FARIAS, Naiara [1]
FARIAS, Naiara. Obstetric violence: Integrative Review About abusive practices in health institutions. Multidisciplinary Core scientific journal of knowledge. 03 year, Ed. 06, vol. 03, pp. 136-157, June 2018. ISSN:2448-0959
Summary
Every woman has the right to a prenatal with quality to target the mother's health and especially the baby, having as main need an escort you to your preference that will be at your side throughout the duration of the period of confinement, in addition to all the woman should r treated with dignity where their physical and psychological integrity were to be guaranteed. Institutional violence has become a public health problem in recent years, as occurs in all gravid-puerperal cycle during the attendance of these pregnant women in health institutions. Following this sense the present work will conduct an analysis of the main points that lead these women suffer this kind of violence committed by professionals in the field, this is an exploratory study with a qualitative approach of deal with the problem presented in the course of the work.
Keywords: Obstetric Violence, Institutional Violence, natural childbirth, child abuse, Wife, humanization.
1. Introduction
This paper will discuss with ownership over the problems that drive certain acts of cruelty to women, who from the moment you discover pregnant women preparing for the long-awaited hour is the arrival of your baby, but throughout this process these women are faced with many questions, tribulations, fear, joy and emotions. So many times this dream now becomes a situation of suffering, embarrassment, pain and even torture.
The work is justified by the subject addressed as troubling matter and of paramount importance on individual and collective awareness of health professionals especially for those who suffer violence obstetric, that issue has become a practice quite common in health institutions. Women affected by acts of violence obstetric fear for maltreatment in your moment of weakness, by not being aware of the physiological process of childbirth, cultural issues, low income, illiteracy among countless factors that also influence in this understanding. Much has been talked about violence against women, domestic violence, sexual, verbal, among others that is applicable to judicial penalty, even more so the obstetric violence issue has become a theme still uncertain for these victims.
The theme addresses as main subject the abuse these women suffer for being in a moment so delicate as pregnancy, although the term violence is discussed in obstetric brazilian society your experience within the institutions Hospital and very common, but little is reported by victims, leaving a traumatic experience, difficult to handle in the course of life.
It is understood that there is a problem around the violence that occurred in health institutions. On the above, this study is based, the following question: what about abusive practices analysis of obstetric violence within health institutions? In the course of work we will perform a search of which acts are applicants during delivery of these women, and how it feels to go through this situation, using as main instrument of information not only for those victims as well as to all society.
The general objective proposed a presentation regarding the abusive practices of obstetric violence within health institutions committed by professionals in the field, through a bibliographical review to extremely academic. While specific objectives have priority; analyze the factors that are associated with obstetric violence, abusive conduct present performed by health professionals evaluate how the humanization can influence the process of childbirth.
For many years these practices related to pre-childbirth, postpartum and childbirth are being carried out in these women, today a great discussion that revolves around these situations to find out the need of these procedures are performed almost routinely by professionals in the field. These professionals need to be aware that these practices which abuse the body of these women injure the personal integrity, freedom, honor and dignity of those mothers. In the course of the project the aim is to discuss how the existence or not of violence and understanding these women about it, for elimination of this practice.
According to approach the problem, this research is an exploratory study with a qualitative approach held from bibliographical revisions through secondary sources in order to target the knowledge of the given theme, were researched articles in database-Scientific Electronic Library Online (Scielo), Virtual Health Library (VHL), electronic journal of Information communication and innovation in health (RECIIS). The items entered as inclusion criteria were all original articles related to the theme proposed between the period of 2005 to 2017, exclusion criteria was thrown any article that didn't treat the subject directly.
2. Factors related to obstetric violence
The care offered to the woman during the birth process has suffered many modifications through time, consequent of the medicalization of childbirth, and institutionalization of technological advances and the development of medicine. In the past, childbirth was assisted by women in home environment, by midwives, who were pregnant or confidence of recognized experience in the city, which had some wondering about the physiological mechanisms of delivery.
However, in the twentieth century in the 40, has intensified the hospitalization, which allowed the medicalization and childbirth, pregnancy period control and birth as a natural process, and private, family started to be experienced in the public sphere, in health institutions with the presence of several leading actors this time. (MC; et al 2016)
However due to those facts mentioned above the woman became an object of study since the institutionalization of childbirth away these women not only from the comfort of your there, but also left them more susceptible to suffer some sort of aggression, leading to a little theme known, but who comes won space over the years.
Violence against women in health institutions, refers to any act related to the psychological, physical and moral suffering, soon and can be characterized as any cruel act committed by health professionals using interventions without need, accelerating the biological processes of a normal birth (ADHIKARI; AGGIO, 2014).
This term corresponds to the birth abuse, institutional violence, cruelty in childbirth, desumanizada assistance among others, which are used to describe the various forms of violence that occurred in puerperal assistance. (DINIZ; et al., 2015).
