ANDRADE, Nívea Cristiane de Sousa de [1]
ANDRADE, Nívea Cristiane de Sousa de. Epidemiological profile of Chagasic patients attended in reference Cardiology hospital in Belém/PA-Multidisciplinary Core scientific journal of knowledge. Year 1. Vol. 9. pp. 118-135, October/November 2016. ISSN. 2448-0959
SUMMARY
Currently the Stop is responsible for 80% of the records of cases of chagas disease in Brazil, has seen a growing increase of the disease in its acute form caused by oral transmission via ingestion of food contaminated by the faeces of triatomine or Skunk urine. Already the chronic cases of chagas disease, it has been documented in Palm collectors in extractive region of Rio Negro, in the brazilian Amazon. Aim profile of acute and chronic Chagasic patients attended at the Hospital de Clínicas Gaspar in Bethlehem in the period from January to December 2012; starting from the hypothesis that in the region, socioeconomic characteristics interfere with the mode of transmission of the disease. Descriptive methodology, quantitative approach, such as documentary instrument was used a screenplay with close-ended questions in 163 charts provided by the medical files and statistical service (SAME). The sample was made up of seven confirmed patients of wounds. The results 86% were male, 43% posuiam age over 50 years .57 percent married .71% had the color Brown, 57.14% were Evangelical, 42.85%, about 57% had no income, and being from the Northeast region of Tome Acu. Discussion were provided with main diagnostic records of 163 congestive heart failure and only two records with primary diagnosis of chagas disease This population seven confirmed patients with wounds. Final considerations on the unavailability of information this study becomes the basis for it to be expanded even to private health networks.
Key words: epidemiological profile. Chagas disease.
INTRODUCTION
In Stop the growing Association of oral transmission of the disease to humans causes concern. Says Guimarães (2012), that after having participated in health actions carried out b[2]y Pro Peace, 2011, Points2shop Island, close to Bethlehem, to detect that more than 50% of the people examined presented changes in heart rate was observed also that the locals knew the insect Barber, but didn’t know the severity of that “coexistence”; What we awakened desire to study this disease in our State.
For Hinrichsen (2006, p. 381), Mathew (2008, p. 123) and Nevis (2009, p. 142), chagas disease, also called American trypanosomiasis, is a malady endemic character, caused by a Protozoan flagellate, Trypanossoma cruzi (t. cruzi) that is transmitted to humans by infected feces of insects known as Triatominae. Chagas disease and its causative agent were discovered and described by scientist Carlos Ribeiro Justiniano das Chagas in 1909, in the small city of Lassance, situated in the North of the State of Minas Gerais.
Second vp/Panaftosa-PAHO/who (2009, p. 19), Trypanosoma cruzi is a parasite of many hosts and capable of infecting dozens of species of wild and domestic mammals belonging to eight different orders, with the birds and cold-blooded vertebrates refractories to the parasite.
Most species of Triatominae known live in the Middle, associated with a diversity of flora and fauna, and may become domiciled when there are environmental changes caused by human action and human migration in traditionally endemic areas and ecological imbalance resulting
Despite being a simple procedure, proper planning of the site of anastomosis, which should be in the preoperative and postoperative and setting the time for the beginning of the clip are fundamental to the success of the surgery (TOREGLANI, 2008).
the disorderly deforestation in the Amazon region (VP/PANAFTOSA-PAHO/who; 2009; p. 17; SESPA, 2009, p. 5).
The Triatominae have three life cycles according to the adaptation of the species to the environment: the wild cycle, the peridoméstico and household, these being the biological cycles that provide the transmission of Chagas disease (Miles et al.. 19..). Chagas disease can be transmitted by transfusion, congenital, vector, oral and accidental.
In symptomatic cases, the incubation period varies according to the form of transmission: vector (4 to 15 days); transfusion (30 to 40 days); congenital (without specific period) and oral (3 to 22 days).
