DUTRA, Júlia Cunha [1]
TAVARES, Sheila Lucas da Silveira [2]
DUTRA, Júlia Cunha; TAVARES, Sheila Lucas da Silveira. Diabetes Mellitus as Primary Illness in Chronic Kidney Patients Users of the Hemodialysis Service of Bagé / RS. Multidisciplinary Scientific Journal. Edition 05. Year 02, Vol. 01. pp. 187-202, July 2017. ISSN:2448-0959
SUMMARY
With knowledge about the evolution of chronic diseases with hypertension and diabetes for chronic kidney disease, this research was carried out with the main objective of evaluating the occurrence of diabetes mellitus prior to chronic kidney disease in hemodialysis patients. The study sample comprised 20 users of the nephrology service of a city in the interior of the Region of Campanha – Rio Grande do Sul, data were collected in the months of April and May 2017, through an instrument containing ten questions that were recorded and later transcribed. To analyze the data, we used the Bardin Content Analysis Technique, which consists of three phases: pre-analysis, material exploration and treatment of results, and interpretation. The results showed that nephrology service users are mostly adults and elderly, and when patients with diabetes mellitus are type II, it is necessary the screening of comorbidities as recommended in the health protocols. It was also evident that health information when isolated is not sufficient for users to adhere to the recommended treatments, and these should be oriented on the aggravations that may still arise, even though they are already in treatment, so there is a need to implement the care that aiming at the promotion of health education aimed at the users' knowledge about the complications of their disease, providing a continuity of the health team's assistance in terms of knowledge, in order to promote self-care and increase the quality of life of this population .
Keywords: Diabetes, Chronic Kidney Disease, Health Education.
INTRODUCTION
Diabetes Mellitus is no longer a disease prevalent in rich countries, has been growing worldwide in recent years, especially in developing countries (WHO, 2016). The increase in DM cases is directly related to population growth and aging, greater urbanization, the progressive prevalence of obesity and sedentary lifestyle, and therefore, quantifying the current prevalence of DM and estimating the number of future cases is important because it allows planning and allocate resources in a rational way (BRAZILIAN DIABETES SOCIETY, 2015).
According to Nettina (2011) and Guyton and Hall (2011) diabetes mellitus occurs when the body does not produce the hormone insulin enough or when the body can not adequately use the available insulin, this hormone is responsible for allowing the glucose into the cells, thus providing control of blood glucose levels.
It is estimated that the number of diabetics has almost doubled since 1980, reaching 422 million adults living with diabetes in 2014, a total of 8.5% of the world's adult population, and type II diabetes currently accounts for 90% of cases of diabetes (WHO, 2016).
In situations where blood glucose levels are not controlled, even with medication, damage to various organs and tissues, especially kidneys, heart, eyes and nerves can occur. In addition to the possibility of injury to the blood vessels of the renal system, which may lead to diabetic nephropathy and renal failure (BRAZIL, 2013).
Diabetes is associated with increased mortality, especially if it is associated with cardiovascular diseases, and although the rate of more advanced chronic complications related to DM has been decreasing in the last decades, the number of affected users is still very large in view, because the incidence of DM has increased considerably (BRAZILIAN DIABETES SOCIETY, 2015).
METHODOLOGY
TYPE OF RESEARCH
This qualitative, analytical, descriptive study was carried out with a data collection from a questionnaire applied to the users of the hemodialysis service of the Nefro Rim Sul Clinic, in the city of Bagé, State of Rio Grande do Sul. The same, it complied with Resolution 466/2012 of the National Health Council that defines as research involving human beings any that individually or collectively directly or indirectly involves the human being, in its entirety or parts of it, including the management of information or materials.
By answering very particular questions, qualitative research is concerned with a level of reality that can not be quantified, since it works with a universe of motivations, aspirations, beliefs, values and attitudes that can not be reduced to the operations of variables (MINAYO , 2001).
A complete description of a population concept, in order to define the characteristics of the totality or part of the study population, characterizes a descriptive study (FORTIN, 2009).
STUDY POPULATION
Twenty interviews were conducted with the users of the Bagé nephrology service who were undergoing hemodialysis as renal replacement therapy, with exclusion criteria covering patients who underwent other treatments than hemodialysis, as well as those who did not wish to participate or sign the TCLE.
