SILVA, Francilene Amorim da [1], ROCHA, Bianca Malheiros Ferreira [2], GESTA, Silvia Sidney Maia [3], FECURY, Amanda Alves [4], DIAS, Cláudio Alberto Gellis de Mattos [5], OLIVEIRA, Euzébio de [6]
SILVA, Francilene Amorim da; et. al. – Serum Epidemiological profile of Dengue cases reported in the city of Belém, Pará – Magazine Multidisciplinary Scientific Knowledge Center. Year 01, Ed. 07, Vol. 04, pp. 75 – 85, July 2016. ISSN:0959-2448
SUMMARY
Dengue is one of the most frequent infectious diseases in Brazil and one of the major public health problems in the world. This study aimed to characterize the serum epidemiological profile of dengue fever in the period 2007 to 2011. The data were obtained from the Department of epidemiological surveillance, the Municipal Health Secretariat in the city of Belém-PA. It was observed that individuals affected by the disease, were females, with 57%, compared to 43% male. The age groups most affected were those observed between individuals from 20 to 39 years (39%) of cases, followed by 40 to 59 years (23%). With regards to dengue serotype 1, 2, 3 and 4, showed that in the period and the region under study, the biggest was for the serotype 4 with 56% of the cases; serotype 1, with 25%; followed by the serotype 2, with 19%. It is believed that the distribution of reported cases of the disease points to the influence of climatic factors, such as precipitation, temperature and humidity, which are favourable to the proliferation and development of Aedes aegypti; Even so, as the lack of public policies and awareness of the population.
Keywords: Dengue fever. Epidemiology. Belém-Pará.
1. INTRODUCTION
Dengue is one of the most frequent infectious diseases in Brazil and one of the major public health problems in the world, mostly in tropical and subtropical regions. It’s a disease endemic and epidemic, which presents clinical picture of early sudden and large, varying the forms of clinical expression, as the form of undifferentiated fever (classical dengue) and severe form (Dengue hemorrhagic fever-FHD), shock (Dengue shock syndrome-SCD) (BRAZIL, 2008b; TORRES, 2008). Dengue fever, in its classic form (“break bone” fever) is a disease with fever (39 C to 40º C), beginning almost always similar to the flu, with generalized malaise and cough followed by headache. Although unpleasant, this form of dengue fever, rarely is inevitable and let a few sequels (LEVINSON, 2005).
Etiologicamente, its causative agent is a virus belonging to the Flaviviridae family and has four serotypes known as dengue 1, 2, 3 and 4 (BRAZIL, 2008 c; TAUIL, 2002). Your transmission is made by the Aedes aegypti mosquito, vector, which, in General, uses artificial containers for vector proliferation, making this species predominantly urban (RAHAMAN et al., 1999; BARRETO; TAMIL, 2008).
This arbovirose reaches the population of all Brazilian States, independent of social class. In 2001, the municipalities of 3,567 27 Brazilian States were infested and transmission have occurred in 24 cities 2,262 of these States. In the year 2007, only the State of Santa Catarina has not presented indigenous transmission (TAUIL, 2002).
According to estimates of the World Health Organization (who), 80,000,000 people are infected each year, with approximately 550,000 hospitalizations and deaths of 20000 (BRAZIL, 2008a).
Of these, approximately 50,000,000 are found in tropical and subtropical regions, taking into consideration that, currently, 2.5 to 3,000,000 people live exposed to the risk of being infected by this arbovirose, where environmental conditions such as temperature and presence of breeding favor the development and proliferation of Aedes aegypti mosquito vector of the disease, primary (BRAZIL, 2008b; TORRES, 2008; MYAZAKI et al. .2009).
The Brazil presented the first epidemic in the early 80, being your first reference in Rio de Janeiro in the 19th century, in the Northeast and in the South (FOCCACIA, 2005).
There are reports of epidemics in Rio de Janeiro in 1946, Niterói in 1923, Curitiba in 1896, Rio Grande do Sul in 1917, Bethlehem in 1967, and the campaign against the Aedes aegypti kept the disease out until 1981 (DONALISIO; GLASSER, 2002). However, the mosquito was detected in several regions, and, in the city of Boa Vista, in 1981, 11000 cases were reported, corresponding to 1/5 of the population of this municipality, being involved in these cases the dengue serotypes 1 and 4 (DONALISIO; GLASSER, 2002; SETUBAL; OLIVEIRA, 2006).