However in the second decade of the 21st century, the obstetric violence wins visibility through reports, documentaries, all this through testimonials from women who are victims of that era, becoming a public health problem with joint interventions confirmed by the World Health Organization (who), entitled "prevention and elimination of abuse, disrespect and mistreatment during childbirth in health institutions". (DINIZ; et al., 2015, p. 1).
Parses that despite being considered a new theme has a very important impact in changing care practices in the gravid-puerperal cycle.
However, the period of 1980 in Brazil this subject was approached by feminists of the time who used experiences of victims showing explicit as was experienced births that occur in health institutions, the mirror of Venus was the pioneer because was a descriptive study of these experiences. (DINIZ; et al., 2015)
(…). It's not just in sexual intercourse that violence appears marking women's existential trajectory. Also in the medical patient relationship, once the ignorance of your physiology is raised to explain the feelings of helplessness and disappointment with his wife watching your body be manipulated when refers to the medicine in the most significant moments your life: birth control, childbirth, abortion. (DINIZ; et al., 2015, p. 2)
Institutional violence is embedded in everyday hospital work, defined under two aspects one of omission and Commission. The first relates to neglect customer service regarding women seeking the unified health system (SUS) no longer met their needs of that moment, and the Commission is unnecessary or even undesirable procedures , including insults and threats. (Saints; Smith, 2010)
Among various situations of violence related to women during childbirth is characterized by the negligence of the professionals that make, using technologies such as unnecessary procedures on gravid and puerperal cycle and there is no the victim's consent wounding so their rights.
Surveys conducted in several States in Brazil showed extreme authority of professionals under the body of his wife during childbirth, being one of the most frequent complaints among those who have recently given birth. (ADHIKARI; et al 2016)
A factor that is still pointing as utmost importance, are patients who live in disadvantaged socioeconomic situations these are the biggest victims of oxytocin, immobilization in bed, litotômica position in childbirth, and the famous episiotomy, especially if they are black in disadvantaged economic situation, and even foreign Northeastern.
We cannot deny that advances in technology are bringing quality obstetric assistance, however much has observed that the exploitation comes bringing with it the medicalization, thus making the labor as a problem, where medical intervention becomes essential to have a healthy birth. (CASTRO; CAPLIS, 2005).
The humanization of childbirth is linked to reduction of Cesarean sections on improving customer service, so that it can be rescued a birth of most natural way possible.
But this goal can only be achieved after the desmedicalização of assistance, and of course with the changes of posture of these professionals face the needs of women who need a decent service. (CASTRO; CAPLIS .2005)
The institution also has to understand that it is not doing labor anesthesia in all patients who humanizes; and not decreasing the number of cesárias with the increase of forceps; much less only preaching breastfeeding has that unique; and Yes educational restructuring in the pros; upon scientific basis. (CASTRO; et al., 2005. p. 966)
Nursing is linked directly with the humanization, would contribute what they have autonomy, but the birth Centre is more complicated because there are many barriers that prevent the humanization is implemented with these women, among them are the own doctors to rule out a more natural therapy, putting above all a science based on mechanical and chemical procedures.
The interventionists are of an alleged security, so that many doctors, if they consider it scientific knowledge holders sometimes deem unnecessary to provide the woman information on pregnancy, as well as to receive the consent the same.
2.1 the pilgrimage of pregnant women in the gravid-puerperal cycle
A considerable factor as institutional or obstetric violence is women's demand for a hospital that embrace at the time of the birth of your baby, this important fact is connected to precariousness of care in public health.
In Brazil on 27 December 2007, 11,634 law guarantees the right of pregnant women to knowledge and linking to the maternity ward where you will receive the necessary assistance to have your baby, however, the precariousness of the assistance to these women along with inequality related to obstetric beds unavailable, it is evidenced the lack of investment in public health in the country. (RAO et al., 2015)
The journey that these women experience from the moment you see without the need to feel protected, may be contributing to future problems related to them, and also to its concepts, bringing serious risk of life, for not they get care in a timely manner, causing maternal mortality infant rates been increasing every year.
Here are some statements concerning:
Just when I was starting the aches, pains and increasing went to the hospital and treated me and then I went to another, in another city, and I have attended and I came to this motherhood.
I was told to look for another maternity and had no place for hospitalization (…) was a lack of respect for me, I'd have to meet and have a spot and look for another hospital (…) it was a chaos (…). And I never want to go through that situation, I couldn't spot for lack of bed. (RAO; et al, 2015. p. 616)
It is observed according to the above reports, that some factors were instrumental in occurrence of not meeting these women, first reported this referring to the structural conditions of the health units that are not prepared to receive these women, and the second refers to the distance a unit with beds available for specialized care, undermining thus the birth of these babies.
