ORIGINAL ARTICLE
ROCHA, Karina Dias [1], FECURY, Amanda Alves [2], OLIVEIRA, Euzébio [3], DENDASCK, Carla Viana [4], DIAS, Cláudio Alberto Gellis de Mattos [5]
ROCHA, Karina Dias. Et al. Number of congenital syphilis cases in Brazil between 2009 and 2013. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 05, Ed. 05, Vol. 01, pp. 131-143. May 2020. ISSN:2448-0959, Access link in: https://www.nucleodoconhecimento.com.br/health/congenital-syphilis-cases, DOI: 10.32749/nucleodoconhecimento.com.br/health/congenital-syphilis-cases
ABSTRACT
Syphilis is a disease caused by the bacterium Treponema pallidum. Congenital syphilis is a contagious disease transmitted from the mother to the fetus. The objective of this work is to show the number of cases of congenital syphilis in Brazil between the years 2009 to 2013. The research was carried out in the DATASUS database[6]. The number of cases of congenital syphilis increased between 2009 and 2013 and the southeastern region had the highest national average in this period. females had a higher number of cases than males and most cases were diagnosed in the age group of up to six days of life. An average of three times as many women received prenatal care as those who did not. Women with a maternal school grade from the 5th to the 8th incomplete grade of elementary school had a higher number of syphilis cases. A greater number of treatments of the mother is perceived in the year 2012. In Brazil, despite the high performance of prenatal care, most cases of congenital syphilis were diagnosed only after delivery, showing errors in the diagnosis of the disease during the performance examination and resulting in late treatments. Education and income are factors that seem to influence the diagnosis and treatment of the disease. It seems necessary to increase the number of treatment partners, thus reducing the transmission of syphilis and consequently that of congenital syphilis. The treatment performed in most cases seems to guarantee the cure of the disease.
Keywords: Congenital syphilis, epidemiology Brazil.
INTRODUCTION
Syphilis is a disease caused by the bacterium Treponema pallidum (SONDA et al., 2013). It can be transmitted mainly through sexual contact. Contamination by blood transfusion, contact with mucocutaneous tissue and through the placenta can also occur (SANTOS and ANJOS, 2009).
classified into primary, secondary and tertiary. In the first stage, the symptoms are lesions at the contamination site, with no clinical manifestations at the extremities. In the second stage, symptoms can be headache, malaise, bone pain, rash on the face and body, and the symptom of the first stage may still be present. In the third stage, symptoms can be neurosyphilis, psychosis, stroke and partial loss of movement, reaching other organs of the body (SANTOS and ANJOS, 2009). Treatment for all stages is carried out with the use of penicillin and must extend to sexual partners (SONDA et al., 2013).
Congenital syphilis is the contagious disease caused by the bacterium Treponema pallidum, when transmitted from the mother to the fetus via the placenta. (PIRES et al., 2014).
Treatment for congenital syphilis is performed using intravenous crystalline penicillin G. There is a variation in doses according to age, with mothers inadequately treated or mothers treated with newborns who present negative syphilis test (SONDA et al., 2013).
In Brazil, in 2013, there were 13,705 cases of congenital syphilis, of which 4,417 in the Northeast, 1064 in the North, 5,907 in the Southeast, 1,566 in the South and 751 in the Midwest. In the same year in the state of Amapá, there were 98 cases of congenital syphilis (BRASIL, 2016).
AIM
Show the number of cases of congenital syphilis in Brazil between the years 2009 to 2013.
METHOD
The research was carried out in the DATASUS database[7]. National data were collected according to the following steps: A) the link[8] was accessed, clicked on “epidemiological and morbidity”. On the open page, “Diseases and Diseases of Notification – 2007 onwards (SINAN)”. On the next page, “Congenital syphilis” was selected. In the “geographic scope” box, “Brazil by region, state, and municipality” was chosen. From there, the steps were followed: A) In line, “Diagnostic Year” was selected, in the “not active” column and in the content “confirmed cases”. All data, in this and the next steps, were collected between the years 2009 and 2013. B) In the row, “Region of Notification” was selected, in the column “Not Active” and in the content “confirmed cases”; C) in the line, “Age group” was selected, in the “not active” column and in the content “confirmed cases”; D) In the line, select “Prenatal care”, in the column select “not active”, in the content select “confirmed cases”; E) In the row select “Maternal Syphilis”, in the column select “not active”, in the content, select “confirmed cases”; F) In the row, select “Diagnostic Year”, in the column, select “gender”, in the content, select “confirmed cases”. The data was compiled using the Excel application, part of the Microsoft Corporation Office suite. The bibliographic research was carried out in scientific articles, using computers from the computer lab of the Federal Institute of Education, Science and Technology of Amapá, Campus Macapá, located at: Rodovia BR 210 KM 3, s / n – Bairro Brasil Novo . CEP: 68.909-398, Macapá, Amapá, Brazil.
