MOREIRA, Elizangela Claudia [1], FIUZA, Helenair Farias [2], FECURY, Amanda Alves [3], ABREU, Luciléa de Jesus Madeira Palhano de [4], DIAS, Cláudio Alberto Gellis de Mattos [5], OLIVEIRA, Euzébio de [6]
MOREIRA, Elisangela Claudia. Et. al. Incidence of Psychiatric disorders in pregnancy and Puerperium in women 18 to 35 years in the Charity Hospital Portuguesa de Belem/Pa, Brazil. Magazine Multidisciplinary Scientific Knowledge Center. Year 01, Ed. 05, Vol. 02, May of 2016, pp. 81-93 -ISSN:0959-2448
SUMMARY
Generally speaking people present changes in mood as pleasant or unpleasant events arise in their lives. In pregnancy, serious transformations occur in women, such as: modifying your body and hormones necessary for that to happen the maturation of the fetus. Psychic disorders in the puerperium are among the most serious in psychiatry. The present study aimed to determine the incidence of Psychiatric Disorders (Dysphoria, depression and Psychosis) in pregnancy and puerperium; in women 18 to 35 years, mothers and multiparous from different social classes admitted in the Charity Hospital of Belém, Portugal seeking to identify the possible causes that lead to these disorders in pregnancy and the puerperium. Psychic disorders seem to be often underreported crime, being the Dysphoria more found in this study. The age range of 18 to 24 years with low monthly income appear to be risk factors associated with the disturbance. Monitoring due to these pregnant women during prenatal care could prevent these types of disorders.
Keywords: Pregnancy, Psychic Disorders, health.
INTRODUCTION
Generally speaking people present changes in mood as pleasant or unpleasant events arise in their lives. The intensity and duration of these moods should be proportionate to the moments of life and psicoemocionais conditions of the subject. In the view of psychoanalysis and psychology, this is considered normal. In this way, the psychological disorders can occur to all individuals regardless of class, color, or purchasing power. How these are manifested disorders will depend on this individual vulnerability to natural events and the psychosocial predispositions. One of the important moments and significant, it is usually the pregnancy (CAMACHO et al., 2006).
In pregnancy, serious transformations occur in women, such as: modifying your body and hormones necessary for that to happen the maturation of the fetus. These modifications end up generating doubts, feelings of weakness, insecurity and anxiety (MATTHEWS et al., 2008).
During pregnancy and the puerperium the woman experiencing great changes, both physical and psychological, such as and role in the family and in society. There are changes in your body self-image, disputes feminilidades, sexuality and even pregnancy (ZACK et al., 2003).
In puerperal State the woman undergoes profound physical, psychological and social changes. The psychological changes may be translated on the idea that, in the view of women, pregnancy is the realization of the dream of being a mother. However, because of significant transformations in the body occurs and hormonal changes, planned or not and desired, can trigger psychological conflicts such as: dysphoria, postpartum depression and puerperal psychosis, causing many times, sense of fragility, insecurity and anxiety. Especially in cases of Primiparous Women, where pregnancy becomes a novelty associated with the lack of experience, causing feelings of fear and fear of not knowing how to deal with the situation (CAMACHO et al., 2006; MOREIRA et al., 2008).
Zack et al. (2006), stated that puerperal stage the woman is exposed to greater risks of appearances of mental disorders in other stages of life, since the two saves, both physical, psychosocial, as are directed to protection and vulnerability.
Second Neme (2005) and Moura et al., (2011), the psychic disorders in the puerperium are among the most serious in psychiatry. Presenting risk so much to mother as well as for the newborn, and classified into lighter frames called gender dysphoria in the puerperium and puerperal depression and in more serious paintings, called psychotic disorders.
The gender dysphoria postpartum or also called “Puerperal blues”, where occurs sudden change of mood and may also be feelings as sadness, anguish, melancholy, pessimism and feeling of shame, considered by some authors as a physiological phenomenon common in puerperium (NEME, 2005).