The lack of respect, refusal of care is embedded in the everyday life of some professionals, contributing to a reality in obstetric assistance, as disrespect, abuse that can be observed in these pregnant women during your search process by attendance.
The height of absurdity was the doctor speaking rude to me, giving me a Scolding for this situation, and at the end I think I got out as guilty, but then I got out of there and went with a friend to another hospital because there wouldn't be any attention from anyone. A contempt. (PS36) And I started to complain and the nurse began to repress me and insult me, saying I had to do this before, and how would I do that? A rude, disrespectful to me and on behalf of my weakness, I felt guilty at the time, more then I thought they were wrong, not me. (PS39) (RAO; et al, 2015. p. 618)
These professionals must pass through a reflection of his attitude, because the host of those women not set an unacceptable conduct on the code of ethics of each professional.
After all, the journey these women looking for beds in health institutions in Brazil became an obstacle characteristic of poor care during the prenatal period to these pregnant women, since, as law No. 11,634, December 27 2007, has that is straight from the woman have as main information which motherhood will receive assistance in the parturitivo process, avoiding the pilgrimage in prepartum and postpartum, avoiding therefore complications for both.
3. Conduct that represses women in childbirth
Health professionals in particular doctors and nurses as the whole team are responsible for a dignified assistance to their patients, who often describe themselves in situations where women are used as objects of study for medical residents to perform an episiotomy with academic purposes without the consent of the victim, so your body. (DINIZ, SALGADO et al., 2015)
According to Diniz, salty et al. Studies show that women selected for these types of procedures with improvement in the technique of episiotomy, forceps and cesárias, depends a lot on your social level, noting that the bigger the woman is vulnerable more humiliating is the treatment offered to her. What makes something regrettable to see these women have their dignities disrespected by the mere fact of being helpless at that point or simply victims of your own ignorance.
So women whose pregnancies without complications end up being neglected by being subjected to unnecessary and harmful intervention causing more damage than benefits the health of the mother and the baby, demanding a string of Cesarean sections, featuring a birth pathological that needs to be treated and changed to a new model of assistance. (SANTOS, LEO et al., 2017).
As for procedures performed on women in puerperium realizes that in the vast majority of your hurt women's rights, such as the determination of position, Kristeller maneuvers, episiotomy, husband, ocitócicos administration as the accelerator Labor, interventions with didactic purpose, valsava maneuver, birthing position constraint, restriction of feeding and hydration, all these assigns decision-making power to health-care professionals, in addition to constituting a form of physical violence mother and baby.
In the year 2002, more than 38,000 newborns and 2000 women have died in the country by gravid-puerperal cycle complications and as a result of abortions. In this sense, there are over 500,000 maternal deaths in the world, more than 50 million women suffer from diseases or sequelae related to pregnancy, and at least 1.2 million newborns die from complications during pregnancy and puerperal cycle. The hegemony of knowledge of medical science, about the woman should based on recent results, acquired from studies carried out in the area, supported by scientific evidence, be questioned, so that there is a reformulation in order to deal with the physiological process of childbirth. (MC; 2007, p. 453).
Unnecessary interventions which are responsible for the largest number of infections, which result in further complications that require medical intervention. (MC; et al., 2007)
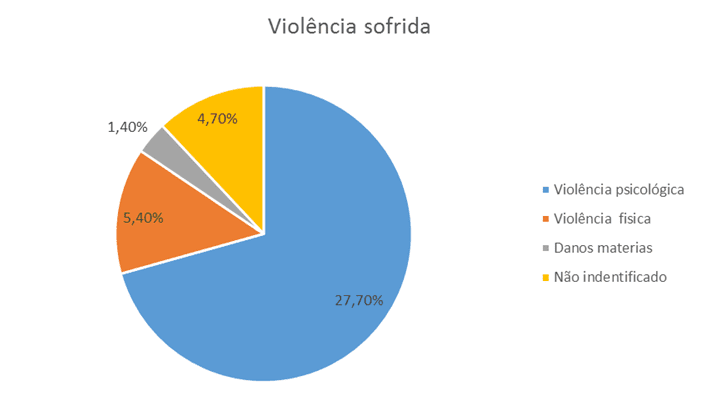
Follow the chart that shows the violence suffered by women (%)
Taking into account the evidence cited above, cannot be allowed to use the ruler medical wisdom known risk factors, that would be the concern for the safety of your concept and who has recently given birth, as a way of justifying the medicalization of natural process of birth, disregard any possibility inconsistent.
3.1 Distinguishing obstetric violence
Obstetric violence is not an easy thing to be recognized first by that most women don't even know that exists, second because most of the pipes are in many ways, with different characteristics, and many times these women come to think and consider normal and routine attitudes of these professionals to be expected by them. These acts that affect the body of these women, causing pain and even physical injury (from mild to intense degree), without scientific basis, features physical violence. The verbal and behavioural conduct that develop in these women feelings of weakness and helplessness, are psychological.