RESULTS
Figure 1 shows the percentage of confirmed cases of congenital syphilis in Brazil between the years 2009 to 2013. The graph shows an increase between the years 2009 and 2012, with a significant decrease in the year 2013.
Figure 1 Shows the percentage of confirmed cases of congenital syphilis in Brazil between 2009 and 2013.
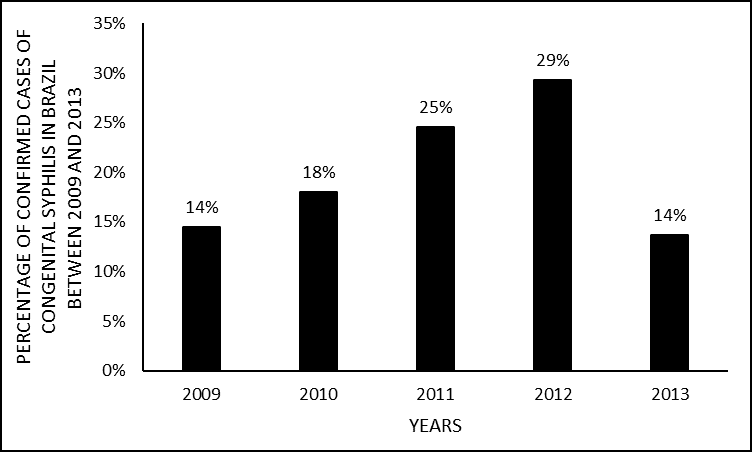
Figure 2 shows the percentage of cases of congenital syphilis by regions of Brazil between the years 2009 and 2013. The southeast region had the highest national number in this period, followed by the northeast region. The lowest results were from the south, north and central-west regions, respectively.
Figure 2 Shows the percentage of cases of congenital syphilis by regions of Brazil between 2009 and 2013.
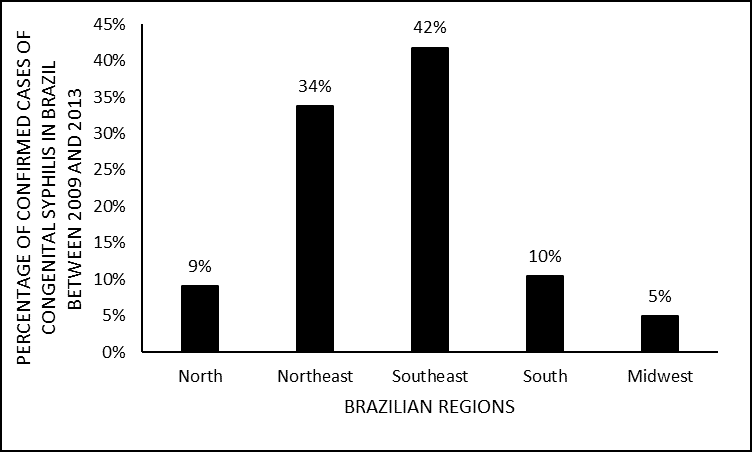
Figure 3 shows the percentage of cases of congenital syphilis by gender in Brazil, between the years 2009 and 2013. The data show a slightly higher number of cases among females than males.
Figure 3 Shows the percentage of cases of congenital syphilis by gender in Brazil between 2009 and 2013.

Figure 4 shows the percentage of confirmed cases of congenital syphilis by age group in Brazil between the years 2009 and 2013. The graph shows a greater number of cases in the age group of up to six days of life.
Figure 4 Shows the percentage of cases of congenital syphilis by age group in Brazil between 2009 and 2013.