LOCATION AND PERIOD OF PERFORMANCE OF THE RESEARCH
The study was conducted at the Nefro Rim Sul Clinic, in the Municipality of Bagé, State of Rio Grande do Sul, in the months of April and May 2017.
DATA COLLECTION PROCEDURES
The data were collected through a questionnaire, consisting of ten open questions, which were later transcribed and analyzed. Together with the questionnaire, the participant was given the Free and Informed Consent Term, which after being clarified was signed by the participant who agreed to participate.
Twenty interviews were conducted and the interviewees received guidance on recording responses for later transcription.
DATA ANALYSIS PROCEDURES
After the data collection, they were transcribed for further evaluation, which, according to Bardin (2006) occurs in three stages: 1) pre-analysis, 2) exploration of the material and 3) treatment of results, inference and interpretation.
ETHICAL AND MORAL ASPECTS
According to Resolution No. 466/2012 of the National Health Council, since it is a question of research involving human beings, the present study was submitted to the Ethics and Research Committee, approved under Opinion No. 2,048,685, the confidentiality of the information provided and all Participants received the Informed Consent Term, with the option to withdraw their participation in the research at any time during the data collection. In order to maintain the anonymity of the participants, the interviewees were identified with the letter P and a number.
DATA ANALYSIS AND DISCUSSION
Data analysis was performed using the Bardin Content Analysis Technique (2006) and consisted of three phases:
In the first phase or pre-analysis, the interviews were transcribed, followed by a careful reading with the objective of identifying the meaning of the utterances.
Second phase or exploration of the material comprised the mapping of the answers of each subject to the questions, followed by the grouping of the data where four categories were found from the questions of the research instrument. The categories evidenced were: Knowledge of the users about the relationship between Chronic Kidney Disease and Diabetes Mellitus; Occurrence and characterization of chronic Chronic Kidney Disease in the participants; Estimation of the time between the diagnosis of DM of the users and the beginning of the HD therapy; Realization of guidelines by the staff of the service to users, especially by the Nursing Team and Adhesion of the users received guidelines.
In the third phase or treatment of the results and interpretation, an individualized evaluation of the responses was performed, the following subcategories being evidenced: I think not, Yes, No, Hypertension, Diabetes, Cardiopathy, Cancer, Bronchitis, Neurogenic Bladder, Medication, Liquids, Physical Activity.
CHARACTERIZATION OF STUDY PARTICIPANTS
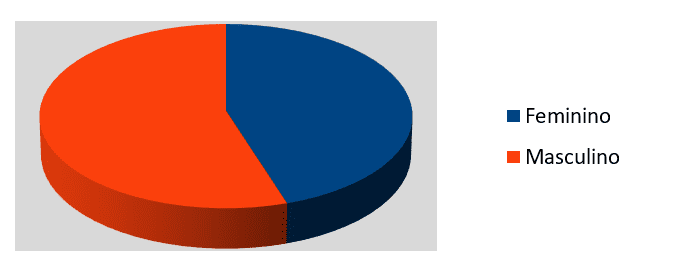
The information collected refers to 20 users who authorized participation in the study by signing a Free and Informed Consent Form, of which 11 were male (55%) and 9 were female (45%), as shown in the Graphic 1. A study conducted in Bahia by Almeida, Alves e Silva (2012) found a similar result, with a 56.6% prevalence for males.
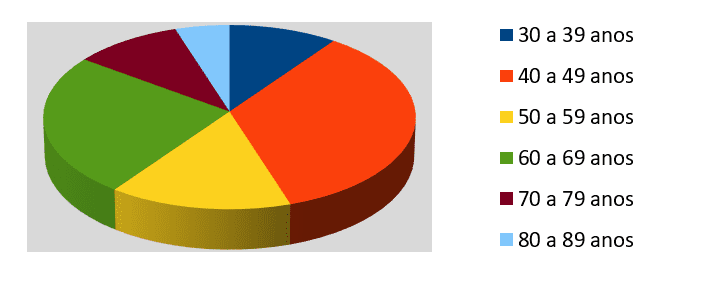
The age group of the participants was between 30 and 89 years of age as shown in figure 2. For better elaboration of the graph, the ages were arranged in six intervals. The first one ranged from 30 to 39 years and counted 2 people, the second 40 to 49 years 7 people, the third from 50 to 59 years 3 people, from 60 to 69 years 5 people, from 70 to 79 years 2 people and from 80 to 89 years old 1 person.