When the conduct of these professionals are conducted to infringe the privacy or your physical integrity, to touch the private parts, will be set up the sexual nature of this violence. However, as the Organization of the institution is so difficult or even go so far as to prevent the access of recent mothers to their legally guaranteed rights, will be setting up institutional violence.
The following is a fact-based reporting:
"The episiotomy is the most commonly performed obstetrical operation in the West. Is one of the most dramatic and intense ways in which the territory of women's body is suitable, the only operation performed on the body of a healthy woman without your consent. It represents the power of Obstetrics: babies cannot get out without women to be cut. She avoids that women experience childbirth as sexual event, and is a form of ritual genital mutilation "(DINIZ; 2001. p 42)
In a survey titled "Born in Brazil: national survey on Childbirth and Birth" in which it was found that women who are serviced in the SUS (unified Health System) are more helpless and vulnerais increasing the chance of suffering violence, obstetric but we can't say that those who are served by private network are free from being victims of violence. (FAUSTINO; et al 2016).
What happens is that in private hospitals these pregnant women don't even get to go into labor, they have their scheduled surgeries following straight to the operating room, where they are subjected to unnecessary elective cesarean section. Some myths in pregnancy stimulates these women to take a decision on the question of choice of childbirth, many of them already come with the decision, others are influenced by the professional staff accompanying them during the prenatal period, making the decisive guidelines for choice, as a false indication of Cesarean section, lack of dilation, narrow basin, dry delivery, delivery time consuming, has no expansion among other information passed the these pregnant women.
Was published in 2016 National Health Agency (NSA) data on births that occur in Brazil, so that we can conclude that 569,118 were performed in accredited network deliveries, all Parents, and 481,571 were cesarean sections corresponding 84.6% of the births that occurred through covenants doctors, were c-sections, i.e. Comparing the previous year 2014 there was a fall of 1% in cesárias rate made by health plans. (FAUSTINO; et al 2016)
It is worth mentioning that a debate on the society in order to clarify any doubt aware women, about the abusive procedures, that are usually pointed to as natural or normal on the understanding of these women, who in most times do not have the notion of being victims of violence obstetric, because the institutional or circumstances involving pregnancy leave the woman vulnerable to receipt of these procedures
3.1.1 protection mechanism to the victim of violence obstetric
All recent mothers have the right to receive the necessary information about your health and the baby too, about the above procedures and carried out, in clear and precise language so respectful and understandable where the same can understand what's going on in your current situation.
The multidisciplinary team has a duty to explain the purpose of each intervention or treatment, as well as the risks or potential complications to the mother or your baby may have during your hospital stay, as well as the alternatives available to help her. Yes, will be based on information passed to her, that these women will have the right to refuse the treatments or procedures in your body.
According to research conducted in 2010 1 between four women suffer from violence during childbirth, among them are patients in disadvantaged economic situation that are served by public hospitals, Northeastern, with HIV, prostitutes, users of drugs, single women, adolescent girls, black girls, among other foreign. Such violence and disrespect were proven through test called "Obstetric Violence test" where they were answered by more than 2000 women in 2012. (SILVA et al., 2014).
Based on information taken from the Department of health launches the humanization in the prenatal program in order to ensure women's rights in your pregnancy and puerperal cycle. According to the who women must have their births without any type of induction, the event should occur spontaneously without any mechanical or chemical intervention, giving full freedom to woman to move freely, to express their emotions without any repression or disrespectful. (ADHIKARI; et al 2016).
Besides, all these rights are guaranteed by Human Rights:
Practice the disrespect and abuse during the pré‐natal and childbirth are violations of the basic human rights of women. All these rights are based on internationally established human rights instruments, including the Universal Declaration of human rights; Universal Declaration on Bioethics and Human Rights; International Covenant on economic, social and cultural rights; International Covenant on Civil and Political Rights; Convention on the Elimination of all forms of discrimination against women; Declaration on the Elimination of violence against women; Report of the United Nations High Commissioner for human rights regarding the prevention of Maternal morbidity and mortality and Human Rights; Declaration and Platform for Action of the Fourth World Conference on women, Beijing, 1994. (SILVA et al., 2014. p. 721).