The city of Rio de Janeiro was hit in 1980, 1986 and 1987 for dengue serotype 1. The second outbreak occurred in 1991, with the introduction of dengue serotype 2. The population of this city in 2002, faced the worst epidemic of dengue fever in the country’s history, with 188,073 cases, with the majority by the dengue 3. Increasing the risk of sequential infection deaths and also by the increased virulence of this new strain (DONALISIO; GLASSER, 2002; FOCACCIA, 2005; VITA et al. .2008).
In the North, with the exception of the State of Roraima, the cases have been isolated, from 1995 in the cities of Redemption and Rondon, both in the State of Pará (EVANDRO CHAGAS INSTITUTE, 1997). The city of Bethlehem has today about 1,400,000 inhabitants and its metropolitan region of 2,300,000 inhabitants (IBGE, 2011).
The city of Bethlehem has a hot and humid climate with average annual temperature of 26° C in the hot months. The average maximum temperature reaches 32° C and the minimum average reaches 22 C. The air humidity is approximately 85%, where the rains are not equally throughout the year and offers a higher incidence in the months of January to June (SHARMA et al., 2003). These features are tropical, hot and humid that contribute significantly to greater occurrence of cases of dengue in the region (COSTA, 2005).
METHODOLOGY
The methodology represents the path and the instrumental approach of reality ” including the theoretical concepts and the set of techniques that allow the apprehension of reality and also the creative potential of the researcher “(MINAYO, 2000).
In this sense, the present study was carried out by means of bibliographical research, through books, magazines, and scientific articles related to the topic, seeking to describe the General aspects that involve the dengue virus as well, might make a bibliographical survey on serum epidemiological profile of dengue, the data confirmed notification about virus serotype 1, 2, 3 and 4 , and the characterization by age group and sex, individuals affected by the disease in the city of Belém-PA through analysis of data obtained in organs bound to healthcare.
Obtaining research data occurred in the months of July to September 2012. The data were collected through the reportable diseases information system Notified (SINAN) and Ministry of health (MS) in the city of Belém, in the period from 2007 to 2011, as well as through data provided by the Department of health surveillance of the Municipal Health Secretariat of Bethlehem-SESMA in the same period.
Subsequently, the data obtained from the survey were grouped in tables, statistically analyzed and subsequently transformed into graphics for better visualization, presentation and discussion of same.
RESULTS
In Figure 1 the city of Bethlehem contributed 21% of cases occurring in the State of Pará in the year 2007, approximately 13,955 cases; Already in 2008 noted a reduction in the incidence of cases, declining to only 9% throughout the year; However, it was noticed that in the following years of 2009 and 2010 there was a growth in this index.
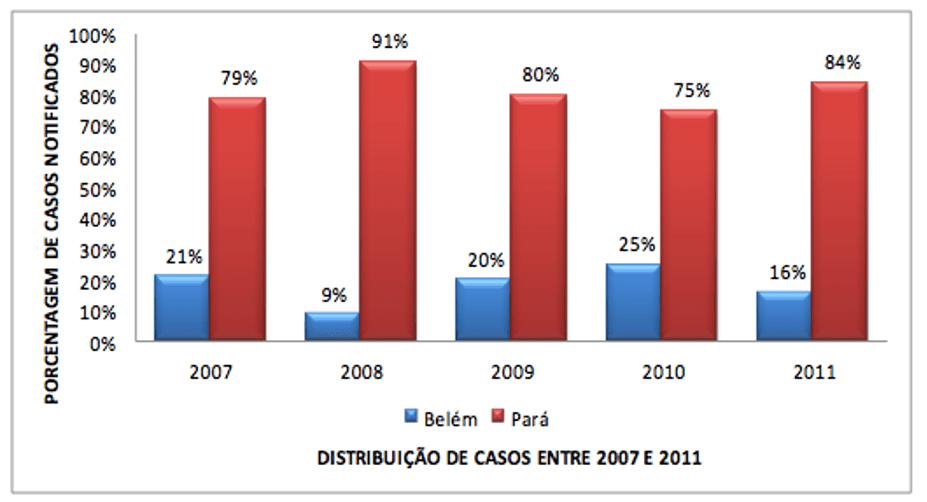
It is worth mentioning that, in the year 2010, Bethlehem was responsible for the highest percentage in those periods, with approximately a quarter of all cases in the State. While in the year 2011 there was again a decrease, getting a percentage of 16% in relation to the registered in the Stop (Figure 1).