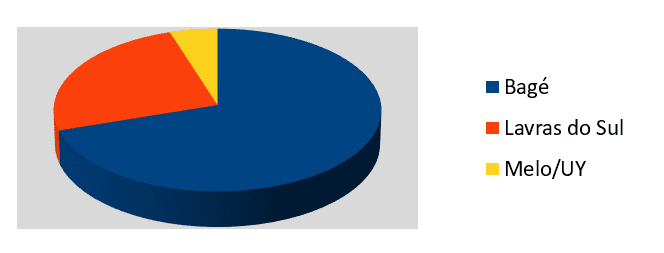
The Hemodialysis Service in Bagé in which the research was carried out is a reference in Nephrology for the Municipalities covered by the 7th Regional Health Coordination, for this reason it is provided service to users of different cities, as shown in Chart 3. During the interviews, 14 clients residing in the Municipalities of Bagé, 05 residing in the Municipality of Lavras do Sul and a user from the City of Melo / Uruguay were receiving care.
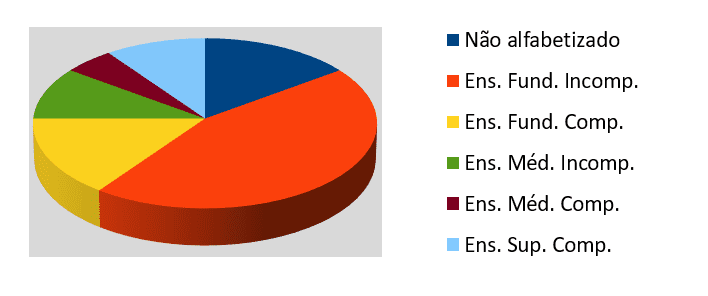
As for the level of schooling of users who participated in the study, three were not literate, 9 did not complete Elementary School, three reported having completed Elementary School, two said they did not complete High School, one user reported having completed High School and higher education, as can be seen in Graph 4.
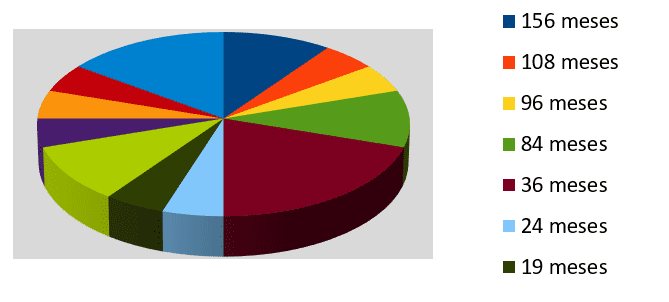
Because it is a chronic pathology, renal disease requires continuous treatment, and when it advances to the final stage there are two options of treatments to be performed, renal transplantation and renal replacement therapy. The mean length of stay on hemodialysis of the study participants is 45.75 months, covering patients who started the treatment two months ago and others who have already performed the procedure 156 months, as shown in figure 5.
DISCUSSION OF THE DATA
Because it was a qualitative study, the results were listed in categories, about users' knowledge about the relationship between Chronic Kidney Disease and Diabetes Mellitus, the objective was to verify if the users of the service believed that CRD may be related to DM, and it was observed that some participants (50%) believe that there is no relationship between Chronic Kidney Disease and Diabetes Mellitus, as evidenced in the speeches:
– "I think it's unrelated because I'm not diabetic." (P06)
"I do not think so." (P01, P03, P10, P13, P15)
– "I believe it has nothing to do." (P17)
With the information, it is evident that a large proportion of those attending the Health Unit do not relate DM to the DRC, although data from the Brazilian Chronic Dialysis Survey of 2014 point to high blood pressure and diabetes as the main diseases that lead the patient to chronic renal insufficiency requiring dialysis in Brazil. These data are superior to those of other countries in Europe and North America, confirming these diseases as the main reasons that lead the patient to require hemodialysis or peritoneal dialysis (SESSO et. al, 2014).
