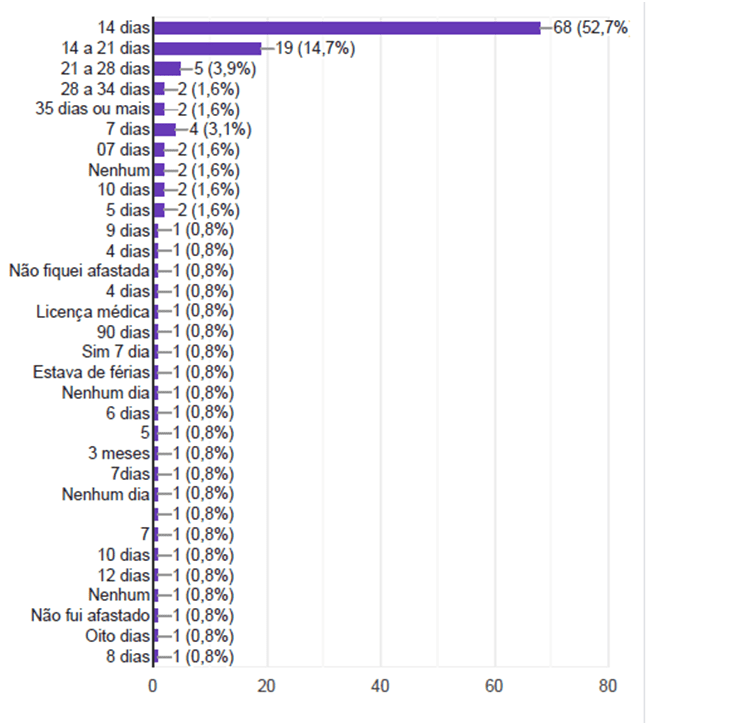
Most employees, totaling 52.7%, had to stay 14 away from work, others for longer, up to 21 days, totaling 14.7% of the workers.
The main health obstacle that affects workers who are in direct care those infected by COVID-19 is the high chance of being infected by the virus. There are several factors that show the high degree of exposure and contagion of health workers (TEIXEIRA et al., 2020).
Workers who offer their skills daily to health services also end up being exposed to workloads that are considered extremely exhausting and stressful, causing an illness. These loads are classified: biological, chemical, physical, mechanical, physiological and psychic (SILVA; FERRAZ; JÚNIOR, 2017).
Graph 09: Do you have any chronic disease?
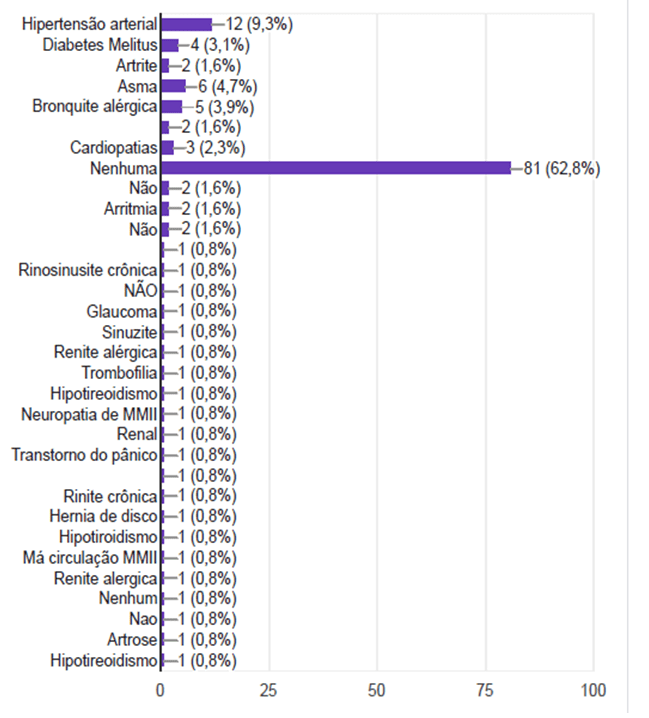
Most workers, that is, 62.8% had no chronic disease, only a minority had hypertension, diabetes mellitus, arthritis, asthma, allergic bronchitis etc. It is important to define the term chronic disease, it is used to designate pathologies with one common point: known to be persistent and require permanent care.