Chagas disease has two phases: acute and chronic. The acute phase, which can be apparent or invisible, is the period in which they can detect parasites in the peripheral blood for direct examination, and the chronic phase is characterized by the lack or absence of parasites into the bloodstream. In children the acute phase is highly lethal and adults can develop into chronic or asymptomatic phase, which may be irreversible (FERNANDES, 2005, p. 26).
The initial clinical manifestations are similar to all frames, in which the infectious fever if accompanied of malaise, fatigue, anorexia and headaches, complicating the diagnosis (HINRICHSEN, 2006, p. 384). Other manifestations as adenopathy, hepato and splenomegaly, generalized edema, acute myocarditis and signs of meningoencephalitis, pericardial effusion, tachycardia, pallor, Dyspnea and abdominal pain can be detected in the acute phase of the disease (Pinto et al., 2008).
Are also important due to gravity, cardiac lesions, the Chagas ‘ heart disease due to its high mortality and the expansion of liners that affect mainly the digestive tract (megaesophagus, megacolon) (REY, 2008, p. 295).
When the specific treatment is not carried out in the acute phase, the spontaneous reduction occurs the parasitemia and evolution to chronic forms that can be indeterminate, cardiac, gastrointestinal, or associated form (cardiodigestiva) (BRAZIL, 2010, p. 144).
In the case of vector-borne transmission, there is occurrence of signal input port as the oftalmoganglionar complex (romaña sign) and cutaneoganglionar (inoculation chagoma) (CHOY 2005, p. 570).
Valente et al. (2011, p. 18) States that the increase of cases occurs by increasing rapprochement between the vectors, the reservoirs and the man due to deforestation and the migration of people to potentially endemic areas.
The knowledge about Chagas disease is necessary to health professionals, especially nurses who must identify early cases in basic health units, triage of acute and chronic cases and refer the patient to a doctor in order to receive the proper treatment. In this context the descriptive, retrospective epidemiological study and quantitative, identify the profile of the Chagasic patients served in the region.
METHODOLOGY
The descriptive epidemiology is intended to highlight the human features on the occurrence of the disease. The study of these features allows you to establish the correlation between the disease and certain personal attributes, such as: age, gender, occupation, marital status, socioeconomic status, and others; or the distribution in time and space (CAMPOS et. Al., 2000, P. 29).
TYPE OF STUDY
Second Parker (2007, p. 271) the descriptive study, aims to inform about the distribution of a population in quantitative terms and the population used in this type of study may be composed only of patients, can also be exclusively from healthy people.
The study is the epidemiological survey of existing data in charts, records of sampling form to characterize indexes, with views to the consolidation and analysis of existing data to evaluate the epidemiological behavior of a population (CAMPOS et. Al., 2000, P. 47).
This study is the epidemiological retrospective and descriptive type.
PLACE OF PERFORMANCE OF RESEARCH
The survey was conducted on Public Foundation Hospital de Clínicas Gaspar Vianna, reference in cardiology, psychiatry, and obstetrics, Nephrology ambulatory and hospital care of medium and high complexity, with support for teaching and research in the area of health, reference in Nephrology, cardiology and Obstetrics, in addition to the Diagnostic support service.
INSTRUMENT AND DATA COLLECTIONS
The objects of studies were open records in the public hospital in Bethlehem, from January 2012 to December 2012, provided by the medical files (SAME).
Based in Pereira (2007, p. 63) this survey stick to the variables concerning the people, place and time as follows:
- As for the person: gender, age, marital status, religion, income, occupation, education,
- On the spot: neighborhood, city and State of origin.
- About time: the month of service and further confirmation.
- Analysis of the data
The coefficients for each variable were expressed in percentage obtained by the formula: frequency of the variable is equal to the total number of data obtained about the total number of population times 100 constant (PARKER, 2007, p. 62).
For the statistical evaluation and graphical representation of the results was used the program Microsoft Office Excel 2007.