In addition, it is known that chronic renal failure results from the progressive and irreversible loss of large numbers of nephrons, and the causes may be diverse, among which are hypertension, renal vascular disorders, immunological disorders, infections, obstructions the urinary tract, congenital disorders and metabolic disorders such as Diabetes Mellitus and Obesity (GUYTON AND HALL, 2011).
Among the users who expressed knowledge about the relationship between diabetes mellitus and chronic kidney disease, the following statements stand out:
– "I think so, I think not, I'm sure so." (P7)
– "I do not have this problem, but I think so." (P8)
– "Certainly." (P16)
What demonstrates that Diabetes Mellitus is considered relevant by some users as a cause of Chronic Renal Disease, it is important to emphasize health education through proper guidance, providing better adherence to treatments, making it possible to obtain more satisfactory results and lasting, decreasing the incidence of chronic kidney diseases (LOUREIRO et. al, 2011). For this process of health education, although it does not re-establish the renal function of the patients, it is possible to use the nephrology service as an auxiliary in the process, taking into account that the daily therapy time is long, which would favor the process, in addition, it is taken into account that the patient who already suffers from the consequences of renal replacement therapy, has the capacity to externalize his experiences, in the vast majority of cases.
Hypertension and Diabetes Mellitus were cited by half of the interviewees, with systemic arterial hypertension previously diagnosed as CKD in 6 users (30%), type II diabetes mellitus in 2 users (in the category of occurrence and characterization of previous CKD 10%) and, when associated with SAH and Type II DM present in 2 patients (10%), one participant reported having neurogenic bladder (5%), 5 users said they did not know about any previous CKD pathology (25%) and 4 20%) reported having diagnosed other pathologies such as myopia, cancer, bronchitis, heart problems and alterations of the spine, highlighting the following speeches:
– "I have lung cancer, I had another cancer of the pelvic region, no connection between the two, in six months. I have a saphenous bridge. "(P7)
– "I am hypertensive, I have heart disease, diabetes and a back problem." (P4)
– "I have vision, high blood pressure." (P9)
– "I have the heart and the pressure." (P13)
– "In fact my kidney disease came from the bladder, I have neurogenic bladder, so I do not empty my bladder completely, I should do catheterization three to four times a day and it is very difficult to probe me, so I relaxed and there . "(P17)
A similar study by Oliveira, Formiga and Alexandre (2014) showed that hypertension was the etiology of CKD in 38% of cases and diabetes mellitus in 13%, and in 10% of the patients, these two diseases were found to be concomitant causes and , 28% had unknown etiologies for CKD.
According to Bastos, Bregman and Kirsztajn (2010) there are users who are more susceptible to CKD due to pathologies that are considered predisposing as cardiovascular diseases, since these are associated with a decrease in the glomerular filtration rate. Hypertension, for example, is commonly associated with chronic kidney disease. Users with a family history of chronic kidney disease have an increased prevalence of hypertension, diabetes mellitus, proteinuria, and renal disease. In addition, users diagnosed with diabetes mellitus are at increased risk for CKD and cardiovascular disease, so they are included in risk groups.
In the category that sought to estimate the time between the diagnosis of DM of the users and the beginning of the HD therapy, it was evidenced that the mean time span between the initial diagnosis of Diabetes Mellitus in the four users and the beginning of the hemodialysis therapy was 5 years and medium, ranging from 2 to 8 years.
The Brazilian Society of Diabetes (2016) directs that the screening for diabetes renal disease be initiated soon after the diagnosis of type II DM and after five years of diagnosis of type I DM, except in patients diagnosed at puberty or with decompensation of recurrent DM , as they should follow up independently of these indications. It is also recommended that this screening be annual, checking Glomerular Filtration Rate and albuminuria dosage.
This is necessary in view of the fact that, according to Brazil (2013), uncontrolled diabetes can cause dysfunction and failure in several organs in the long term, with the most affected being nerves, eyes, heart, blood vessels and kidneys. Increased mortality and development of micro and macrovascular lesions are also associated with diabetes, and thus, diabetes mellitus is considered a cause of blindness, renal insufficiency and limb amputations, considerably increasing health spending and reducing work capacity, and life expectancy of the population.
