ORIGINAL ARTICLE
LOREDO, Felipe Pereira de [1], BIANCO, Sabrina Ramos [2], SILVA, Sildomar Queiroz e [3], COELHO, Daniella Paula Dias [4]
LOREDO, Felipe Pereira de. Et al. Comparison between tomosynthesis and breast magnetic resonance imaging to assess tumor response after neoadjuvant chemotherapy: a case report. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 06, Ed. 07, Vol. 12, pp. 56-65. July 2021. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/neoadjuvant-chemotherapy, DOI: 10.32749/nucleodoconhecimento.com.br/health/neoadjuvant-chemotherapy
ABSTRACT
Increasingly, the surgical treatment of breast cancer has been preserving as much tissue as possible, avoiding mutilating surgeries such as mastectomies. Therefore, it is necessary to analyze the morphological characteristics, location and size of the tumor, and neoadjuvant chemotherapy is often used to reduce the tumor mass and thus enable conservative surgery. The evaluation of tumor response to neoadjuvant chemotherapy has magnetic resonance imaging as the gold standard, which, however, is not always accessible, has a high cost and is contraindicated for claustrophobic and obese patients. Tomosynthesis is a 3D mammography method that proposes to reduce tissue overlap and provide a better definition of tumor borders. So, could tomosynthesis be an alternative to magnetic resonance imaging for this evaluation? This work shows a case report where tomosynthesis offered quality information as reliable as magnetic resonance imaging for the evaluation of tumor response and even better visualization of the marker by a metal clip inside.
Keywords: Tomosynthesis, Magnetic Resonance, Breast neoplasm.
INTRODUCTION
Conventional mammography stands out as a screening method and early detection of breast cancer, showing good sensitivity for the detection of malignant lesions, but tissue overlap is a limitation in the identification of some lesions (ALSHAFEIY et. al., 2018) .
Tomosynthesis or 3D mammography is an image acquisition method that, through angulations, reduces or even suppresses the overlapping of tissue in the image, thus increasing the detection of lesions by about 30% when compared to 2D mammography (VILAVERDE et al. ., 2016).
Although the gold standard for evaluating tumor response after neoadjuvant chemotherapy is magnetic resonance imaging, it is difficult for patients to access, being an expensive and time-consuming method (the necessary sequences take between 30 minutes to 1 hour), not always available, and patients claustrophobic or obese people have restrictions or cannot be submitted to it (SEABRA and LOURENÇO, 2014). In this way, could tomosynthesis, which is a more available method, evaluate and monitor the control in the therapeutic response, replacing magnetic resonance?
There is evidence that the margins of the lesions are well evidenced in tomosynthesis, due to less tissue overlap. Thus, we consider that it could be a very useful tool for these cases, in addition to directing the evaluation of microcalcifications in case they exist or appear (PEPPARD et. al., 2015).
More and more, breast specialists and oncologists choose neoadjuvant chemotherapy, even in cases of non-advanced cancer, as it allows for better aesthetic results, better surgical planning, reduction of local recurrence and impact on the overall survival of the patient (CHESEBRO et al., 2017). ).
In this work, we will present a case report of a patient who presented a malignant nodular lesion, where we opted for the implantation of a metal clip and evaluation by tomosynthesis and magnetic resonance imaging of the results of neoadjuvant chemotherapy in the reduction of tumor mass. This evaluation aimed to perform a conservative surgery, thus avoiding mastectomy.
CASE REPORT
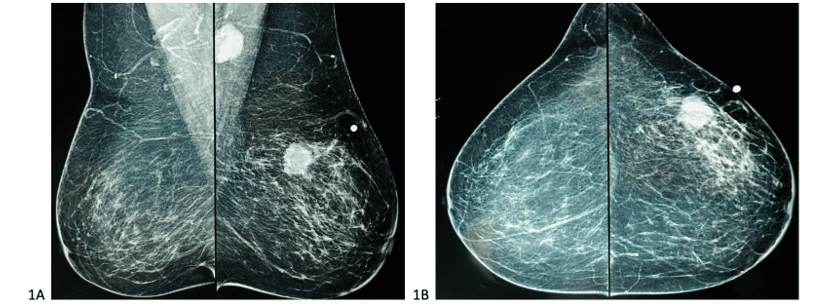
A 67-year-old female patient with no previous comorbidities noticed the presence of a lump in the left breast, with a mammogram showing a spiculated nodule associated with lymph node enlargement in the axillary region. She underwent core biopsy for histopathology and immunohistochemistry, which confirmed it to be a triple-negative infiltrative ductal carcinoma (estrogen receptor negative, progesterone receptor negative and HER2 negative). It was then decided to perform neoadjuvant chemotherapy, to perform a reconstructive surgery and lymphadenectomy. Marking the nodule using a metal clip was necessary to guide the evolution of the tumor mass.