Sudden changes of depressive mood appear in the early days of postpartum and tends to decrease on the tenth day of puerperium. Are usually mild depressive symptoms accompanied by emotional instability, tension and irritation that not enough to compromise the relationship with mother and newborn, and there is no need for medical treatment, the persistence of that humor does not disappear from the eleventh day, can be seen as a possible major depression, requiring appropriate assessment and treatment (NEME, 2005; CAMACHO et al., 2006).
Depression is characterized by a State of sadness, sleep disorders, feelings of guilt, indecision, discouragement, anorexia, inadequate to meet the newborn. Usually, depression can mean either an affective state as a symptom, a syndrome or various diseases (RAJAN and ADHIKARI, 2005).
According to Sotto-Mayor and Piccinini (2005); Fonseca e Silva (2010) and Moura et al., (2011), postpartum depression is a depression that appears in most transitional of women after the baby is born.
The clinical picture of post-partum depression is highly variable, and may present physical, cognitive and behavioral changes, is characterized by symptoms such as sadness, crying easily, despondency, depression, anorexia, lability, sometimes accompanied with nausea, sleep disorders, especially insomnia and nightmares, included also the own baby care, such as feelings of not loving him enough, fear of harm, anxiety sleep and feeding the child feeling of inability for a proper care (ZACK et al., 2003).
Postpartum depression is a psychiatric disorder that causes great suffering for the mom and upsets the mother-child interaction, wife-husband and family relationship (ZACK et al., 2003; FONSECA et al., 2010; MOURA et al., 2011).
One of the factors that may contribute to the high rate of depression in pregnancy and puerperium in adolescence is the lack of affective maturity of these patients relationships, unwanted pregnancy due to unresolved relationships, as well as the fact that many have to give up their freedom of youth or even having to abandon their studies because of pregnancy (SZIGETHY , 2001).
The puerperal psychosis represents the frame and less frequent, being its incidence found between 1% for each births (oak, 2007). Some risk factors for puerperal psychosis can be related to history of previous psychiatric disorder, stressful events, marital conflicts, being single or divorced, or have little social support (CAMACHO et al., 2006).
The puerperal psychosis is among the most serious frames in Psychiatry, representing the risk to both the mother and the baby. Develops between the third and fourteenth day postpartum, this related to primiparity and single mothers. This occurs when there is a personal or family history of mental illness, hormonal changes and psychosocial stresses (NEME, 2005).
According to Nunes Filho and Bueno (2005), the post-partum psychosis should not be confused with postnatal sadness, (“Postpartum blues”) due to being a normal condition that affects in about 50% of women.
It is important that the health professional can identify the characteristics of psychological disorders in pregnancy during the prenatal period and puerperium, taking home the first three weeks of the puerperium with high incidence and bringing consequences for mother and child. The professional should have proper care and attention the recent mothers to identify and intervene more precociously in the treatment and in the knowledge of the condition, because the psychosis is the depression that has high prevalence, and divergences between authors on the factors related to this pathology (HIGUTI, 2003).
Being the pregnancy a normal process of human development, with large organic transformations, psychic and family partner. The assistance provided should be providing full satisfaction and wellbeing woman, aiming at the strengthening of the bond between a mother-baby (FALCONE et al., 2005).
Some mothers feel ashamed to demonstrate to his doctors and family the depressive symptoms, failing to meet its new responsibilities, appearing on them, a sense of guilt for not experiencing this moment in a satisfactory manner, with the need of the professional identify the symptoms, to interact and leave the mother more safe to expose your problem (PEIXOTO, 2007; GARCIA et al., 2010).
The professional should aim to understand the emotions, feelings, fantasies, fears and stress relieve the anxieties present the patient, noting the States of confusion on mother between the period of the pregnancy and after the baby is born. The feelings and thoughts about who has recently given birth interfere and hinder the activities faced in day to day professional. Therefore, the assistance should identify in their dislike to the baby who has recently given birth, sadness, estrangement, absence, loss of appetite, carelessness of self care, insomnia, preserving the regular sleep and rest of who has recently given birth so you can face your required activities with the baby (TRUCHARTE et al., 2010; VIEIRA et al., 2011).