Identifying individuals with CKD, especially in the early stages, favors interventions, either those that delay or potentially prevent disease progression through the implementation of educational activities, aiming at motivating and adhering patients to their disease. This screening work can be performed in a variety of ways, ranging from simple methods such as the use of questionnaires and estimation of GFR from serum creatinine, to more complex strategies using sociodemographic data, physical examination, and laboratory tests. blood and urine, in high-risk patients and in the general population (MAGACHO et. al, 2012).
Chronic kidney disease sometimes does not present symptomatology in its initial stage, because being a slow progression pathology the organism can adapt to the new situation, which leads to the manifestation of symptoms when there is already severe kidney involvement in most cases ( HOSPITAL ISRAELITA ALBERT EINSTEIN, 2012). A study carried out by Moreira, Gomes and Santos (2010) showed that the late diagnosis of hypertension and hypertension often occurs, often diagnosed with associated complications, referring to the complexity of supply and access to health services.
With this, it can be inferred that the diagnosis performed in the participants was not carried out in a time close to the occurrence of the disease, and the organism may have suffered initial damage to the glycemic decompensations.
In the category of guidelines provided by the service team to users, it was intended to investigate which orientations the patients of the service received from the team during the service, especially those provided by the nursing team. When questioned about which guidelines were received, a large part of the interviewees reported receiving information during the hemodialysis sessions and consultations, from the medical, nursing and nutritionist staff, this information covers issues such as feeding, medication, fluid intake, appropriate treatment and physical activity as well as fistula care, as evidenced by the following statements:
– "They say there is no cure, they have to treat three times a week, and also take care of food and liquids. "(P1)
– "They tell us not to drink too much liquid, to take 500ml of water, to feed without salt and without fat, and to do physical exercise. "(P2)
– "That you have to take care of yourself, that you have to take medicine. "(P6)
– "All possible, the precautions, given here by them, which by the way is a wonderful place. "(P7)
– "It says how we should take care, how we should eat, how we should drink water, they explain why the people 's kidney stops working. "(P13)
"Oh, all we have to do is watch out for food, what you can take, and the medications. "(P17)
A study by Gricio, Kusumota and Candido (2009) concluded that patients with chronic renal disease in conservative treatment, in most cases, have insufficient information about the disease and treatments, which can cause negative interference in adherence to the treatment instituted and , thereby accelerating the progression of the disease. The need to construct an educative approach as a strategy to stimulate patients to adhere to the treatment, leading to the reduction of early morbidity and mortality during the dialysis treatment, is then perceived.
Pacheco, Santos and Bregman (2010) believe that clients need to be aware of their potential for self-care, assuming that people are not completely sick, and there is a healthy core within them. These subjects should be encouraged to lose the notion of passivity, becoming protagonists of their own care, this is an act of citizenship.
In the category of user adherence to the guidelines received, it was analyzed the care taken by the users based on the guidelines provided, and it was possible to notice that although they have been in treatment for a considerable period of time, only half of the participants said follow the guidelines received , nine stated that they did not perform the care according to orientation and one of them reported that they are trying to perform only one part. Of those who follow the guidelines, it became clear that food is the main concern, followed by fluid intake and medications, as seen in the speeches that follow:
– "I take care of the diet, not as a heavy thing, I control the liquids, I take a little liquid." (P1)
– "I try to follow all, what I can usually eat and the remedies." (P4)
– "I try to do all, I try to follow the guidance to the letter." (P7)
– "I take care of everything I can with food and medicines." (P10)
– "That he can not drink much liquid, that he has to control the feed because of sodium and potassium." (P14)
Canhestro et. al (2010) suggest the need for a reassessment of the strategies used in educational activities, adapted to the age and cognitive development of each patient and life experiences, with proposals for activities that involve the active participation of patients and their families, aiming to make them constructors of the own knowledge and, consequently, to lead them to better adherence to the treatment.
The major challenge of nursing when it comes to the health of the elderly is to insert it in the process of health promotion, making it understand and have access to information about the policies in relation to them in a clear and objective way (CANEPA, CARDOSO and RICARDINO, 2014).
The teaching of self-care, therefore, should value the knowledge, the voices, the culture and the forces of struggle for the life of the people, leading them to their autonomy in questions of well-being and well-being (PACHECO, SANTOS and BREGMAN, 2007 ).