Thus the woman is supported in every way, it's up to her to seek their rights when they feel themselves wronged somehow. Assists in maternity wards are defined by women as good or bad support and related actions, the presence or absence of professionals in most of the time and also the communication that often restricted in few words, becoming one of the the most significant factors for both patients and for their families. (AB; OLIVEIRA, 2011)
According to the law of 8,080 1990 constitutes the single health system that brings the principle of universality and compliance, highlighting a important annex of 11,108/2005 law, ensuring the right of women to date of your choice, during labour, childbirth and postpartum. (SHAH; et al., 2016)
In this sense, was edited to Ordinance No. 2,418/2005 of the Ministry of health:
Art. 1 Regulate in accordance with art. 1 of law No. 11,108, of 7 April 2005, the presence of an escort for women in labor, birth and immediate postpartum in public hospitals and affiliated with the Sistema Único de Saúde – SUS. (SHAH; BRAVE, 2016, p 03)
So it's not up to hospitals, perform an interpretation of the law, but, just run it. Since the norm is explicit in the sense that the woman has the right to date in the labor, i.e., the date can and should watch any kind of labor, because the law doesn't make any kind of specification, but the problem continues, do not supervision and even punishment for those who insist on I broke it.
4. The importance of humanizing at birth
The humanization of childbirth carries mainly professional performance for human physiology, i.e. not intervened without the normal process of parturient, recognizing how members and cultural aspects of childbirth and birth, promoting health, emotional support to mother and baby, facilitating links between them.
The term humanize, is being used, in childbirth assistance for many years, and their broadcast concepts in obstetrics medical authorities in the international arena, in order to retrieve the birth family and natural event and join the benefits of modern scientific evidence. (DINIZ .2005)
The who (World Health Organization) decided to propose in its guidelines that the purpose of the assistance is to achieve the main objective of a mother and a baby more healthy with the least possible intervention that interfere in the safety of both, thereby reducing the neonatal mortality rate.
On Humanized assistance, avoid unnecessary procedures and are only carried out interventions whose effectiveness and safety have been demonstrated by scientific studies well conducted, following the principles of what we usually call " Evidence-based medicine ". Outdated practices such as fasting, Trichotomy (by scraping) and enteroclysis (enema) should not be adopted. You must enable and encourage the woman to take the position that you want during labour. The presence of the escort should be stimulated, 8 that women feel safer and more comfortable when accompanied by someone of your family or your group of friends. The presence of a chaperone results in less pain for the mother and reduces unnecessary interventions. Stimulate the non-supine positions for labor and childbirth should be avoided in the conventional position lithotomy position (popularly known as "roast chicken"). Non-pharmacological methods are used for relief of pain and analgesia is performed in selected cases, if the mother request. Avoid the routine episiotomy, that is, the cut in the perineum that theoretically believed to facilitate the departure of the baby, but nowadays if you know that it is not necessary for routine and can be harmful. Immediately after the birth the baby must be placed in the arms of his mother, heated and dried in your lap, stimulating yourself breastfeeding in the first half hour of life. But at all times should consider the characteristics and expectations of that mother. (CHANDLER, 2016, p 07)
It is essential to report that the humanization of childbirth assistance, recognizing the social and cultural aspects of childbirth and birth, offering emotional support to women and all your family. Other aspects relating to women's freedom during the whole process of giving birth, with the preparation of a plan of childbirth that is respected by health care professionals to assist it; to have an escort of your choice; to be informed about all procedures shall be submitted; and to have their citizenship rights respected.
The humanized childbirth has a broad range of interpretation so that it can be understood as that which is accomplished with less medical and pharmacological interventions possible, respecting the physical and psychological time of each pregnant woman, always occurring in a place respectful and warm keeping your privacy, being informed of all the procedures that can be performed in your body. (LAMB, 2011)
So, briefly, inside of this ideology seeks to:
Show the risks to the health of mothers and babies obstetric practices inappropriately interventionist, rescue the birth as existential and socio-critical event with deep and wide personal repercussions, revalue the birth, humanizing the postures and conduct in the face of labor and birth, and encourage women to increase your autonomy and decision-making power over their bodies and their deliveries and combine technical and scientific knowledge systematized and proved the humanized assistance practices Labor and birth. (LAMB, 2011, p. 21)
Still continuing to what was quoted above, the humanization of childbirth in modern days, formula that all initiatives have criticized the fact that Brazil be the world record holder of Cesarean sections, became the "normal mode of birth" or "typical" national delivery pointing to the results of this situation both for women and for children. (LAMB, 2011)
Humanize childbirth is to give rights to women's choices, providing a service targeted to their needs, where this same woman come have more autonomy over their choices, who will be at your side at time of delivery, in which institution the hospital is childbirth and even what is the professional who will attend the birth, something that doesn't happen with women met in public networks, in this type of delivery the presence of an escort and the pregnant woman has as guidelines change over positions, or to choose the most suitable position for the expulsive period, thus facilitating the birth of a fetus.
4.1 the importance of emotional support at birth-doulas
As well as the companion has paramount importance in time of childbirth for women where she has greater satisfaction in time to give birth, currently can enlist the aid of specialized professionals also called doulas, these women harmonize a affective and emotional support, and integrates the social support network, these professionals are trained with the assistance procedures and monitoring, offering emotional support and physical and affective support before, during and after childbirth. (SILVA, 2011).