The service explains, supports and lessens the anxiety of the mother, that is, it provides benefit to women, facilitating the expression of their feelings on the changes of motherhood. Treatment includes antidepressants, psychotherapeutic approach, guidance, support, home visits until complete remission of depression or psychotic (ZACK et al., 2003).
On the basis of the above, the present study aimed to determine the incidence of Psychiatric Disorders (Dysphoria, depression and Psychosis) in pregnancy and Puerperium in women 18 to 35 years of Primiparous and multiparous, of different social classes admitted in the Charity Hospital of Belém, Portugal seeking to identify the possible causes that lead to these disorders in pregnancy and the puerperium.
METHODOLOGY
This study was done by quantitative research, performed by database research, seeking to identify the incidence of the three States of psychic disorders in pregnancy and the puerperium (Dysphoria, depression, psychosis), in 100 women from 18 to 35 years, mothers and multiparous from different social classes met in the maternity ward of the Hospital Benefit Portuguesa de Belém do Pará, in the period from March to April 2014. Were excluded mothers under the age of 18 years and older than 35 years. The Excel Office program from Microsoft Corporation was used in the Organization and data tabulation and statistical analysis.
RESULTS
During pregnancy
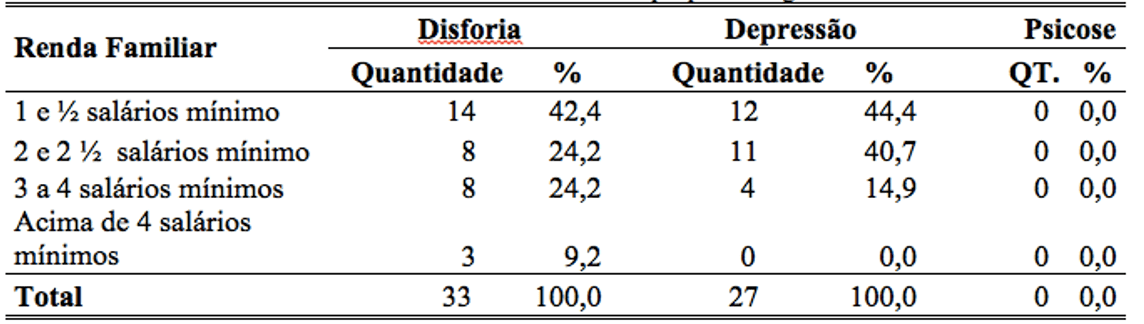
On the basis of the results collected in the database, of the 33 women who have signs and symptoms of Dysphoria during pregnancy, most owned income between 1 and .5 minimum wages, representing 42.4% of these women. Twenty-seven submitted signs and symptoms of Depression representing 44.0% who also has income between 1 and .5 minimum wage (table 1).
Table 1: percentage of minimum income of women with psychological disorder in pregnancy.