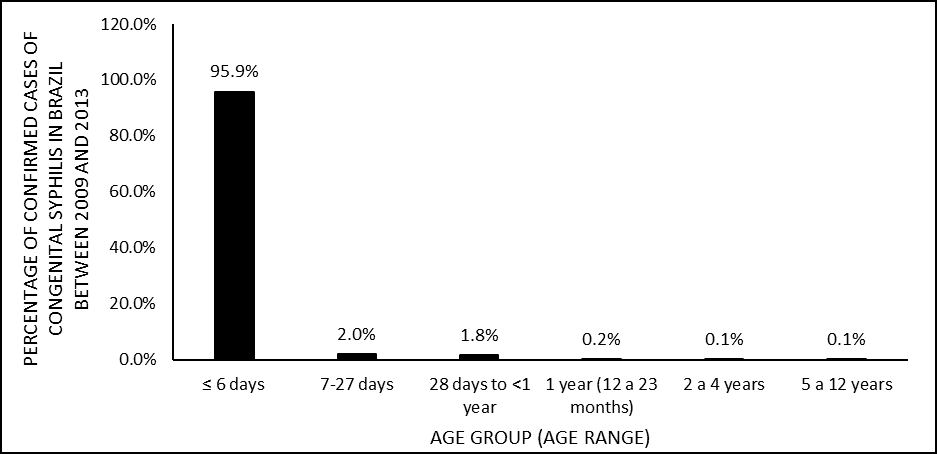
Figure 5 shows the percentage of confirmed cases of congenital syphilis in Brazil due to prenatal exams between the years 2009 and 2013. The data shows a higher percentage of women who have had prenatal care (prenatal examination) than those who have not.
Figure 5 Shows the percentage of confirmed cases of congenital syphilis in Brazil due to prenatal examination (prenatal care) between 2009 and 2013.

Figure 6 shows the percentage of confirmed cases of congenital syphilis in Brazil by the time of maternal syphilis infection, between the years 2009 and 2013. A greater number of infections is noticed during the prenatal examination and also at the time of childbirth.
Figure 6 Shows the percentage of confirmed cases of congenital syphilis in Brazil by the time of maternal syphilis infection, between the years 2009 and 2013.

Figure 7 shows the percentage of confirmed cases of congenital syphilis in Brazil by the mother’s level of education between the years 2009 and 2013. The data shows a greater number of cases with the maternal level of school from the 5th to the 8th grade of incomplete elementary school, and the lowest number with complete higher education.
Figure 7 Shows the percentage of confirmed cases of congenital syphilis in Brazil by the mother’s education level between 2009 and 2013
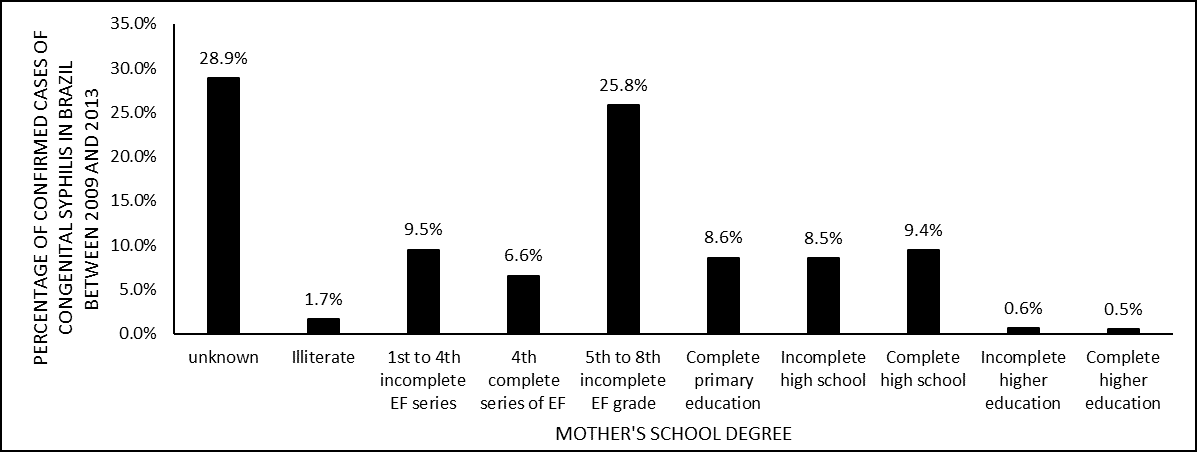
Figure 8 shows the percentage of confirmed cases of congenital syphilis in Brazil by ethnicity (race) between the years 2009 and 2013. The mixed race had the highest number of cases, followed by the white one. The ethnicities with the lowest number were black, indigenous and yellow, respectively.