According to Silva (2011); We can say that compete the doulas the following functions:
Before delivery:
- Clarify and inform about the formation and development of the baby and the pregnant body (amendments)-the reflection of these changes relative to the companion and adaptation in daily life;
- Delete some sort of pain that the new attitude can bring;
- Awakening in pregnant better awareness of the body through body language techniques;
- Perform massage sessions and relaxation, reflection, seeking a unique moment, silent and pleasurable with your baby; 75
- Teach breathing techniques to control pain, stretching exercises and strengthening for the lower back, legs, muscles of the pelvic region, preparing the body for childbirth;
- Addressing topics such as: what is pain, contractions, positions, statements and other pregnant women about their experiences and feelings experienced;
- Guide in decisions of the couple about the choices in relation to time, type and location of birth, showing its advantages and disadvantages, allowing the couple a conscious choice and responsible;
- Explain medical terms, hospital procedures and possible interventions.
During childbirth:
- Assist the mother about the most comfortable positions for labour and delivery, help with breathing techniques and measures to ease the pain, such as hot showers, relaxing massage between contractions, among other procedures that assist and facilitate the birth of a baby;
- Protection the woman that she has your desires, your privacy and your rights;
- Follow the mother since the beginning of labor, decreasing the tension caused by hospitals and by the presence of many unknown at time of delivery;
- In the immediate post-partum stay with the mother, in order to guide the first feeding.
Postpartum (Puerperium):
- Offer support in relation to breastfeeding and baby care, bath, change diapers, nutrition of the mother because of breastfeeding;
- Postpartum exercises, aimed at the recovery of the pelvic floor; 76
- Promote massage technique in infants – "Shantala" –, and teach her parents (in order to increase the intimacy of the parents with the child). (SILVA, 2011, p 74)
Yet we say that doulas comes to assist women who have the desire for a normal and natural childbirth without medical intervention, always looking for is next to pregnant women, to facilitate the labor, through techniques, providing a quiet moment and only for the mother, experiencing the time of delivery so sensitive, always reducing the tension and nervousness of the pregnant woman, giving chance to mate with a moment so special and unique. This proximity of doulas brings the security of these women, mainly psychological, because the trust establishes a bond where the mother feel comfortable expressing their emotions.
4.1.1 guidelines that contribute to the humanization of natural childbirth
The precariousness of mother and child health care in the country, the program of humanization of the unified Health System, for the prenatal and Birth, can be an important milestone, despite the difficulties encountered in your implementation.
In the late 20th century, increases in worldwide a movement that offers service that is based on evidence of experiences for women, advocacy and efficiency of procedures in all medical specialties. In the case of pregnancy and childbirth care, this concern is all the more essential since, unlike other specialties, these practices will interfere on women and children supposedly healthy, and a supposedly normal delivery process. (DINIZ, 2001)
The World Health Organization (who, 1997) developed a classification of common practices in the conduct of normal childbirth, driving for what should and what should not be done in the process of childbirth. This classification was based on scientific evidence concluded through research done around the world. Let's see: (SILVA .2011)
The) conduct that are clearly useful and should be encouraged:
1. delivery plan should determine where and by whom the delivery will be carried out and should be elaborated during pregnancy by the wife and husband/partner.
2. The risk factors of pregnancy should be evaluated along the same and should be re-evaluated until the time of delivery.
3. The physical and emotional well-being of women throughout the labour and delivery should be monitored.
4. liquid should be provided orally to the woman during labor and delivery.
5. all information must be provided about the possible choices of local labour and must respect the final decision taken by the woman.
6. obstetric assistance shall be provided on the periphery of the site of delivery chosen (…)
B) Conducts clearly harmful or ineffective and should be deleted:
1. Routine feature the enema/colonic.
2. Routine feature the Trichotomy (scraping of pubic hair).
3. Routine intravenous infusion in labor.
4. Routine prophylactic intravenous cannula insertion.
5. Routine use of the supine position (lying down) during labour.
6. Rectal exam.
7. Use of x-ray pelvimetry (measurement of diameter of pelvis/pelvis).
8. Administration of pitocin at any time before delivery, so that your purpose can be controlled.
9. Routine use of the lithotomy position with or without Stirrups during labour and delivery.
10. Excessive efforts of expulsion during delivery (…)
C) Ducts used with insufficient evidence to support your clear recommendation and should be used with caution until the completion of further studies:
1. not pharmacological Method of pain relief during labour, such as the use of herbs, immersion in water and nervous stimulation.
2. routine Feature the amniotomy to rupture it (surgical disruption of fetal membranes = "bag of waters") during the beginning of labor.
3. pressure on the bottom of the uterus during labor and delivery.