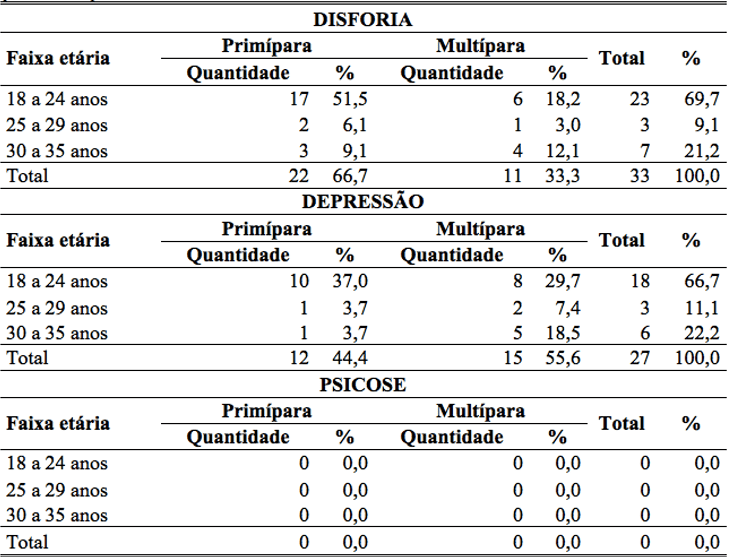
33 women showed signs and symptoms of Dysphoria. It was found that most (66.7%) are young first-time mothers, and 33.3% are multipara. The young first-time mothers, 17 women (51.5%), between the ages of 18 and 24 showed years. The multiparous, 6 women (18.2%) were between the ages of 18 and 24 years. In total, women who have gender dysphoria in the age group of 18 to 24 years between Primiparous and multiparous comprise 69.7%, and those of age groups between 25 to 35 years between Primiparous and multiparous totaling 30.3%. With regard to women with Depression, it was found that most are multipara. Of the 27 women who showed signs and symptoms of Depression, 15 were multiparous 55.6%, representing and representing 44.4% 12 mothers, especially also in the age group of 18 to 24 years, which totals between Primiparous and multiparous 66.7%, and the remaining age groups a minority of 33%. There has been cases of women with Psychotic Disorders during pregnancy (table 2).
Table 2: percentage of women with psychic disorder during pregnancy, in the age group of 18 to 35 years, Primiparous and multiparous.
During the Puerperium
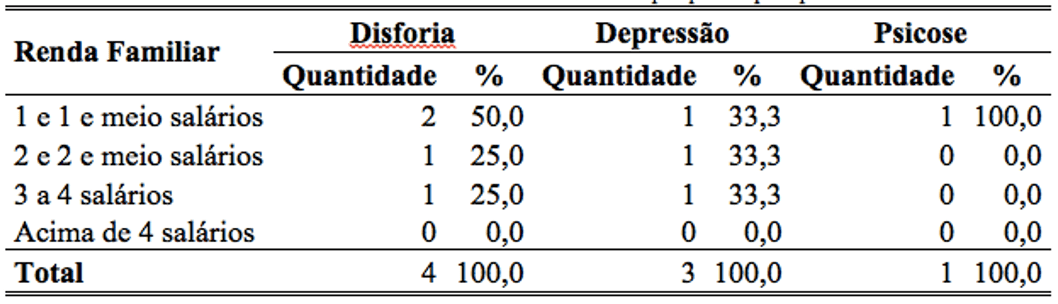
It was found that in the puerperium, of 100 women, 4 showed signs of Dysphoria most with incomes between 1 and .5 minimum wages, (50%). Already in relation to depression, it was found that more than 65% presented minimum income below 3 minimum wages, and the signs of psychosis, only one case (100%) with income between 1 and .5 minimum wage (table 3).
Table 3: percentage of minimum income of women with psychic disorders.
Four women showed signs and symptoms of Dysphoria. It was observed that the majority (75%) are young first-time mothers in the age group of 18 to 24 years, while 25% are aged 30 multiparous to 35 years. Already towards women with depression, it was found that 66.7% are mothers between the ages of 18 to 24 years and 33.3% are aged 30 multiparous to 35 years, while women with psychosis, only 1 (100%) case of woman multípara with age in the age group between 30 and 35 years (table 4).
Table 4: percentage of women with puerperal psychic disorder between the ages of 18 to 35 years, Primiparous and multiparous.