Figure 8 Shows the percentage of confirmed cases of congenital syphilis in Brazil by ethnicity (race) between the years 2009 and 2013.
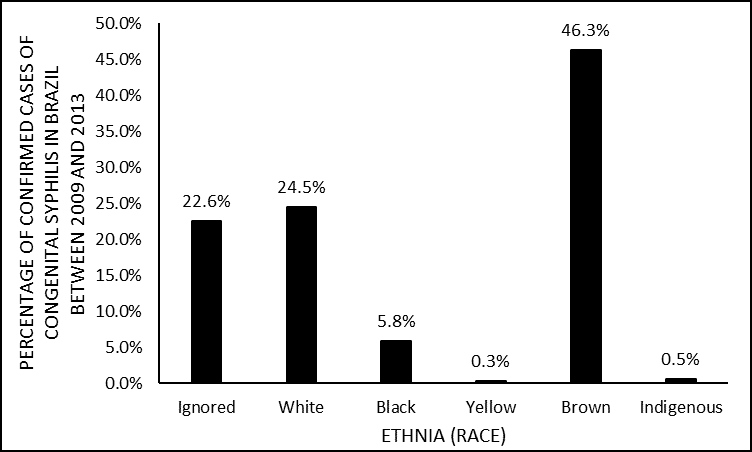
Figure 9 shows the percentage of confirmed cases of congenital syphilis in Brazil by the year the mother started treatment between 2009 and 2013. A greater number of treatments for the mother is perceived in 2012, followed by 2011 The year 2013 had the lowest number, followed by the year 2009 and 2010.
Figure 9 Shows the percentage of confirmed cases of congenital syphilis in Brazil by the year the mother started treatment between 2009 and 2013.

Figure 10 shows the percentage of confirmed cases of congenital syphilis by treatment of the partner between the years 2009 and 2013. The data shows a greater number of men who did not undergo treatment than those who did not.
Figure 10 Shows the percentage of confirmed cases of congenital syphilis by treatment of the partner between the years 2009 and 2013.
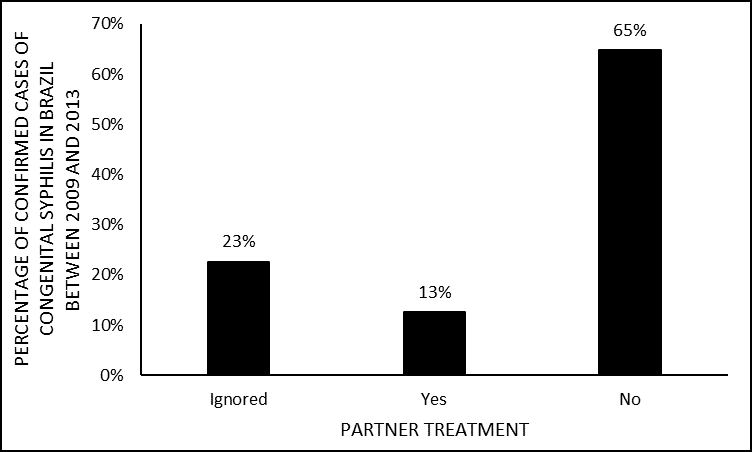
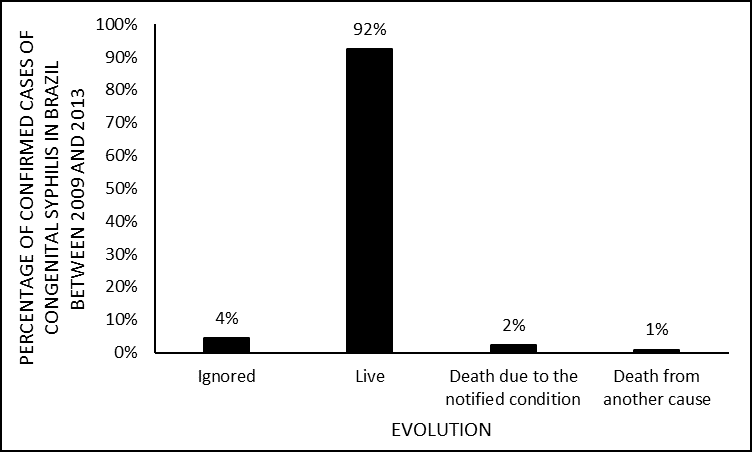
Figure 11 shows the percentage of confirmed cases of congenital syphilis in Brazil due to evolution between 2009 and 2013. In the graph, there is a significantly higher number of people alive than deaths due to the notified disease or other cause.