Hypertension is the most prevalent chronic disease in the population, causing high mortality and morbidity rates and lifelong maintenance treatment is required. Among the risk factors for hypertension, we have a lifestyle characterized by failed feeding, drinking habits, smoking, complemented by sedentary lifestyle (ANDRADE et al., 2015).
Diabetes mellitus is a chronic disease that is part of a group of metabolic diseases manifested through increased blood glucose or defect in insulin secretion by the pancreas and/or defect in the action of insulin in target organs (SBD, 2016).
Graph 10: Do you use continuous medication? If it is, which one?
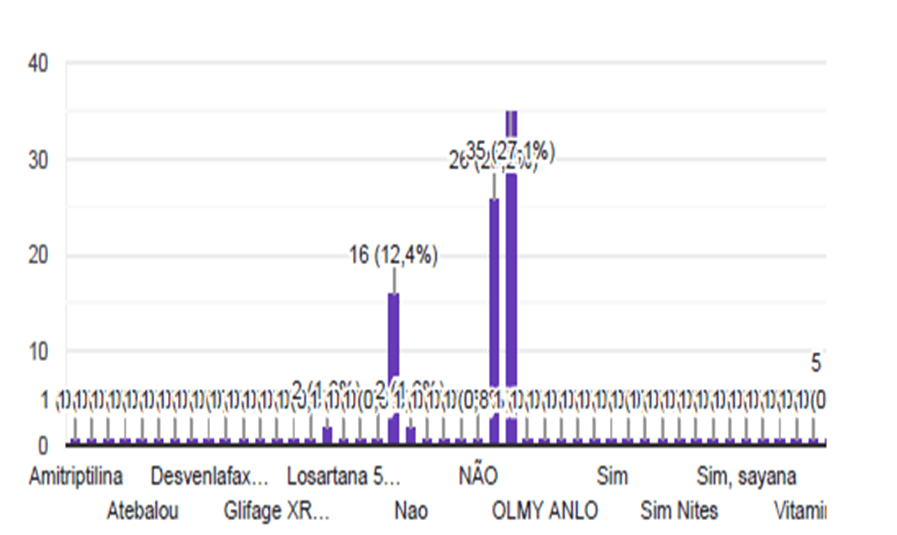
The professionals continued to use the medication for a good part of time, given, being followed up and evaluated gradually. In addition, the professionals were instructed never to self-medication.
Graph 11: Was there a need to seek hospital care during COVID-19 in addition to scheduled evaluations?
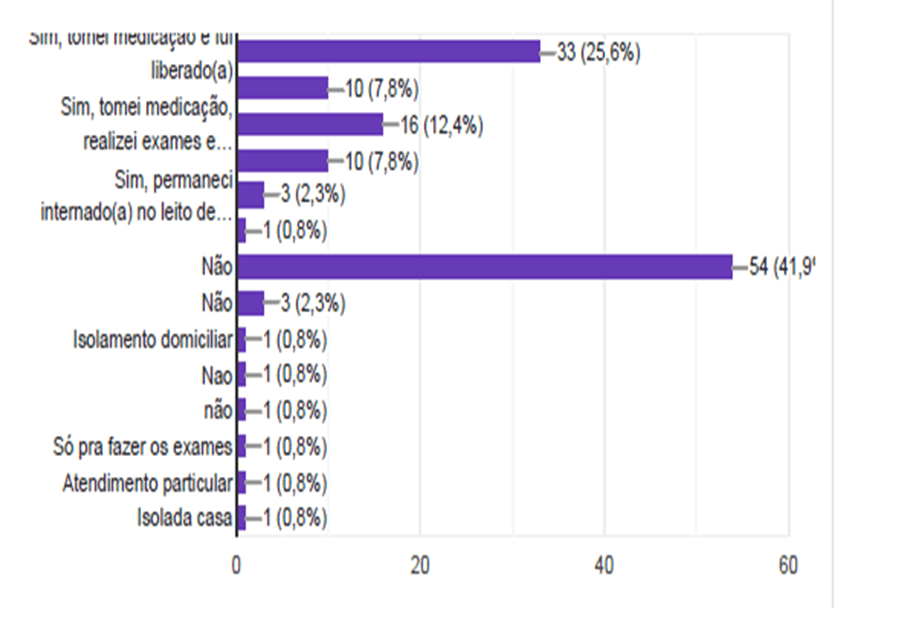
In this question, it can be seen that most of the professionals, totaling 41.9% did not need to seek hospital care during COVID-19 beyond the scheduled evaluations.