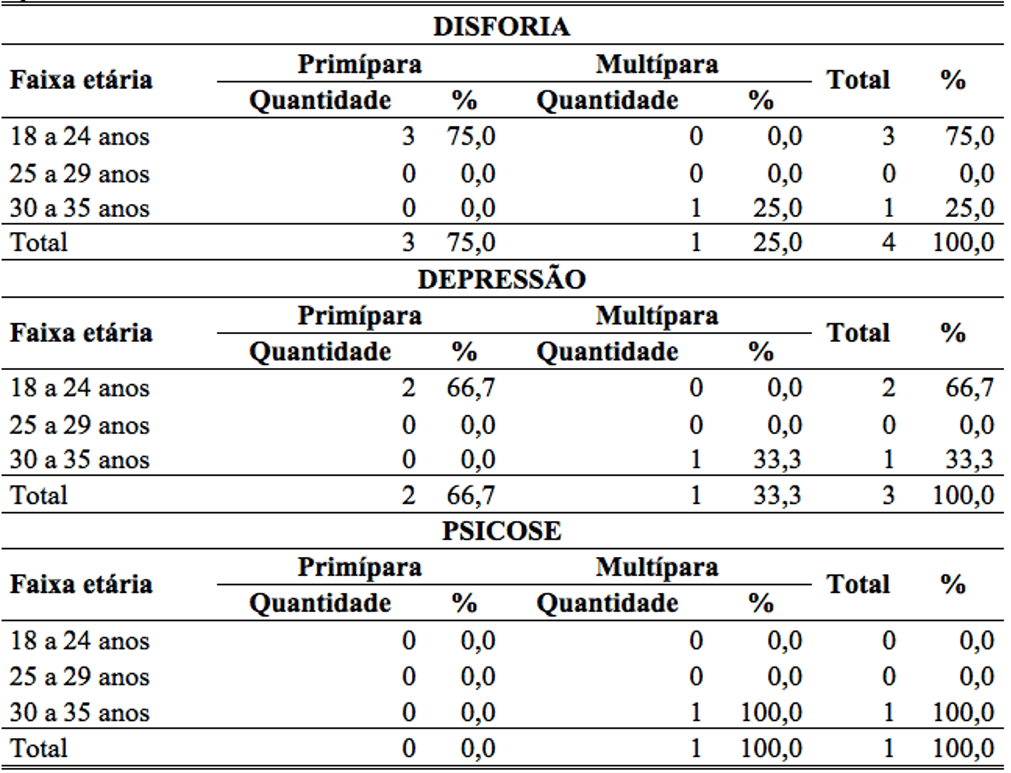
Table 5 shows that women, 60% presented some sort of psychic disorder during pregnancy. Of these, 83% did not seek the help of a healthcare professional, while only 17% sought a health care professional. Of the women who sought help from a health professional, 40% spoke with psychologist, while 30% spoke with nurse, 10% spoke with gynecologist and 20% spoke with obstetrician.
Table 5: percentage of women who have or not psychic disorders during pregnancies and reported to a health care professional.
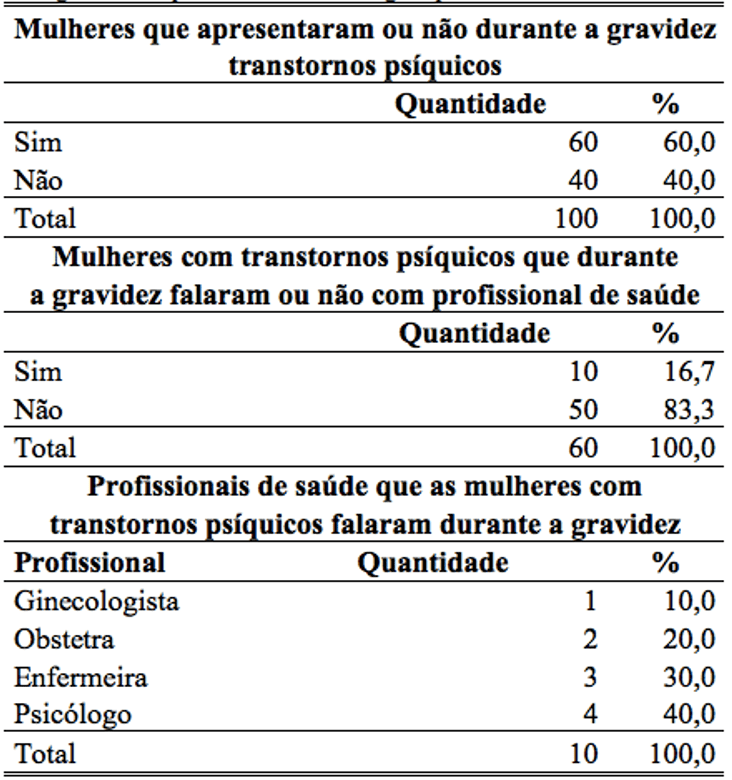
Source: Portuguese Charity Hospital, Bethlehem PA, 2014.