Figure 11 Shows the percentage of confirmed cases of congenital syphilis in Brazil by evolution between 2009 and 2013.
DISCUSSION
The data show an increase between the years 2009 and 2013, with a significant decrease occurring in the year 2013 (figure 1). Probably the cause was the campaign launched by the Public Ministry in 2013, which encouraged the diagnosis of the disease during prenatal care, in addition to increasing the offer of tests for the diagnosis of syphilis from 31,500 in 2011 to around 1, 7 million in 2013. The increase in the number of confirmed cases of congenital syphilis between 2009 and 2012, can be explained by the growth in the number of notifying health units, allowing access to exams and testing, and allowing several cases to enter the records (BRASIL, 2014; 2017).
Between 2009 and 2013, the southeastern region of Brazil had the highest number of cases of congenital syphilis (figure 2). Probably, the cause is the large population of the region, which, according to IBGE, has about 80 million inhabitants, being the most populous region in the country. This can cause a greater number of unprotected sex, in addition to increasing the risk of transmission through mucocutaneous tissue and blood transfusion, thus affecting pregnant women who transmit the disease to the fetus (GUIMARÃES et al., 2015).
Between 2009 and 2013, about 52% of cases of congenital syphilis were diagnosed in females (figure 3). The fact of not having a fixed sexual partner, associated with not using a condom, justified in most cases by the trust in sexual partners, explains the disease affecting women more (MENESES et al., 2017; MOREIRA et al., 2017).
Between 2009 and 2013 the largest number of cases of congenital syphilis was diagnosed in the age group of up to 6 days of life (figure 4). There seems to be a failure to perform prenatal care or a failure to diagnose the disease during the examination that causes congenital syphilis to be diagnosed only after delivery. The child who presents symptoms soon after birth forces exams and tests to diagnose the disease (DOMINGUES et al., 2013).
Between 2009 and 2013, 74% of pregnant women underwent prenatal care (figure 5). Probably the cause is the federal government’s incentive to basic health care, thus increasing the coverage of prenatal care. However, it is noted that this assistance was of low quality resulting in errors in the diagnosis of congenital syphilis at the time of the examination (PEDRAZA, 2016).
A higher percentage of confirmed cases of congenital syphilis due to maternal syphilis in Brazil seems to be detected in the prenatal examination and the moment of delivery (figure 6). Economic inequality in Brazil means that a majority of pregnant women undergo a precarious prenatal examination that can result in errors in diagnosis and not detect the disease. Because of this, cases of congenital syphilis were diagnosed during the examination and most cases were detected at the time of delivery (SANTOS et al., 2016).
During the research period, the data show a greater number of cases in people with lower education (figure 7). Probably pregnant women with low schooling tend not to perform prenatal care, as they do not have access to, ignore, or devalue its importance. This fact seems to make treatment impossible during pregnancy (SANTOS et al., 2016).
In Brazil, self-declaration of race is guaranteed by law (CRUZ, 2016). Between 2009 and 2013, the mixed race had the highest number of registered cases (figure 8). Probably the mixture of races resulting from the colonization of the country resulted in a population where a large part of the people declare themselves to be brown (MOREIRA et al., 2017).
Between 2009 and 2012, there was an increase in the number of treatments for the mother, with a significant drop in 2013. The reduction in the number of confirmed cases of congenital syphilis may have happened as a result of the campaign carried out by the Public Ministry that encouraged the diagnosis of disease during pregnancy (BRASIL, 2017).
In the country, between 2009 and 2013, 65% of the sexual partners of women diagnosed with syphilis during pregnancy did not undergo treatment for the disease (figure 10). The reasons are probably the lack of knowledge about the disease and its consequences, as well as cultural association diagnosis of syphilis to infidelity (FIGUEIREDO et al., 2015).
Research shows a large percentage of living in relation to the deaths notified grievance and others. Between 2009 and 2013, about 92% of cases of congenital syphilis survived the disease and 2% died. Possibly the treatment performed in the registered cases seems to guarantee the cure of the condition (MOREIRA et al., 2017).