It is noteworthy that the flow of care within the Hospital Unit was reorganized according to the symptoms presented by each employee, such as proceeding for self-assessment, rapid test schedules for COVID-19, visits to the doctor and other orientations.
In order to better serve everyone and avoid complications all guidelines and flowcharts were delivered to the coordinators of each sector of the Public Hospital of Açailândia, SAMU, Transport Sector, some employees of the Health and City Hall secretariat.
Graph 12: If there was a need for hospitalization after complication by COVID-19, what was the reason?
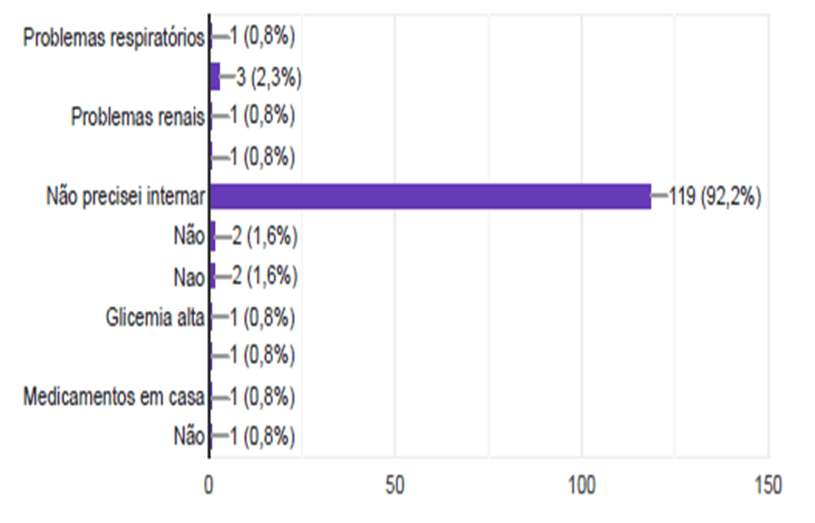
Only 2.3% needed hospitalization, on the other hand, 92.2% did not need to be hospitalized, because it was important all the support offered by the Public Hospital of Açailândia to these professionals.
Remembering that daily follow-up of health professionals was performed, the need for medical evaluation was classified according to the symptomatology of each one, when complications were referred for evaluation in the UPA, a reference unit in the municipality in question (observation or even hospitalization), and may be referred to the isolation beds of the Public Hospital of Açailândia or Hospital Campanha with cases of moderate symptoms, and ICU severe cases.
Figure 13: What tests did you take during follow-up in the first month of COVID-19?
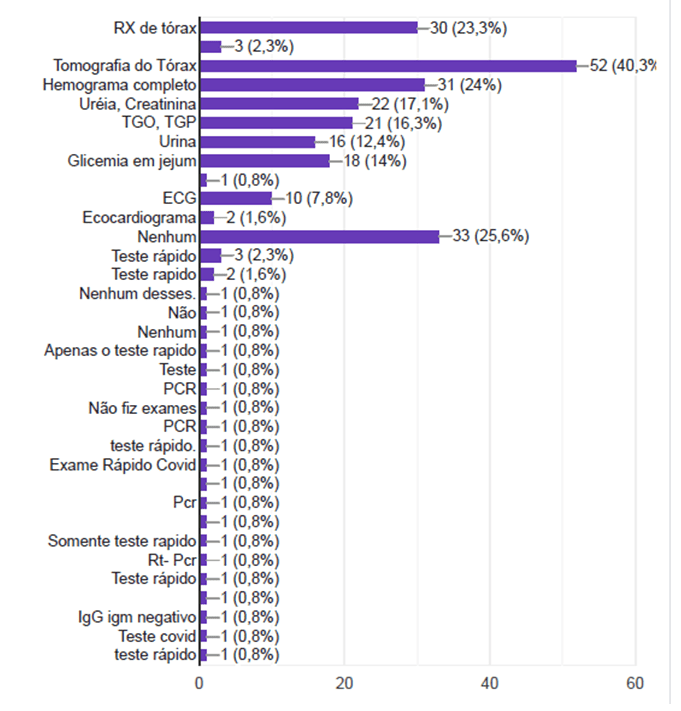
The main tests were chest X-ray, tomography, among others, but some professionals did not perform tests, which totaled 25.6%. We sought to make a daily follow-up of all employees according to the need, psychological evaluation in specific cases, laboratory tests, X-ray, chest tomography among others. The municipality made available the delivery of kits for COVID, leaving in the Internal Pharmacy facilitating access to employees, at first being delivered to 05 Basic Health Units that were prepared to receive the general population with suspicious or confirmed conditions for COVID, and later delivered to the Basic Pharmacy located in the Municipal Health Department.