DISCUSSION
The present study had the Dysphoria as the most common disorder. The prevalence was about 66.7% of the pregnant women and 75% of postpartum mothers between the ages of 18 to 24 years with monthly income of 1 and .5 minimum wage. According to Moreira et al., 2008, pregnancy affects functioning women’s hormone causing bodily transformations necessary for that to happen the maturation of the fetus, these modifications end up generating doubts, feelings of weakness, insecurity and anxiety, leading to the framework of gender dysphoria. Featuring: sudden change of mood, and may also be feelings such as sadness, anguish, melancholy, pessimism and sense of shame. Although the dysphoria be regarded as a mild depressive disorder not requiring medical treatment, their persistence can be looked at as a possible major depression, requiring appropriate assessment and treatment (NEME, 2005).
Signs and symptoms of depression during pregnancy were found in 55.6% of multiparous postpartum of 66.7% and also the same age groups and monthly income. It is assumed that the high rate in this age group may be related to inexperience, immaturity, unwanted pregnancies because of unresolved relationships, as well as the fact that many have to give up their freedom of youth or even having to abandon their studies because of pregnancy (SZIGETHY; RUIZ, 2001).
With relation to puerperal psychosis, this represents the frame more serious and less frequent, being its incidence found between 1% for every birth (oak, 2007).
In this study, the 100 mothers only a multípara between the ages of 30 to 35 years showed symptoms of psychosis such as: insomnia, restlessness, irritability, crying, difficulty concentrating. It is assumed that the late gestation, multiparidade, history of psychiatric disorder, marital conflicts, being single or divorced, or have little social support, may be risk factors for this disorder (CAMACHO et al., 2006).
A fact that deserves attention in this study is that of the 100 women who have some kind of psychic disorder during pregnancy, only 17% sought a health care professional to report their symptoms. The remaining 83%, i.e. most reported symptoms. It is believed that for fear of possible stigmatization (EPPERSON, 1999); for some mothers feel ashamed to demonstrate to their doctors symptoms; for they think they can’t meet its new responsibilities, appearing on them, a sense of guilt for not experiencing this moment, feeling sad, unhappy, at a time when they should be feeling Jolly (PEIXOTO; Amorim, 2007).
It is believed that the good service clarifies, supports and lessens the anxiety of the mother, making the expression of their feelings on the changes of motherhood (ZACK et al., 2003).
CONCLUSION
Psychic disorders appear to be more frequent in pregnancy and puerperium, not being often underreported crime. The Dysphoria the framework of highest incidence, and despite being regarded as a mild depressive disorder, usually do not require medical treatment, their persistence can be seen as a possible major depression, requiring appropriate assessment and therapeutic management. The age range of 18 to 24 years with low monthly income appear to be risk factors associated with these disorders.
Monitoring due to pregnant women during prenatal care could prevent these types of disorders. For that, the pros need to be enabled, willing to listen carefully to pregnant women and recent mothers to identify and intervene more precociously in the treatment and understanding of pathology.
REFERENCES
CAMACHO, R.S. et al. Psychiatric disorders in pregnancy and the puerperium: classification. Diagnosis and treatment. Revista de Psiquiatria Clinica. Clin. Vol. 33, no. 2-São Paulo, 2006.
CARVALHO, Geraldo m. nursing in Obstetrics. 3 ed. rev. and ampl. São Paulo: E.P., 2007.