FINAL CONSIDERATIONS
Based on this study, it is evidenced that the nephrology service users are mostly adults and elderly, and when patients with diabetes mellitus, are type II, this way it is necessary the screening of comorbidities as recommended in the protocols of health, always from the diagnosis of DM, being repeated annually.
This screening work in the risk population when carried out together with the health education process may help to reduce the evolution of chronic diseases, leading to an improvement in the quality of life of patients with these diseases, since there is no better way of treatment which is aimed at maintaining health and reducing injuries.
It is also evident that health information when isolated is not sufficient for users to adhere to the recommended treatments, and these should be targeted on the diseases that may still arise, since although they are already being treated in a specialized health unit the habits of life and are of paramount importance to slow the progression of chronic kidney disease.
Nursing care must be carried out in a planned manner, taking into account the problems identified in each users and the level of care that is necessary for their care, so it is important to develop strategies that favor therapeutic communication and management of quality, for this it is necessary that the interpersonal relationship and the communication between team and users be carried out in an effective and clear way, according to the cognitive capacity of each client.
Through the results found, it is possible to note the relevance and necessity of the implementation of care that aims at the promotion of health education aimed at the users' knowledge about the complications of their disease, providing a continuity of health care assistance with knowledge, in order to promote self-care and increase the quality of life of this population.
At the end of the study, it is considered that the objectives were achieved, since there were occurrences of users who had diabetes mellitus diagnosed as a chronic kidney disease, the participants were receptive and collaborative for the accomplishment of the present study, to questions about adherence to the guidelines received. As final objective, this work will be sent to the nephrology service, in order to expose the results and possible elaboration of strategies that assist in the treatment of the assisted ones.
REFERENCES
ALMEIDA, A. B .; ALVES, V. F .; SILVA, D. C. S .. Quality of life of the chronic renal patient on hemodialysis. 2012. Available at: <http://www.libertas.edu.br/revistas/index.php/riclibertas/article/view/23/15> Last access on: November 24, 2016.
BARDIN, L .. Content analysis (L. de A. Rego & A. Pinheiro, Trads.). Lisbon: Editions 70, 2006.
BASTOS, M. G .; BERGMAN, R .; KIRSZTAJN, G. M .. Chronic kidney disease: frequent and severe, as well as preventable and treatable. Revista Médica Brasileira. 2010 Available at: <http://www.scielo.br/pdf/ramb/v56n2/a28v56n2> Last access on: November 18, 2016.
BRAZIL. Ministry of Health. Secretariat of Health Care. Department of Basic Attention. Strategies for care of the person with chronic disease: diabetes mellitus. Brasília: Ministry of Health, 2013.
CANEPA, E. B. S .; CARDOSO, A. I. Q .; RICARDINO, A. R .. The nurse and the promotion of quality of life for the elderly: a review. 2014. Available at: <www.unigran.br/interbio/paginas/ed_anteriores/vol8_num1/arquivos/artigo6.pdf> Last access on: June 16, 2017.
CANHESTRO, M. R .; OLIVEIRA, E. A .; SOARES, C. M. B .; MARCIANO, R. C .; ASSUNÇÃO, D. C .; GAZZINELLI, A .. Knowledge of patients and relatives about chronic kidney disease and its conservative treatment. 2010 Available at: <www.reme.org.br/artigo/detalhes/124> Last access on: June 12, 2017.
FORTIN, M. F .. Foundations and stages of the investigation process. Loures: Lusodidacta, 2009.
GRICIO, T. C .; KUSUMOTA, L .; CÂNDIDO, M. L .. 2009. Perceptions and knowledge of patients with Chronic Renal Disease in conservative treatment. Available at: <https://www.fen.ufg.br/fen_revista/v11/n4/pdf/v11n4a14.pdf> Last access on: June 12, 2017.
GUYTON, A. C .; HALL, J. E. Treatise on medical physiology. 12th edition. Rio de Janeiro: Editora ELSEVIER, 2011. (p329-433; p987-1003)
ISRAELI HOSPITAL ALBERT EINSTEIN. Chronic Renal Disease. 2012. Available at: <https://www.einstein.br/doencas-sintomas/doenca-renal-cronica> Last access on: September 22, 2016.