Graph 14: What symptoms did you present suggestive for COVID-19 after the first 14 days of initiating symptoms?
Even after 14 days, some symptoms persisted, including fever, dry cough, headache, weakness, among others, but 24% did not present any more complaints.
Figure 15: Are you still using any medication after COVID-19? If so, which one?
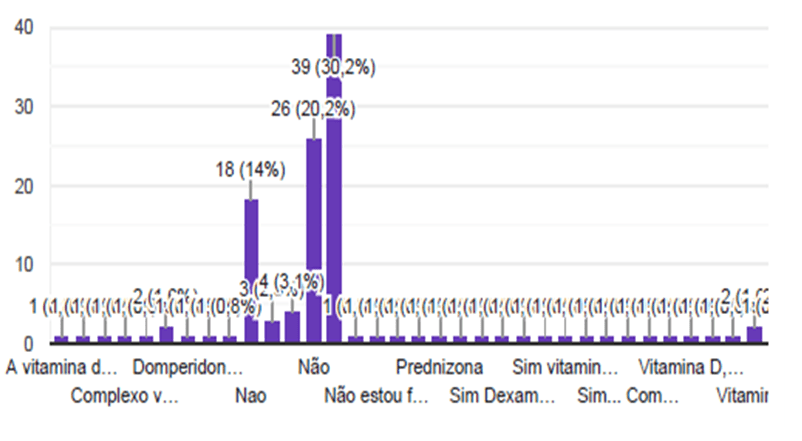
There are few employees who continued to use some medication, when it happened, it was domperidone, vitamin D, etc.
Graph 16: If you repeated the test for COVID-19 (rapid test or RT-PCR) after the first 14 days of initiating symptoms, what was the month?
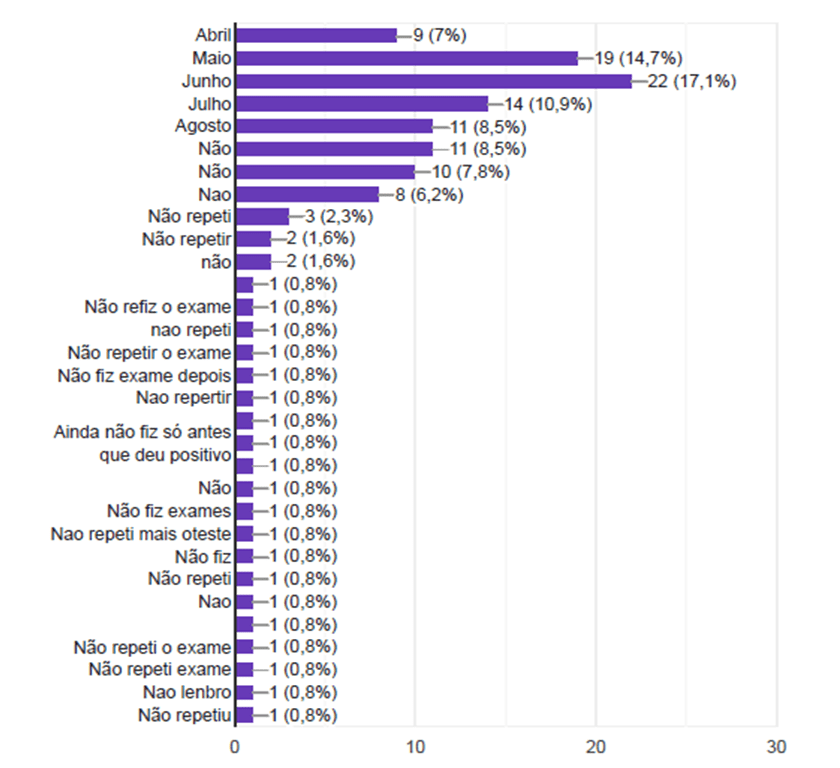
Regarding the repetition of the test for COVID-19 (rapid test or PCR) after the first 14 days of the first symptoms started, the most cited month was June, representing 17.1%.