4. protection-related Maneuvers of the perineum and the cephalic pole at time of delivery.
5. active Manipulation of the fetus at the time of birth.
6. Use of oxytocin, controlled cord traction or combination of both during uterine emptying (…)
D) Pipes often used inappropriately:
1. Restricting food and fluids during labour.
2. Pain management for systemic agents.
3. Pain control through anesthesia epidural.
4. Electronic monitoring of the fetus. (…) (SILVA .2011, p77 seats)
The above program introduces policies of autonomy and recognition of human rights, based on the guidelines of the World Health Organization (who). Therefore, the transformations are resistors, practices being sustained assistance it keeps and deletes, the idea that contradicts the ethics that should support it.
So it was observed that some of these practices that were adopted in the model of attention, such as in the case of a woman's choice date, already in Group B are more common in maternity wards as for example the scraping by, washing and fasting, and in Group D, the high Cesarean rate and episiotomy. Soon we can say that, prevent deaths considered preventable and maternal health is one of the main national interest amounts in relation to the guarantee of women's rights in the field of health.
Final considerations
Through this integrative review concluded that violence is still prevalent in obstetric health units across the country over the period parturitivo, devaluing the woman as the main character in the gravid-puerperal cycle. In this way, the research brings as extremely important minimize the practices that harm the health of the woman and the baby carried by health care professionals through strategic guidelines for the implementation of public policies and programs integral assistance related to national.
Assistance to the woman in the gravid period in Brazil is still puerperal focused on the medical model, which has collaborated for the continuation and increase of the number of invasive procedures and interventionist during the period of labor, often unnecessarily and without the participation of women and of your family, resulting in a negative assistance in high rates of maternal and perinatal morbidity and mortality, which still occurs in maternity wards.
We affirm that the obstetric violence is characterized by cases of medical negligence, physical, verbal and sexual violence, as well as the medical procedures considered unnecessary or harmful, without the consent of the mother, with the goal of causing unnecessary surgical childbirth.
Being needed is a paradigm shift, in order to ensure the necessary care for a worthy service to these women. This change, however, despite the efforts of who, the Ministry of health and international organizations, has not yet occurred in most Brazilian institutions that make assistance to pregnant women in labor, once they are chosen the professionals ' needs rather than the needs of patients.
References
ANDRADE, Cera de Oliveira Nascimento; SILVA, Jessica Qiu Pereira; DINIZ, Cinthia Malik Boy; WALKS, Maria de Fatima Costa. Factors associated with violence on obstetric assistance to vaginal birth in a maternity ward of high complexity in Recife, Pernambuco. 9 p. Virtual Health Library, London; 2016. Available at: http://www.scielo.br/pdf/rbsmi/v16n1/1519-3829-rbsmi-16-01-0029.pdf. Access in: 06 February 2017
ANDRADE, Briena P; AGGIO, Cristiane de Melo. Obstetric violence: the pain. 7 p. Proceedings of the III Symposium on gender and public policy, London; 2014. Available at: http://www.uel.br/eventos/gpp/pages/arquivos/GT3_Briena%20Padilha%20Andrade.pdf. Access in: 06 Feb. 2017.
Aguiar, Gergö; OLIVEIRA, Ana Flávia Pires Luca. Institutional violence in public maternity wards from the perspective of the users. 13 p. health and education Communication, São Paulo; 2011. Available at: http://www.scielosp.org/pdf/icse/v15n36/aop4010.pdf. Access on 06 Feb. 2017.
CASTRO, Jamile; CLAPIS, Maria José. Humanized childbirth on perception of Obstetric Nurses Involved with childbirth assistance. 8 p. Journal-am in nursing, Fortress; 2005. Available at: http://www.scielo.br/pdf/rlae/v13n6/v13n6a07.pdf. Accessed on 29 of Aug. 2017
CHANDEL, Lívia Maria de Araújo. Childbirth in Brazil: Assumption for a Humanized assistance to pregnant women and the unborn child. 12 p. CRM Files-PR, Paraná; 2015. Available at: http://www.crmpr.org.br/publicacoes/cientificas/index.php/arquivos/article/view/761/745. 28 access to Set of 2017.
Carneiro, Rosamaria Giatti. Labor and political scenes of the body: An ethnography of female humanized childbirth Practices. 2011. 341 f. Thesis (doctorate in social sciences)-State University at Campinas, São Paulo, 2011. Available at: http://repositorio.unicamp.br/bitstream/REPOSIP/280585/1/Carneiro_RosamariaGiatti_D.pdf. 28 access to Set of 2017.