Regarding the prevalence of dengue fever, stratified by year and related to clinical form of dengue, which were found throughout the study period, there has been no case notified of Dengue shock syndrome (SCD) (Figure 2).
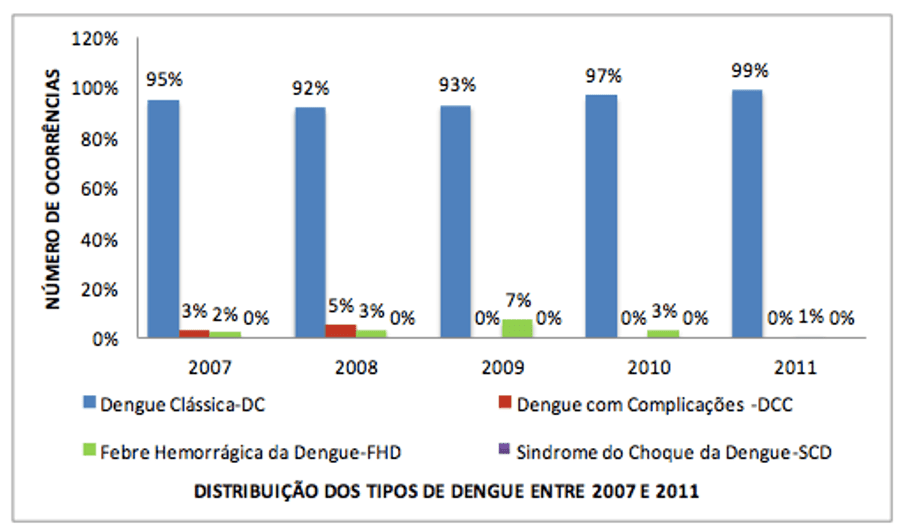
The same was observed with Dengue with complications (DCC) in the years 2009, 2010 and 2011. However, it is worth mentioning that, in the case of Classical Dengue (DC) there was a remarkable number of occurrence of the disease, and there is a constant in their notification for each year surveyed. In the case of Dengue hemorrhagic fever (DHF) found that there were records for the years 2007 to 2011, with a decrease in the latter year.
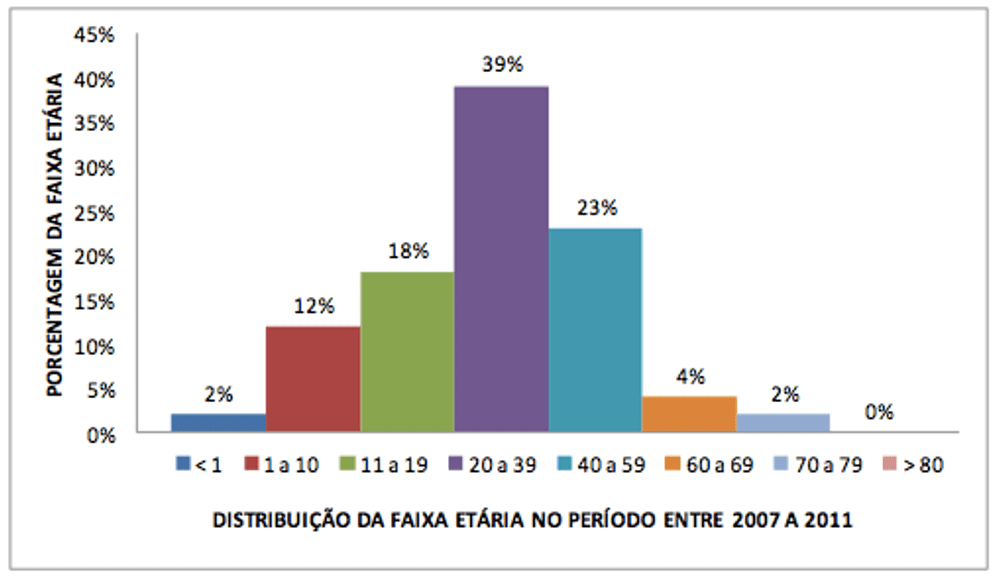
To verify the data by age group (Figure 3) realizes that in the period from 2007 to 2011, the largest number of dengue fever cases occurred in individuals from the age group between 20 to 39 years, which were the most affected by the virus, representing a total of 39% of cases, followed by 23% to the age group of 40 to 59 years.