POPULATION AND SAMPLE
The aim of this work was the total population of patients with confirmed diagnosis for Chagas disease, enrolled and served in public hospital Cardiology reference in Belém/PA, from January 2012 to December 2012.
- Inclusion criteria
The present study had as a criterion for inclusion the charts legible, fair and complete patients over 18 years old, enrolled in the public hospital Cardiology reference in Belém/Pa, with the diagnosis of chagas disease from January 2012 to December 2012.
EXCLUSION CRITERIA
Were excluded from this research under the age of 18 years and medical records incomplete unreadable and unhealthy to people over 18 years, patients who were not registered in the public hospital Cardiology reference in Belém/PA, undiagnosed or dubious diagnosis of Chagas disease and outside the period stipulated in the criteria described above.
- Risk and benefit
This study presented direct risks to patients, as they displayed were not contacted and their identities remained secret. Also in the same proportion to the public hospital and for researchers, because it was held in restricted and safe environment of consultative form without the presence of unauthorized persons to the information of the patients. Conveniently, the benefits were low cost data analysis, with targeting important to public health in the State, with disclosure and clarity of the Chagasic patients para region.
- Ethical aspects
The research was based on Council resolution 196/96 national health service that “incorporates from the perspective of the individual and of the collectivities, the four basic principles of bioethics: autonomy, non-maleficence, beneficence and justice, among others, and aims to guarantee the rights and duties that relate to the scientific community, the subject of the search and the State” (BRAZIL, 2004, p. 1).
In compliance with the ethical aspects of this study, were suppressed any information that could identify patients and their medical records, as well as the assistance professionals and their conduct.
TERM OF INFORMED CONSENT (TFCC)
Because there was no interview or questionnaires to patients and not for professionals, there will be no assistance for this study the FICS. So was replaced by approval of this project by the Ethics Committee of the public hospital concerned.
RESULTS
Of the 163 records analyzed the SAME of Hospital de clínicas Gaspar Viana, seven were from patients diagnosed with carriers of Chagas disease.
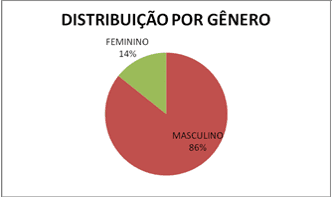
As the variable gender, the majority (86%) belonged to the male gender (Figure 4) and 14% of the female gender.
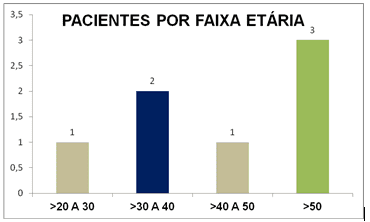
Already about the age group 20 to 30 had 14 >% patients, 29% were 30 to 40, 14 >% belong to the age group 40 to 50 and > above 50, being the highest rate at 43% (Figure 5).
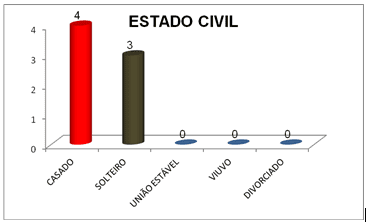
On the civil status, 57% of the patients are married and 43% are single, and the other as a widower, divorced and with stable did not show frequency (Figure 6).
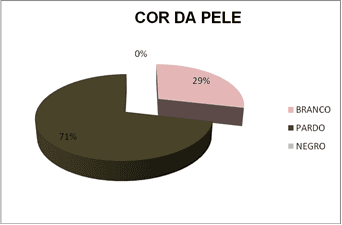
In the skin color stood out the color brown with 71%, and to a lesser extent with 29% declared to be white (Figure 7).
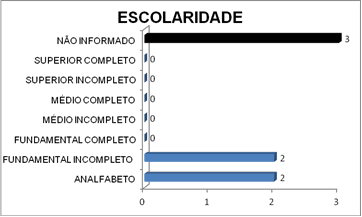
The figure below shows the level of schooling variable, where the prevalence of reported data with 43%, 29% belonged to the 28% incomplete basic illiterate and 0% for the middle and upper levels.