Image of the first diagnostic mammogram performed by the patient:
Figure 1. Diagnostic mammography showing a suspicious nodule in the upper lateral quadrant of the left breast, associated with ipsilateral axillary lymph node enlargement.
Images before and after neoadjuvant chemotherapy:
Figure 2. Incidence synthesized in MLO[5] performed by tomosynthesis showing a nodule marked by a clip, performed before and after neoadjuvant chemotherapy respectively in 2A and 2B, showing in B the reduction of the tumor mass and absence of lymph node enlargement.
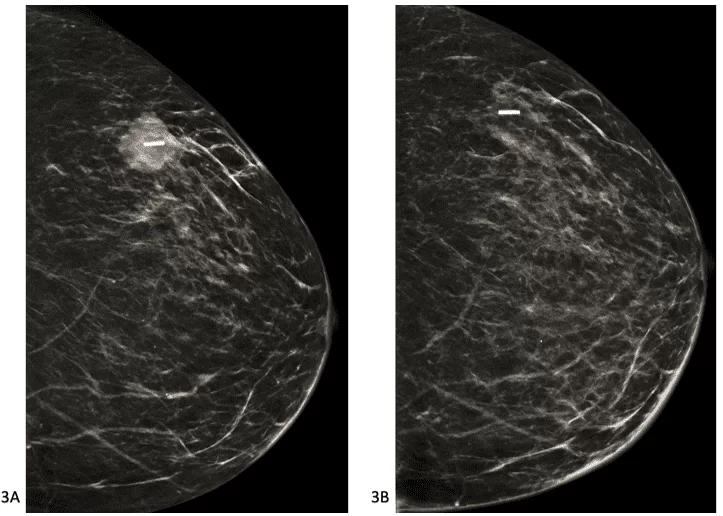
Figure 3. Incidents synthesized in CC[6] performed by tomosynthesis showing a nodule marked by a clip, performed before and after neoadjuvant chemotherapy, respectively in 3A and 3B, showing the reduction of the tumor mass in 3B.
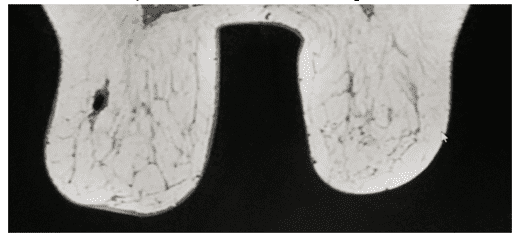
Figure 4. T1-weighted axial magnetic resonance imaging of the breasts with fat suppression after contrast, performed before and after neoadjuvant chemotherapy, respectively, in 4A and 4B, showing the reduction in tumor mass in 4B.
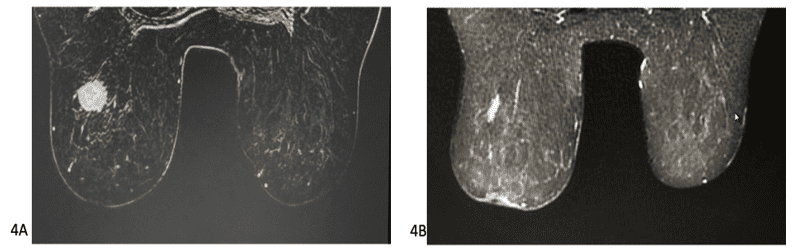
Figure 5. T1-weighted sagittal magnetic resonance imaging of the breasts with fat suppression, after contrast, performed before and after neoadjuvant chemotherapy, respectively, in 4A and 4B, showing a reduction in tumor mass and absence of lymph node enlargement in 4B.