LOUREIRO, F. M .; BARBOSA, L. S .; REBELLO, L. C .; VIEIRA, S.A .; BELINELO, V. J.; PROFILE OF PATIENTS WITH CHRONIC RENAL INSUFFICIENCY, AT THE HEMODIALYSIS UNIT OF LINHARES – ES. 2011. ENCYCLOPEDIA BIOSFERA, Centro Científico Conhecer – Goiânia, vol.7, N.13; 2011. Available at: <http://www.conhecer.org.br/enciclop/2011b/ciencias%20da%20saude/perfil%20de%20pacientes.pdf> Last access on: June 12, 2017.
MAGACHO, E.J. C .; ANDRADE, L. C. F .; COSTAS, T. J. F .; PAULA, E.A .; ARAÚJO, S. S .; PINTO, M. A .; BASTOS, M. G .. Translation, cultural adaptation and validation of the Screening For Occult Renal Disease (SCORED) questionnaire for Brazilian Portuguese. 2012. Available at: <www.jbn.org.br/details/1480/en/traducao-adaptacao-cultural-e-validacao-do-questionario-rastreamento-da-doena-renal-oculta–screening-for- occult-renal-disease — scored-for-the-port> Last accessed on: June 12, 2017.
MINAYO, M. C. S .. Social Research. Theory, method and creativity. 18 ed. Petrópolis: Vozes, 2001.
MOREIRA, T. M. M .; GOMES, E. B .; SANTOS, J. C .. Cardiovascular risk factors in young adults with hypertension and / or diabetes mellitus. 2010 Available at: <https://www.researchgate.net/profile/Thereza_Maria_Moreira/publication/266178171_FATORES_DE_RISCO_CARDIOVASCULARES_EM_ADULTOS_JOVENS_COM_HIPERTENSAO_ARTERIAL_EOU_DIABETES_MELLITUS_a/links/54d370540cf2b0c6146d887d.pdf Last accessed on: June 12, 2017.
NETTINA, S. M .. Nursing Practice. Rio de Janeiro: Guanabara Koogan, 2011. Volume 2. (p.781-786; p919-944)
OLIVEIRA, H. M., FORMIGA, F.F.C., ALEXANDRE, C. S .; Clinical-epidemiological profile of patients in a chronic hemodialysis program in João Pessoa – PB. J Bras Nefrol 2014; 36 (3): 367-374. Available at: <www.scielo.br/pdf/jbn/v36n3/0101-2800-jbn-36-03-0367.pdf>. Last access on: June 12, 2017.
WORLD HEALTH ORGANIZATION. Global report on diabetes. Available at: <http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf?ua=1> Last access on: September 22, 2016.
PACHECO, G. S .; SANTOS, I .; BREGMAN, R .; Nursing Evaluation About Patients With Chronic Kidney Disease: Competence for Self Care. 2007. Available at: <https://www.researchgate.net/profile/Rachel_Bregman/publication/49943656_Clientes_com_doenca_renal_cronica_avaliacao_de_Enfermagem_sobre_a_competencia_para_o_autocuidado/links/00b7d5208e7d4d300a000000.pdf> Last access on: June 16, 2017.
SESSO, R.C. C .; LOPES, A. A .; THOMÉ, F. S .; LUGON, J.R .; WATANABE, Y .; SANTOS, D. N .; MARTINS, C. T .; Brazilian Dialysis Inquiry. 2014. Available at: <http://www.scielo.br/pdf/jbn/v38n1/0101-2800-jbn-38-01-0054.pdf> Accessed on: June 13, 2017.
BRAZILIAN DIABETES SOCIETY. Guidelines of the Brazilian Diabetes Society: 2014-2015 / Brazilian Society of Diabetes; [organização José Egídio Paulo de Oliveira, Sérgio Vencio]. – São Paulo: AC Pharmaceuticals, 2015.
BRAZILIAN DIABETES SOCIETY. Guidelines of the Brazilian Diabetes Society (2015-2016) / [organização José Egidio Paulo de Oliveira, Sérgio Vencio]- São Paulo: A.C. Farmacêutica, 2016.
[1] Academic of the 8th semester of the Nursing course of the University of the Region of the Campaign – URCAMP. Bagé / RS.
[2] Advisor, Nurse, Master and Professor of the Nursing course of the University of the Region of the Campaign – URCAMP. Bagé / RS.