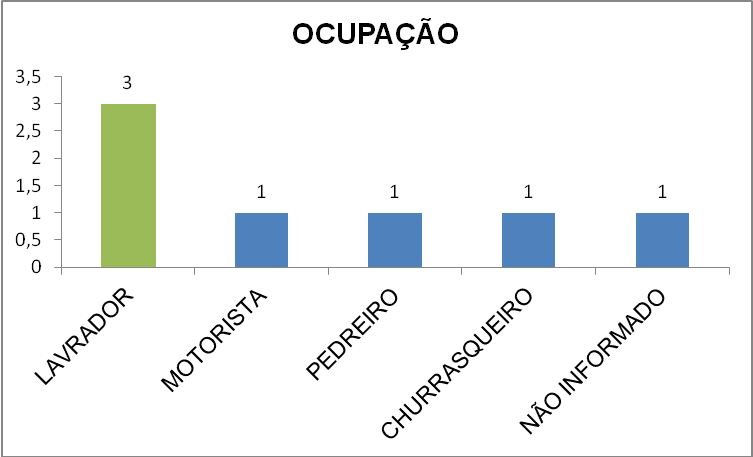
As the occupation 42.85% of the Chagasic patients were farmers followed the other professions of driver, bricklayer, barbecue with 14, 28%, and of those who were not informed 14.28% (Figure 9).
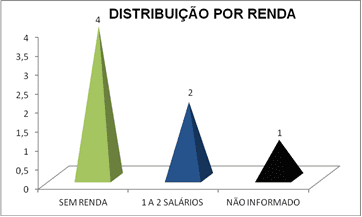
About of 57% do not have family income, 29% receive 1 to 2 salaries and 14% was not informed on the charts of patients (Figure 10).
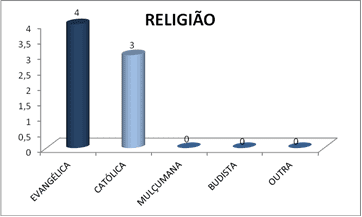
Slightly over half practice 57.14% Evangelical religion and 42.85% of this variable are Catholics and those who are Muslim, Buddhist religion and other religions mentioned in the chart there was no data between the patients seen at the hospital de clínicas Gaspar Viana (Figure 11).
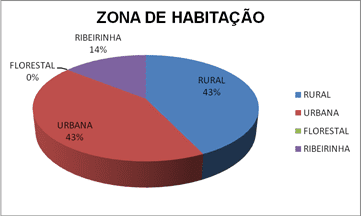
In the housing zone 57% are urban, less frequently the countryside with 43% followed riparian forest and not get any data. (Figure 12).
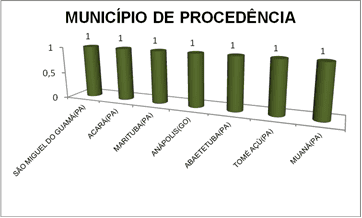
As for the city of origin of patients there was no repetition in the same municipality, 14.28% in the municipalities then occurring cited in (Figure 13)
DISCUSSION
In this work, we reported the epidemiological profile of the Chagasic patients attended at the hospital de clínicas Gaspar Vianna, enrolled in 2012, being made available 161 records with a diagnosis of congestive heart failure main and only two records with primary diagnosis of chagas disease, population seven confirmed patients with wounds.
However, the epidemiological investigation has become fragile on lack of medical records incomplete information in the service of medical file, causing the exclusion of epidemiological questionnaire items. The unavailability of information on patients referred to the hospital, met in the outpatient service concealed this work other possible records of patients with wounds.
The results regarding the genre of 86% of the males were possibly linked to poor hygiene in food preparation, since normally the activities in rural areas, on construction sites and road transits are activities that submit workers to minimum conditions of hygiene and bad eating habits.