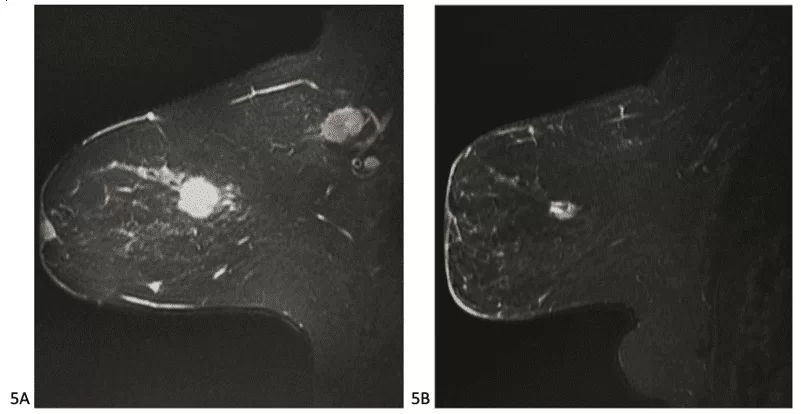
Figure 6. Axial magnetic resonance imaging of the breasts at T1 weighting, performed after neoadjuvant chemotherapy, showing the reduction of the tumor mass with a metallic clip visualized inside the remaining nodule.
Pre-chemotherapy tomosynthesis showed a high-density spiculated nodule, located in the middle portion of the superolateral quadrant of the left breast, measuring about 2.8×2.6×2.1cm (volume of 8.0cm3) and lymph node enlargement measuring 2.5cm . Post-neoadjuvant chemotherapy tomosynthesis showed a reduction of the nodule to 1.6×1.1×1.0 cm (volume 0.91 cm3) and absence of lymph node enlargement.
Pre-neoadjuvant chemotherapy MRI showed a solid nodule in the left breast, in the superolateral quadrant, in the middle third, with hypersignal on T2, with spiculated margins, showing intense enhancement after intravenous contrast, measuring 2.9×2.6×2.3cm (volume of 9.0cm3). In addition to presenting left axillary lymph node enlargement, with loss of usual morphology, signs of restriction to the diffusion sequence and irregular contours, measuring 2.6 cm. Post-chemotherapy MRI showed a reduction of the nodule to 1.9×0.9×0.9cm (volume 0.8cm3) and absence of lymph node enlargement.
The product of the quadrant and axilla of the left breast showed, in the anatomopathological examination, after neoadjuvant chemotherapy, residual alterations from previous antineoplastic treatment, with complete response of the material examined.
DISCUSSION
Tomosynthesis reduces the effect of overlapping fibroglandular tissue allowing an increase in lesion detection, morphological characterization and location, in addition to reducing the rate of recall (CHONG et al., 2019).
Neoadjuvant chemotherapy is chemotherapy performed before surgery with the aim of reducing the size of the tumor, making it operable and allowing for more conservative surgery. The purpose of placing the clip on the tumor bed is to show the examiner the location and size of the tumor in the complete or partial response after neoadjuvant chemotherapy (POLAT et al., 2018).
In patients who will undergo implantation of a metal clip inside the lesion, for control after neoadjuvant chemotherapy, tomosynthesis may be an alternative to magnetic resonance imaging, as it allows better visualization of the metal clip due to the sensitivity of the metal to x-rays ( BURBANK and FORCIER, 1997); verifies the definition of lesion margins, tumor spicules and their extension, controlling the tumor volume, as 3D images are obtained (THOMASSIN-NAGGARA et. al., 2012); it has the shortest time to carry out the study and there is no limitation regarding obese and claustrophobic patients (ALVARES and MICHELL, 2003).
Routine clinical treatment of breast cancer depends on traditional prognostic factors, including nodal status, histological tumor grade and primary tumor size, in addition to estrogen receptor, progesterone receptor and HER2[7] (CARVALHO, 2010).
Triple negative breast cancers account for about 20% of all diagnoses, being more common in young women, they do not express estrogen, progesterone and HER2 receptors. Although they may appear more aggressive due to these characteristics, they may respond well to neoadjuvant chemotherapy, and the earlier they are diagnosed, they have a greater chance of cure (LOPES, 2015). These data from the literature were confirmed in the present case, since the patient, although already presenting lymph node dissemination, had a complete response to neoadjuvant chemotherapy, shown as regression of the tumor mass both in tomosynthesis and resonance exams, what remained was fibrotic tissue, which was confirmed with histopathology after surgery.
CONCLUSION
Although the gold standard of breast lump tumor response after neoadjuvant chemotherapy is magnetic resonance imaging, tomosynthesis can satisfactorily assess the tumor mass in subsequent examinations, in addition to better showing the location of the metal clip, which are essential data for the surgeon. Therefore, it can replace resonance when it is not possible to perform. The case presented in this article obtained a complete response in the tumor regression, which allowed a conservative surgery, increasing the possibilities of cure for the patient.