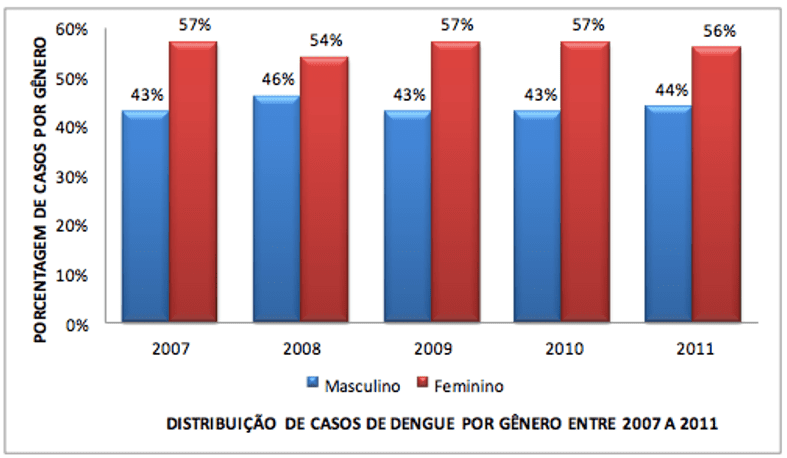
In relation to the prevalence of dengue as the gender (sex), (Figure 4), stratified in the period under study, of 2007 to 2011, remained invariant in the reported data of dengue, where the male was between 43 to 46%, and the female between 54 to 57%. Therefore, we find that the female represents a percentage higher compared to males, throughout the period under study.
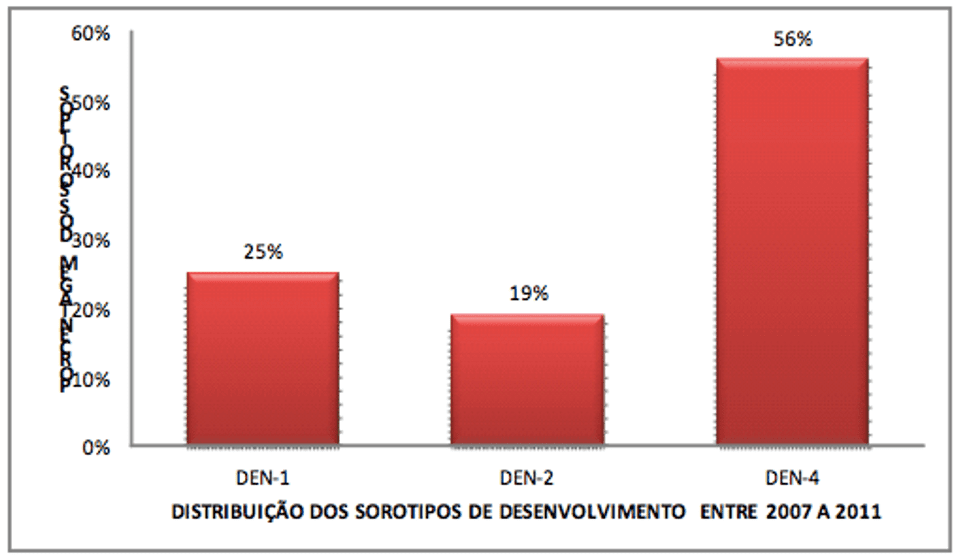
The analysis of the information about the reported cases of dengue serotype 1, 2, 3 and 4, as shown in Figure 5. In the period from 2007 to 2011 the greater frequency of cases of dengue fever, in the metropolitan region of Belém, was of serotype 4 with 56% of cases; then the serotype 1 with 25%; and the serotype 2, with 19%; having no occurrence to the serotype 3.