The transmission rate of workers infected with SARS-CoV is commonly 7 days after the manifestation of symptoms. However, preliminary information from the New Coronavirus (2019-nCoV) indicates that contamination may occur, even if it is asymptomatic. Until then, there are not enough data to define how many days preceding the manifestation of symptoms the infected subject starts to spread the virus (BRASIL, 2020).
Graph 17: If you repeated the test for COVID-19 (rapid test or PCR) after the first 14 days of initiating symptoms, what was the result?
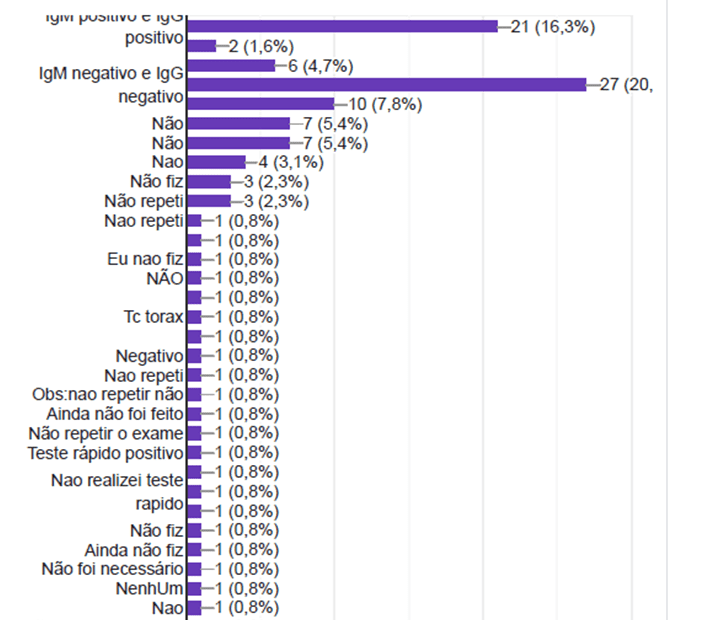
Most of the results, after repeating the test for COVID-19 (rapid test or PCR) after the first 14 days of initiating symptoms, were negative, totaling 20%.
Figure 18: From 01 to 10 how do you rate your health after COVID-19?
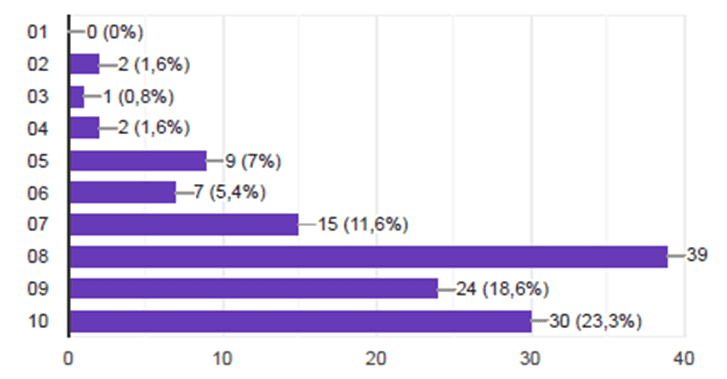
The recovery of COVID-19 is still unknown, but most professionals still reported a health that does not reach 100%, still needing more time for recovery.
4. FINAL CONSIDERATIONS
Some care is essential for the prevention of COVID-19, and they were daily scored with the Public Institution, mainly by professionals, who are on the front line, they are: hand washing, videos via WhatsApp; Mental Health and Psychosocial Care in the COVID-2019 pandemic; guidance for removal and return to the activities of health professionals; Home Isolation Booklet; nutritional guidelines to strengthen the immune system of health professionals; self-assessment of professionals to identify the symptoms of COVID-19; Informational banner about Coronavirus: Learn how to prevent yourself and Guidelines on the correct use of the mask.
The follow-up with symptomatic employees was completed in October 2020, thus passing any confirmed or suspected case to be followed only by the hospital clinical part and the rapid test schedules being carried out directly in the laboratory according to the presentation of the medical request.
The cases of complications continued with follow-up and scheduling with the physicians of the Public Hospital of Açailândia in order to better serve all. Thus, all documents completed during employee follow-up were filed in the HR sector.
The archived documents may in future be used as a source of bibliographic research for the publication of scientific articles as released by the General Board of the Health Institution.