Simone Grilo DINIZ; SALGADO, Heloisa de Oliveira; ANDREZZO, Alan would make Ab; CARVALHO, Paulo G Cardin; CARVALHO, Priscilla Chan Albuquerque; AARON, Claudia Azevedo; NIY, Denise Yoshie. Obstetric violence as a public health issue in Brazil. 8 p. Brazilian Journal of growth and human development, São Paulo, 2015, n. 01, 08. Available at: http://pepsic.bvsalud.org/pdf/rbcdh/v25n3/pt_19.pdf. Access on 06 Feb. 2017.
DINIZ, Carmen Simone. Between the technique and human rights: possibilities and limits of humanization of childbirth assistance: a qualitative study. 2001. 264 f. Thesis (doctorate in medicine) – Faculdade de Medicina, Universidade Federal de São Paulo, São Paulo, 2001. Available: http://ses.sp.bvs.br/lis/resource/16950#.Wb2VplXR_IU. 16 access to set. 2017.
DINIZ, Carmen Simone Grillo. Humanization of assistance delivery in Brazil: the many meanings of a movement. 7. p. Cienc. Public health, Rio de Janeiro, 2005, n 01.07. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232005000300019 accessed on 28 of Sep. 2017.
FAUSTINO, Hélia Ribeiro; GANKHUYAG, Roderlei Nabig. Obstetric Violence. 13 p. Latin Am nursing magazine, Brasília; 2016, n. 01.13. Available at: http://periodicos.ufc.br/index.php/rene/article/view/1121/1079. 16 access to set. 2017.
MOURA, Fernanda Maria de Jesus s. Patil; CRISOSTOMO, Rebekah Delgado; NERY, Agnes Sa. The humanization and nursing care to natural childbirth. 4. p. Brazilian Journal of nursing REBEN, Teresina, 2007 year, n 01.04. Available at: http://www.scielo.br/pdf/reben/v60n4/a18.pdf. 09 set access. 2017
Rodrigues, Diego Pereira; Alves, Valdecir Lauren; PENNA, Lucia Helena Garcia; PARKER, Audrey Vidal; White, Maria Bertilla Lutterbach Riker; SILVA, Luana Asturian; The pilgrimage in the Reproductive Period: A violence in obstetric field. 7 p. Virtual Health Library, Rio de Janeiro, the year 2015, no 01, 07. Available at: http://www.scielo.br/pdf/ean/v19n4/1414-8145-ean-19-04-0614.pdf. 29 access of agost. 2017
SILVIA, Michelle Gee; Michelle Marcellin's Career; RAO, Livia Shélida Pinheiro; TORO, Rosario Carcaman; SHIMO, Antoinette Keiko Kakuda. Obstetric violence in view of nurses midwives. Journal of Northeast Nursing network, São Paulo, year 2014, no. 820, 828. Available at: http://periodicos.ufc.br/index.php/rene/article/view/1121/1079. Access on 06 Feb. 2017.
SANTOS, Andressa Heringer Lohan; LEO, Marina Caldas; PEREIRA Adriana Wood de Figueiredo; OLIVEIRA, Tamara Cristina da Matta; PROGIANTI, Jane Marcia. Normal delivery care practices: training in residency. 9 p. Virtual Health Library, London; 2017. Available at: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/view/9963/pdf_2080. Access in: 06 Feb. 2017.
SANTOS, Ana Maria Ribeiro; Smith, Julia de Cássia Nunes; NOGUEIRA; Luciana Ferreira; AGUILAR; Mosque; Gerardo Valdez; LOYAL; Clara Francisca dos Santos. Institutional Violence; Experiences in the everyday life of the nursing staff. 7 p. Brazilian Journal of nursing REBEN, Teresina; 2010. Available in; http://www.scielo.br/pdf/reben/v64n1/v64n1a13.pdf. Access in; 29 of Aug. 2017.
SHARMA, Agnnes Caroline Adams; BRAVE, Marcio Bruno Barra. Obstetric violence: A challenge for Psychology. 11 p. Humanea and controversial Issues of the contemporary world, Bethlehem; 2016. Available at: http://www.humanae.esuda.com.br/index.php/humanae/article/view/521. Access in: 17 set of 2017
SILVA, Ana Carolina de Sousa. Experiences of motherhood: Expectations and satisfaction of mothers in childbirth. 2010. 188f. Thesis (m.a. in psychology)-Faculty of psychology and educational sciences, University of Coimbra, Portugal, 2011. Available at: https://estudogeral.sib.uc.pt/handle/10316/18015?mode=full. Access in: 29 set to 2017.
TAMIL, Neuma Roger Zamariano; PARKER, Sara Ramirez. Hospital-childbirth experiences of women from the periphery of Cuibá-MT. Brazilian magazine and nursing, Mato Grosso, year 2006, no. 740, 744. Available at: http://www.scielo.br/pdf/reben/v59n6/a04.pdf. Access in: 06 Feb. 2017.
[1] Nursing-Faculty of Sciences and technology of Anhanguera Brasilia