CONCLUSION
In Brazil, despite the high performance of prenatal care, most cases of congenital syphilis were diagnosed only after delivery, showing errors in the diagnosis of the disease during the exam and resulting in late treatments. Education and income are factors that seem to influence the diagnosis and treatment of the disease. It seems necessary to increase the number of treatment partners, thus reducing the transmission of syphilis and consequently that of congenital syphilis. The treatment performed in most cases seems to guarantee the cure of the disease.
REFERÊNCIAS
BRASIL. Boletim Epidemiológico de DST/Aids. Brasília DF: Ministério da Saúde, 2014. 84p.
______. Sífilis 2016. Brasilia DF: Ministério da Saúde: 29 p. 2016.
______. Ministério da Saúde Lança Campanha de Combate à Sífilis. Brasilia DF, 2017. Disponível em: < http://www.brasil.gov.br/saude/2013/10/ministerio-da-saude-lanca-campanha-de-combate-a-sifilis >. Acesso em: 26 set 2017.
CRUZ, I. C. F. Notas sobre prevenção da fraude – autodeclaração sobre raça/cor. Boletim NEPAE-NESEN, v. 13, n. 1, p. 1-4, 2016.
DOMINGUES, R. M. S. M. et al. Sífilis congênita: evento Sentinela da qualidade da Assistência pré-natal. Revista Saúde Pública, v. 47, n. 1, p. 147-157, 2013.
FIGUEIREDO, M. S. N. et al. Percepção de enfermeiros sobre a adesão ao tratamento dos parceiros de gestantes com sífilis. Revista Rene, v. 16, n. 3, p. 345-354, 2015.
GUIMARÃES, R. M. et al. Diferenças regionais na transição da mortalidade por doenças cardiovasculares no Brasil, 1980 a 2012. Revista Panamericana de Salud Pública, v. 37, n. 2, p. 83–89, 2015.
MENESES, M. O. et al. O Perfil do Comportamento Sexual de Risco de Mulheres Soropositivas para Sífilis. Revista de Enfermagem, v. 11, n. 4, p. 1584-1594, 2017.
MOREIRA, K. F. A. et al. Perfil dos Casos Notificados de Sífilis Congênita Cogitare Enfermagem, v. 22, n. 2, p. 1-10, 2017.
PEDRAZA, D. F. Assistência ao pré-natal, parto e pós-parto no município de Campina grande, Paraíba. Cadernos Saúde Coletiva v. 24, n. 4, p. 460-467, 2016.
PIRES, A. C. S. et al. Ocorrência de sífilis congênita e os principais fatores relacionados ao índice transmissão da doença no Brasil da atualidade. Revista Uningá, v. 19, n. 1, p. 58-64, 2014.
SANTOS, G. S. et al. Aspectos Epidemiológicos da sífilis Congênita Associados à Escolaridade Materna. Revista de Enfermagem, v. 10, n. 8, p. 2845-2852, 2016.
SANTOS, V. C.; ANJOS, K. F. Sífilis: Uma realidade prevenível. Sua erradicação, um desafio atual. Revista Saúde e Pesquisa, v. 2, n. 2, p. 257-263, 2009.
SONDA, E. C. et al. Sífilis Congênita: uma revisão da literatura. Revista de Epidemiologia e controle de Infecção, v. 3, n. 1, p. 28-30, 2013.
6. http://datasus.saude.gov.br/
7. http://datasus.saude.gov.br/
8. datasus.gov.br
[1] Mining technician by the Institute of Basic, Technical and Technological Education of Amapá (IFAP).
[2] Biomedical, PhD in Topical Diseases, Professor and researcher of the Medicine Course at Campus Macapá, Federal University of Amapá (UNIFAP).
[3] Biologist, PhD in Topical Diseases, Professor and researcher of the Physical Education Course at, Federal University of Pará (UFPA).
[4] Theologian, PhD in Psychoanalysis, researcher at the Center for Research and Advanced Studies – CEPA.
[5] Biologist, PhD in Theory and Research of Behavior, Professor and researcher of the Chemistry Degree Course at the Basic, Technical and Technological Institute of Amapá (IFAP).
Submitted: May, 2020.
Approved: May, 2020.