The Public Health Institution will continue to maintain the necessary care recommended by the Ministry of Health/ANVISA for measures to control the spread of the virus and prevent a new cycle of infection within the Hospital Health Unit.
It was concluded that the employee, when followed from the beginning of symptoms, the complication was lower, and daily follow-up by a professional for 14 days or more was of paramount importance to avoid further complications. It was noticed that when there is an involvement of the multidisciplinary team, psychological follow-up and the patient is not treated only as the disease itself, a better prognosis is obtained.
The period of greatest distress was predominant mainly in the beginning of the pandemic, March, April and May 2020 were the most critical months, and the month of May and June was the month in which the highest number of cases of COVID-19 was found among employees.
REFERENCES
ANVISA – AGÊNCIA NACIONAL DE VIGILÂNCIA SANITÁRIA. Nota Técnica GVIMS/GGTES/ANVISA Nº 06/2020. Orientações para a prevenção e o controle das infecções pelo Novo Coronavírus (SARS-CoV-2) em procedimentos cirúrgicos – Revisão: 29.05.2020.
ANVISA – AGÊNCIA NACIONAL DE VIGILÂNCIA SANITÁRIA. Nota Técnica GVIMS/GGTES/ANVISA Nº 07/2020. Orientações para a prevenção da transmissão de COVID-19 dentro dos serviços de saúde. Brasília, 08 de maio de 2020.
ANVISA – AGÊNCIA NACIONAL DE VIGILÂNCIA SANITÁRIA. Nota Técnica GVIMS/GGTES/ANVISA Nº 04/2020. Orientações para serviços de saúde: medidas de prevenção e controle que devem ser adotadas durante a assistência aos casos suspeitos ou confirmados de infecção pelo Novo Coronavírus (SARS-CoV-2). Atualizada em 08/05/2020.
ANVISA – AGÊNCIA NACIONAL DE VIGILÂNCIA SANITÁRIA. Nota Técnica GVIMS/GGTES/ANVISA Nº 08/2020. Orientações gerais para implantação das práticas de segurança do paciente em hospitais de campanha e nas demais estruturas provisórias para atendimento aos pacientes durante a pandemia de COVID-19. Brasília, 13 de maio de 2020.
ANVISA – AGÊNCIA NACIONAL DE VIGILÂNCIA SANITÁRIA. Nota Técnica GVIMS/GGTES/ANVISA Nº 05/2020. Orientações para a prevenção e o controle de infecções pelo Novo Coronavírus (SARS-CoV-2) em instituições de Longa Permanência para Idosos (ILPI). Atualizada em 24/06/2020.
ANVISA – AGÊNCIA NACIONAL DE VIGILÂNCIA SANITÁRIA. Nota Técnica Pública CSIPS/GGTES/ANVISA Nº 01/2020. Orientações para a prevenção e o controle de infecções pelo Novo Coronavírus (SARS-CoV-2) em instituições de acolhimento. 24 de junho de 2020.
ANDRADE, Silvânia Suely de Araújo, et al. Prevalência de hipertensão arterial autorreferida na população brasileira: análise da Pesquisa Nacional de Saúde, 2013. Epidemiol. Serv. Saúde, Brasília, 24(2): 297-304, abr-jun 2015.
BRASIL. MINISTÉRIO DA SAÚDE. Secretaria de Atenção Especializada à Saúde. Departamento de Atenção Hospitalar, Domiciliar e de Urgência. Protocolo de manejo clínico da Covid-19 na Atenção Especializada [recurso eletrônico] / Ministério da Saúde, Secretaria de Atenção Especializada à Saúde, Departamento de Atenção Hospitalar, Domiciliar e de Urgência. – 1. ed. rev. – Brasília: Ministério da Saúde, 2020.
BRASIL. Secretaria de Vigilância em Saúde/Ministério da Saúde. Boletim epidemiológico. Doença pelo coronavírus 2019. 09 de abril de 2020/Semana Epidemiológica 15 (05-10/04).
BRASIL. Ministério da Saúde. Protocolo de Tratamento do Novo Coronavírus (2019-nCoV). Brasília – DF, 2020.
BRASIL. Ministério da Saúde. Diretrizes para diagnóstico e tratamento da COVID-19. Brasília – DF, 08 de abril de 2020.
ESTADO DO MARANHÃO. Secretaria de Estado da Saúde. Nota informativa CIEVS Nº 04/2020. São Luís, 13 de abril de 2020.