DISCUSSION
Dengue is one of the main public health problems across the country, and this is due to its easy expansion and the potential for severe and even fatal (PAHO, 1991; TORRES, 2008). The results obtained with the implementation of the present research underline the need for more effective prevention in the city of Bethlehem, especially in relation to the vector of the disease, since it is already known that the registry index of dengue during the years surveyed reported considerable in terms of public health. This is demonstrated by the more confirmation criterion used in the municipality, which is the confirmation by means of clinical epidemiological data, with the support of viral isolation tests carried out in laboratories, trained to detect circulating serotype in this region.
The comparison of the involvement of the disease in relation to sex also requires attention, since women are more affected, because they are more subject to the attack vector. In this sense also public health programs should exist for this genre, as better guidance about environmental care that must be adopted in the home.
This is, probably, the two classes are more subject to infection by the vector, and for being more active professionally, which can provide a greater risk of contracting the disease. This data is according to the survey conducted in Paudex, Monteiro et al. (2006), where data show equivalent of contamination for this same age group. According to data from the literature, this is due to women’s clothing, because the mosquito vector is preferred by sugar mainly in feet or in the lower parts of the legs; However, this does not mean that these insects cannot suck up other parts of the human body and to animals (NAIR, 2003). It is worth mentioning that these same data are similar to those found by Varga and Oke through similar research conducted in Dourados-MS (2009), what can a priori characterize a disease profile.
The inclusion of serotype 4 stock in the region is another factor that deserves highlight by becoming a given worrisome because it shows the versatility of the serotypes, causing a greater attention to all serotypes and no more specific types.
To understand the epidemiological situation that is worrying, it is necessary to be a linkage between the three levels of Government (municipal, State and federal), along with the community itself, with permanent control of this disease. Since the advancement of dengue is generated by a static society, is that we should sensitize the population so that there is a collective combat, especially with more effectiveness.
In the city of Belém, the difficulty in controlling the proliferation of vector occurs due to basic sanitation conditions and the high concentration of the population in the peripheral area. It is necessary to maintain continuously educational activities to clarify the population about the disease and combating vector (GONÇALVES NETO et al., 2004).
The results found here deserve a special attention, since, according to the data of the Ministry of health, the serotype 4 had a notable movement with increase in the number of cases reported in Brazil in the last two years (2010-2011) (BRAZIL, 2011), which confirms the data found in this research. It is believed that the occurrence of reported cases in the region point to the influence of climatic factors, which provided adequate conditions for the development of Aedes aegypti, and other locational and environmental factors. Note, too, that the concentration of the majority of the cases, occurs in the summer, when weather conditions, precipitation, temperature and moisture are favorable to their proliferation.
It is noteworthy that, in the year 2010, Bethlehem was responsible for the highest percentage in those periods, with approximately a quarter of all cases in the State. While in the year 2011 there was again a decrease, getting a percentage of 16% in relation to registered in Pará, which may have been motivated due to lack or ineffectiveness of campaigns as the fight especially the breeding grounds of the Aedes aegypti mosquito, responsible for transmitting the disease.
CONCLUSION
We can say that the majority of the number of cases usually occurs when the temperature and rainfall are higher, which causes an increase in the population of the mosquito vector. It is well-established that water accumulated in puddles or containers several favors the proliferation of Aedes aegypti larvae.
Thus, it is essential to the existence of stronger actions by the population for the control of vectors can be accomplished more efficiently; otherwise, epidemics remain a constant in the region.
Noting that the best way to control the increase of dengue cases is fighting the breeding grounds of mosquitoes, through campaigns for the Elimination of breeding grounds and awareness of the population of the affected areas and, since there is so far no vaccine or medicine specific to the disease.