The age range of the patients as demonstrated in Figure 2, shows no epidemiological significance to this variable, being the individual susceptible to any age over 18 years, pointing out that the study was limited to patients above this age.
As for marital status, there was no occurrence of widowed, divorced or stable Union, and individuals marrieds and singles were tied percentage, which suggests that there is no epidemiological significance to this variable, however, as individuals was of different locations means that the pathology was not being diagnosed on their spouses. It is possible that the infection occurred outside the familial environment, such as working environments.
The results related to skin color are consistent with the data from the IBGE census 2010, where the majority of the population of Pará (69.5%) declares itself and thus this epidemiological variable became unimportant[2].
The data found in charts of patients relating to income and education, showing the profile of the patients seen at the hospital de clínicas Gaspar Vianna in Belém, are poor patients, low educational level, consistent with the public who usually seeks the unified Health System. Despite this caution is needed when it’s safe to say that this is the profile of the Chagasic patients.
The more frequently the labour occupation of a farmer is related to housing, rural zone, where patients were inhabitants of these areas in accordance with Days (2007, p. 14) when it points out that the chagas disease has features rural and traditionally affects people of Central origin that inhabit or inhabited houses. However there was a higher frequency of patients from urban areas and significance due to the small sample.
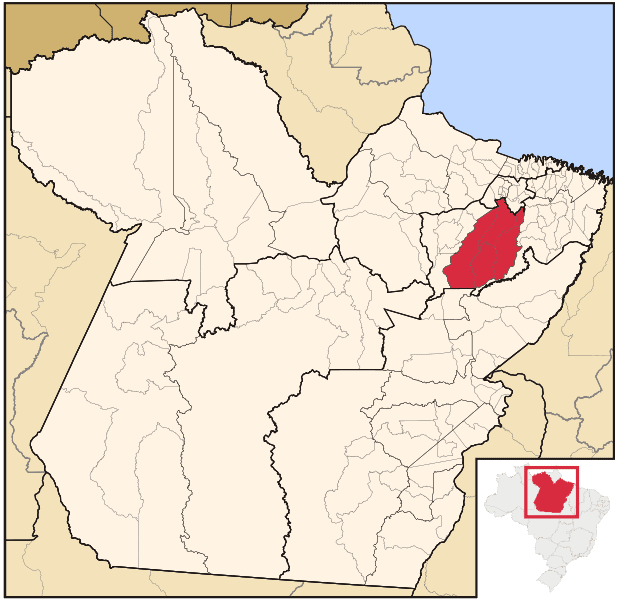
As to origin of patients there was no repetition (figura13), but the municipalities of Angel fish and Thomas Açú are part of the microregion of Tome Acu (Figure 14), making it the area of higher frequency. The municipalities of São Miguel do Guamá, Acará Açu, Thomas and Abaetetuba are part of Northeastern Pará Mesoregion, concentrating on this region as often, followed by Belém Metropolitan (United) and Brazil (Muaná) and one of the city of Annapolis.
CONCLUSIONS AND RECOMMENDATIONS
It is concluded that the profile of the Chagasic patients attended at Cardiology referral hospital in Bethlehem-PA in the year of 2012, men, age above 50 has years, married, color Brown, practice the Evangelical religion is farmer, has no income and is part of the microregion of Tome Acu. The variable ecolaridade was not informed on the forms. Being of fundamental importance to apesquisa.
As the hypothesis that in the region, socioeconomic characteristics interfere with the mode of transmission of the disease, yes one of the analyzed variables showed influences, since patients who seek the unified Health System usually are poor people.
It is worth mentioning that the sample size was small, making this work the basis for it to be expanded even on the private network to achieve a profile consistent with the region.
REFERENCES
ANDRADE J.A.. et al. Brazilian society of cardiology. Latin American guideline for diagnosis and treatment of Chagasic cardiology. ARQ Bras Cardiol 2011; 97 (2 Suppl. 3): 1-48.