GIL, Antonio Carlos. Metodologia do ensino superior. 4. ed. São Paulo: Atlas, 2011.
Instituto Brasileiro de Geografia e Estatística – IBGE. Açailândia. Disponível em: https://cidades.ibge.gov.br/brasil/ma/acailandia/panorama. Acesso em: 25/03/2021.
LEACHI, H.F.L, RIBEIRO, R.P. Máscaras utilizadas pelos profissionais da saúde: o que é recomendado? Advances in Nursing and Health. [Internet]. 2020;2(1):2-7. Disponível em: http://www.uel.br/revistas/uel/index.php/anh/article/view/39757/27114. Acesso em: 26/03/2021.
NEVES, Úrsula. Perfil da enfermagem no Brasil: pesquisa faz levantamento da profissão. Disponível em: https://pebmed.com.br/perfil-da-enfermagem-no-brasil-pesquisa-faz-levantamento-da-profissao/. Acesso em: 25/03/2021.
OLIVEIRA, Edith Cibelle de. Et al. Sintomas clínicos de pacientes recuperados da COVID-19 em regiões da Amazônia Oriental. Revista Científica Multidisciplinar Núcleo do Conhecimento. Ano 05, Ed. 11, Vol. 04, pp. 57-65. Novembro de 2020.
PREFEITURA MUNICIPAL DE AÇAILÂNDIA. Secretaria Municipal de Saúde. Orientações para o isolamento domiciliar. Comitê Municipal de Prevenção, de Combate e Monitoramento ao COVID-19, 2020.
PREFEITURA MUNICIPAL DE AÇAILÂNDIA. Secretaria Municipal de Saúde. Plano Municipal de Contingência. Secretaria de Saúde de Açailândia Novo Coronavírus (COVID-19). Açailândia – MA, 2020.
RICHARDSON, Roberto Jarry. Pesquisa social: métodos e técnicas. São Paulo: Atlas, 1999.
SANTOS, José Natanael Gama dos, et al. Perfil dos profissionais de saúde acometidos pela covid19 no estado do Amapá-Norte-Brasil. Jornal de Ciências da Saúde – JCS HU-UFPI. Ed. Espec. 2020; 3(Supl.2):e-11288.
SANTOS, Genilson Gaudêncio dos. Et al. Atuação de enfermeiros no combate à COVID-19 no Estado da Paraíba: Um relato de experiência. Revista Científica Multidisciplinar Núcleo do Conhecimento. Ano 05, Ed. 11, Vol. 10, pp. 05-15. Novembro de 2020.
SOCIEDADE BRASILEIRA DE DIABETES. Diretrizes da Sociedade Brasileira de Diabetes- SBD /2019-2020. Disponível em: <https://www.diabetes.org.br/profissionais/images/diretrizes-completa-2019-2020.pdf>. Acesso em: 05/03/2021.
SILVA, Andressa; FERRAZ, Lucimare; JUNIOR, Sinval Adalberto Rodrigues. Ações em Saúde do Trabalhador desenvolvidas na Atenção Primária no município de Chapecó, Santa Catarina. Revista Brasileira de Saúde Ocupacional, 2016.
TEIXEIRA, Carmen Fontes de Souza, et al. A saúde dos profissionais de saúde no enfrentamento da pandemia de Covid- 19. Ciência & Saúde Coletiva, 25(9): 3465-3474, 2020.
VALENTE, Jonas. Covid-19 não é doença somente de idosos, alerta OMS. Disponível em: https://agenciabrasil.ebc.com.br/saude/noticia/2020-03/covid-19-nao-e-doenca-somente-de-idosos-alerta-oms. Acesso em: 25/03/2021.
WORLD HEALTH ORGANIZATION. Novel Coronavirus (COVID-19) Situation. 2020. Disponível em: https://who.maps.arcgis.com/ Acesso em: 08/02/2021.
[1] Specialist in Public Health (UEMA) and Specialist in Family Health (IBPEX), completing Master’s degree in Health Education (Polytechnic Institute of Coimbra – IPC, Portugal) – Nurse, Specialist in Health Management (UEMA), Multidisciplinary Nephrology UFMA – Specialist in Clinical Hematology.
[2] Graduation.
[3] Graduation.
Submitted: June, 2021.
Approved: August, 2021.