REFERENCES
ALSHAFEIY, Taghreed I. et. al. Outcome of Architectural Distortion Detected Only at Breast Tomosynthesis versus 2D Mammography. Radiology. Ano 2018, Vol. 288, No. 1, pp. 38-56. Doi: 10.1148/radiol.2018171159.
ALVARES, Beatriz Regina; MICHELL, Michael. O uso da ressonância magnética na investigação do câncer mamária. Radio Bras. Ano 2003, Ed.36, No 6. Doi: https://doi.org/10.1590/S0100-39842003000600009
BURBANK, F.; FORCIER, N. Tissue marking clip for stereotactic breast biopsy: initial placement accuracy, long-term stability, and usefulness as a guide for wire localization. Radiology. Ano 1997, Vol. 205, No 2, pp. 407–415. Doi: 10.1148/radiology.205.2.9356621
CARVALHO, Filomena M. et. al. Triple-negative breast carcinomas are a heterogeneous entity that differs between young and old patients. Clinical Sciences. Ano 2010, Ed. 65, No 10. Doi: 10.1590/S1807-59322010001000019.
CHESEBRO, Allyson L. et. al. Troubleshooting to Overcome Technical Challenges in Image-guided Breast Biopsy. Radiographics. Ano 2017, Vol 37, No. 3, pp. 705-718. Doi: 10.1148/rg.2017160117
CHONG, Alice et.al. Tomossynthesis: Concepts and Clinical Practice. Radiographics. Ano 2019, Vol.292, No. 1, pp. 1-14. Doi: 10.1148/radiol.2019180760
LOPES, Camila M. et. al. Fatores prognósticos clínicos, histomorfológicos e terapêuticos em pacientes com câncer de mama invasivo triplo negativo. J. Bras. Patol. Med. Lab. Ano 2015, Ed. 51, No. 5, pp. 397-406. Doi: www.dx.doi.org/10.5935/1676-2444.20150062
PEPPARD, Heather R. et. al. Digital Breast Tomosynthesis in the Diagnostic Setting: Indications and Clinical Applications. Radiographics. Ano 2015, 35(4):975-90. Doi: 10.1148/rg.2015140204
POLAT, Yasemin Durum et. al. The role of tomosynthesis in intraoperative specimen evaluation. The Breast Journal. Ano 2018, Vol 24, Issue 6, pp 992-996. Doi: doi.org/10.1111/tbj.13070
SEABRA, Zita Teresa; LOURENÇO, João. Imagiologia no Carcinoma da Mama. Revista Portuguesa de Cirurgia, Ano 2014, n. 27, pp. 59-70, ISSN 2183-1165. Disponível em: <https://revista.spcir.com/index.php/spcir/article/view/330>. Acesso em 15/07/2021.
THOMASSIN-NAGGARA, Isabelle et. al. A plea for the biopsy marker: how, why and why not clipping after breast biopsy? Breast câncer Res Treat. Ano 2012, Ed. 132, No 3, pp 881-93. Doi: 10.1007/s10549-011-1847-x
VILAVERDE, Filipa et. al. Tomossíntese mamária: O que o radiologista deve saber. Acta Radiológica Portuguesa. Ano 2016, vol 28, No. 109, pp. 35-41. Disponível em: < https://www.sprmn.pt/revista/arp109/pdf/ARP%20109%20artigo_revisao2.pdf>. Último acesso em 15/02/21.
APPENDIX – FOOTNOTE
5. Mediolateral oblique.
6. Craniocaudal.
7. Human epidermal growth factor receptor 2.
[1] Resident Doctor of Radiology and Diagnostic Imaging at the Fundação Centro de Controle de Oncologia do Amazonas.
[2] Physician, Titular Member of the Brazilian College of Radiology, Qualification in Mammography, Coordinator of the Radiology Sector of the Fundação Centro de Controle de Oncologia do Amazonas, Coordinator of the Breast Sector of the Sensumed Clinic for Oncology Therapy and Imaging Diagnosis.
[3] Resident Physician of Radiology and Diagnostic Imaging at Fundação Centro de Controle de Oncologia do Amazonas.
[4] Resident Physician of Radiology and Diagnostic Imaging at Fundação Centro de Controle de Oncologia do Amazonas.
Sent: July, 2021.
Approved: July, 2021.