EPPERSON, CN. Postpartum care major depression: detection and treatment. Am Fam Physician 59 (8): 2247-2254, 2259-2260, 1999.
FALCONE, v. m. et al. Multidisciplinary activities and the mental health of pregnant women. Public health magazine, São Paulo, mar. 2005, v. 39 (4): 612-8.
FONSECA, V. R. J. R. M.; SILVA, G. A. D.; OTTA, e. relationship between postpartum depression and maternal emotional availability. CAD. Public health, v. 26, n. 4, p. 738-746, 2010.
GARCIA, L. A. et al. Identification of risk factors for post-partum depression: the importance of early diagnosis. Rev. Rene, v. 11, p. 117-123, 2010.
HIGUTI, P. C. L.; CAPOCCI, p. o. postpartum depression. Journal of nursing of UNISA, 2003; 4:46-50.
MATTHEWS, t. m. M et al. Conflicts experienced by teenagers with the discovery of pregnancy. Rev. Esc. Nurses. USP, 2008:32 (2) 312-20.
MOURA, E. C. C.; FERNANDES, M. A.; APOLLINARIS, f. i. r. maternal Perception about psychiatric disorders in puerperium: implications for the mother-child relationship. Rev Bras Nurses, v. 64, n. 3, p. 445-50, 2011.
NEME, Bussâmara-1975. Obstetrics. 3 ed. São Paulo, 2005.
NUNES FILHO, E. P.; BUENO, J. R.; NARDI, e. Psychiatry and mental health: clinical and therapeutic concepts. São Paulo: Editora Atheneu, 2005.
PANDEY, D. F.; Amorim, v. c. of Psicoembriologia the puerperium: awareness of the mother-baby relationship. Electronic journal of Psychology. 1 year, n. 1, jul. 2007.
RIBEIRO, W. G.; ANDRADE, m. the nurse’s role in the prevention of postpartum depression (PPD). Report on health prevention, v. 5, n. 1. P. 07-09, 2009.
SOTTO-MAYOR, I. M. B.; PICCININI, c. a. marital relationship and maternal depression. Psycho. v. 36, n. 2, p. 135-138, may/Aug, 2005.
SZIGETHY, E.M.; RUIZ, p. Depression among pregnant adolescents: an integrated treatment approach. Am J Psychiatry 158 (1): 22-27, 2001.
TRUCHARTE, F.A.R.; KNIJNIK, R. B.; SEBASTIANE. R. W.; ANGERAMI-CAMON, v.a. (organizer). Hospital Psychology: theory and practice 2 revised and enlarged edition. São Paulo: Cengage Learning, 2010.
VIEIRA, A. P. et al. Prevalence of post-partum depression in women of a University Hospital. Annual production of scientific initiation Students, v. 14, n. 25, p. 311-321, 2011.
ZACK, D. V et al. Identification and intervention psychiatric disorders associated with the puerperium: a collaboration with nurse psychiatrist. Nursing magazine, v. 61, n. 6, p. 36-42, jun. 2003. 1 CD-ROM.
[1] Psychologist. Master in theory and research. Lecturer at the University of the State of Pará-UEPA. A researcher at the Graduate program of the Center for Tropical Medicine of the UFPA.
[2] Metropolitan College Studen from Amazon.
[33] Biomedical. Doctorate in Tropical Diseases. A researcher at the Graduate program of the Center for Tropical Medicine of the UFP. Lecturer and researcher at the Federal University of Amapá, AP. Email: [email protected]
[4] Metropolitan College Studen from Amazon. A researcher at the Graduate program of the Center for Tropical Medicine of the UFPA.
[5] Biologist. Doctor in theory and research. Lecturer and researcher at the Federal Institute of Amapá-IFAP.
[6] Doctor of medicine/Tropical Diseases. Researcher of the Graduate program of the Center for Tropical Medicine of the UFPA. Lecturer and researcher at the Federal University of Pará – UFPA.