BRAGA, Julius Cezar Vieira. et.al. Clinical and therapeutic aspects of heart failure by chagas disease. Brazilian Cardiology file. Volume 86, number 4, April 2006. Original article. Universidade Federal da Bahia-Salvador.
BRAZIL, National Health Council. Resolution nº. 196 of 10 October 1996. Brasília: 1996 available at: ˂ http://dtr2004.saude.gov.br/susdeaz/legislacao/arquivo/Resolucao 196 of October 10 1996.pdf ˃. Accessed on 23 October 2012. Time: 10:40
BRAZIL, M.S. EPIDEMIOLOGICAL ASPECTS/MS, 2012. Available at: ˂ http://portal.saude.gov.br/portal/saude/profissional/visualizar_texto.cfm?idtxt=31454 ˃. Access in: 14 July 2012. Time: 8:00 pm.
BRAZIL, Ministry of health. National Secretariat of health surveillance. System of notification of reportable diseases (SINAN). Practical manual of Notifiable aid in SINAN. Base text of John Carlos. 2004. Available at: ˂ http://portal.saude.gov.br/portal/arquivos/pdf/manual_chagas.pdf ˃. Accessed on 23 September 2012. Time: 11:45
Brazil. National Health Foundation. Guide to epidemiological surveillance. 5. Ed. Brasilia: FUNASA, 2002.842 p.
Brazil. Guide to epidemiological surveillance. Ministry of health. Health surveillance Secretariat: Department of epidemiological surveillance. Brasília-DF. 2009.
Brazil. Investigation of two outbreaks of acute Chagas disease in the region of the islands of Marajó, Pará State, Brazil, in 2007. Electronic Epidemiological Bulletin. Health surveillance Secretariat. Year 08 n° 04, June 2008. Available at: ˂ http://portal.saude.gov.br/portal/arquivos/pdf/ano08_n04_surtos_dchagas_aguda_pa.pdf ˃ accessed on: 13 June 2012. Time: 5:10 pm
Brazil. Ministry of health. Health surveillance Secretariat. Department of epidemiological surveillance. Infectious and parasitic diseases: Pocket Guide. 8 ed. Rev.-Brasília, 2010. 448p. (number of basic texts).
Fields, Juarez de Queiroz. et.al. Environment and epidemiology. São Paulo: editora ADEKUNLE, 2000.
CHOY, J.R. dynamics of infectious and parasitic diseases. Rio de Janeiro, Guanabara Koogan, 2005. p. 569.
CHOY, J.R. et al. Laboratory of parasitic diseases, Oswaldo Cruz Institute – Fiocruz Av. Brazil, 4365 – Rio de Janeiro – RJ-21040-360. Available at: ˂ www.paho.org/cdmedia/manualchagas2012/pdf/modulo1.pdf ˃ accessed on: 12 July 2012. Time: 4:00 pm.
FERNANDES, R.M. The evolution in knowledge and control of Chagas disease in Brazil: a case study on the interaction between science, technology, health and the economy. 133f. Dissertation (master in Economics)-Faculty of economic sciences of the Federal University of Minas Gerais, 2005.
Guide to surveillance, prevention, control and clinical management of acute Chagas disease transmitted by food. -Rio de Janeiro: VP/PANAFTOSA-PAHO/who, 2009. 92 p.: il. (Series of technical manuals, 12).
GUIMARÃES, HÉLOÏSE. Symposium on chagas disease. Speech given at the Hospital de Clínicas Gaspar Viana, para-Belém, 21 August 2012. Available at: ˂ http://www.gasparvianna.pa.gov.br/? q = node/˃ 301. Accessed: 26 August 2012. Time: 7:00 pm.
HINRICHSEN, s. infectious and parasitic diseases. Rio de Janeiro, 2006.
Lion, Raimundo Nonato de Queiroz of-Bethlehem: UEPA: Instituto Evandro Chagas, 1997.886 p.
MAIA, T.O.D. et al. Seroprevalence of American trypanosomiasis in adults in anarea of the western Brazilian Amazon region. Journal of the Brazilian Society of Tropical Medicine 40 (4): 436-442, jul-Aug, 2007.
MATHIAS, R.G. et al. Parasitology & human mycology. 5th ed. Rio de Janeiro: Guanabara Koogan, Medical Culture: 2008.
NEVES, D.P. Parasitology. 3 ed. São Paulo, Atheneu, 2009.
VP/PANAFTOSA-PAHO/WHO. Guide to surveillance, prevention, control and clinical management of acute Chagas disease transmitted by food. – Rio de Janeiro, 2009. 92 p.: il. (Series of technical manuals, 12).
PEREIRA, M.G. Epidemiology theory and practice. Rio de Janeiro. Guanabara Koogan. 11th reprint: 2007.
PATHAK, Ana Yecê. et al. Acute phase of Chagas Disease. Study of 233 cases of Pará, Amapá and Maranhão observed between 1988 and 2005. Journal of the Brazilian Society of Tropical Medicine. 41 (6): 602-614, nov-Dec, 2008
REY, l. Parasitology: parasites and parasitic disease in the tropics. 4 ed. Rio de Janeiro: Ganabara Koogan, 2008.
REZENDE, j.m. Clinic: digestive Manifestations. In BRENNER, Z.; ADNAN z. a. Trypanossoma cruzi and Chagas disease. Rio de Janeiro: Guanabara Koogan, 1979-.
SECRETARY of STATE for public health (SESPA), available at: ˂ http://www.saude.pa.gov.br/index 2012. PHP/news/197-Symposium-alert-for-further coronary heart disease-associated-to-evil–of-wounds ˃. Access in: 06 September 2012. Time: 3:30 pm
SESPA. Stock Manual of surveillance and control of chagas disease for community health agents and agents of endemic diseases in the State of Pará. Belém-Pará, 26 p, 2009.
SESPA. Quick reference guide for health professionals. Acute chagas disease-epidemiological aspects, diagnosis and treatment. Government of the State of Pará, Secretary of State for public health, 2007.
SILVA & T, Tiago Person. Elimination of transmission of Chagas disease by Triatoma infestans in Brazil: a historical fact, Journal of the Brazilian Society of Tropical Medicine 39 (5): 507-509 Sept-Oct, 2006.
Brave, V.C. genotypic Study of Trypanosoma cruzi: epidemiology and molecular characterization of isolates, Triatominae and wild mammals of Pará, Amapá and Maranhão. 164f. (Doctoral thesis in biology of infectious agents and Parasitological)-Institute for Biological Sciences of the Federal University of Pará, 2011.
VERONESI, R.F. Treaty of infectious diseases. 3 ed. São Paulo. Publisher Atheneu, 2005.
VERONESI, R.F. Treaty of infectious diseases. 4 ed. São Paulo. Publisher Atheneu, 2009.
www.propaz.pa.gov.br/quem-we are, access date accessed: 18 June 2012. Time: 9:30
[1] Paper presented to the Graduate Center (CPO ´ ‘s) of the Amazon (ESAMAZ). Lato Sensu graduate studies in nursing in Nephrology and Urology/Nurse.
[2] Program of the Government of the State of Pará, created in 2004, in the first mandate of Governor Simão Jatene, aiming to articulate, promote and align public policies focused on childhood, adolescence and youth, in order to guarantee human rights, the fight and the prevention of violence and the spread of a culture of peace. The actions happen in partnership with different sectors of society, Government and non-governmental organizations. www.propaz.pa.gov.br/quem-we are
[3] http://www.brasil.gov.br/noticias/arquivos/2012/07/02/censo-2010-shows-the-differences-between-general characteristics of the population-brazilian