REFERENCES
AGUIAR, Adriana Chan. Epidemiological surveillance Support text. Rio de Janeiro: Fiocruz, 1998.
BARRETO, M. L.; Teixeira, m. g. epidemiological situation and contributions to a research agenda. Advanced studies, v. 22, n. 64, 2008.
BRAGA, I. A.; VALLE, a. Aedes aegypti: control in Brazil’s history, epidemiology and Health Service, Brasilia, v. 16, n. 2, Apr/jun. 2007.
Brazil. Ministry of health. Secretariat for health care. Department of basic attention. Health surveillance: epidemiological surveillance Department. Infectious and parasitic diseases: Pocket Guide: 7.ed.rev. Brasília: Ministry of health, 2008a.
Brazil. Secretariat for health care. Department of basic attention. Health surveillance: Dengue fever, Schistosomiasis, leprosy, malaria, Trachoma and tuberculosis. 2. Ed. rev. Brasília: Ministry of health, 2008b.
Brazil. Ministry of health. National Health Foundation. Dengue: epidemiological aspects, diagnosis and treatment. Brasília: Ministry of health, 2011.
Brazil. Ministry of health. Dengue: nursing Manual-adult and child. Brasília: Ministry of health, 2008 c.
Borges, Sonia m. a. epidemiological Importance of Aedes aegypti Albopictus in the Americas. São Paulo:[S.n.], 2001.
COSTA, Benedict a. classification, types and treatment of dengue fever. [S.l.:S.n.], 2005.
Dantas, Vincent S.; PASSONI, Louis f. c. Dengue: resurgence of an old disease, medical journal, Rio de Janeiro, v. 37, no. 2, 2003.
DENGUE FEVER. Notifications: recorded in the information system of reportable diseases SINAM-NET 2007 to 2011.
DONALÍSIO, M. R.; GLASSER, C m. Entomological surveillance and vector control of dengue, Brazilian Journal of epidemiology. v. 5, no. 3, 2002.
FIGUEIREDO, Louis t. m. Pathogenesis of Dengue virus infections. Ribeirão Preto:[S.n.], 1999.
FIGUEIREDO, Louis t. m. virus hemorrhagic fever in Brazil. Medical journal, v. 39, p. 203-210, sea,/abr., 2006.
FOCACCIA, Roberto. Treaty of infectious diseases: v. 3. São Paulo: Atheneu, 2005.
GAUTAM NAIK, V. S.; Rebelo, j. m. m. epidemiological Aspects of dengue fever in the city of São Luís, Maranhão, Brazil, 1997-2002. CAD. Saúde pública, Rio de Janeiro, 2004.
EVANDRO CHAGAS INSTITUTE. Infectious and parasitic diseases: Amazon Approach. Bethlehem: Cejup/University of Pará; 1997.
LEVINSON, Warren; JANETZ, Ernest. Microbiology. 7. Ed. Porto Alegre: New Haven, 2005.
LÍPI, Osmar; LAMB, Charles G.; RABBIT, Ivo c. b. imunocutâneas Manifestations of dengue. [S.l.: S.n.], 2007.
MINAYO, M. C. S. The challenge of knowledge: qualitative research in health. 7. Ed. São Paulo-Rio de Janeiro: Hucitec-Abraseo, 2000.
Monteiro, e. s. c. et al. Epidemiological aspects and vector of dengue in the city of Teresina, Piauí-Brazil, 2002 and 2006. [S.l.: S.n.], 2006.
MYAZAKI, Pink Djunto et al. Monitoring of the Aedes aegypti mosquito. Brazilian Journal of Tropical Medicine. Uberaba, v. 42, no. 4, July,/ago., 2009.
SNOW, David Parker. Human Parasitology. 10. Ed. São Paulo: Atheneu, 2003.
PAHO. PAN AMERICAN HEALTH ORGANIZATION. Guidelines relating to the prevention and control of dengue and dengue hemorrhagic fever in the Americas. Washington, 1991. Meeting report on guidelines for dengue fever, 1991.
Rebelo, j. et al. Distribution of Aedes aegypti and dengue fever in the State of Maranhão, Brazil, book of public health, Rio de Janeiro, v. 15, n. 3, Jul./set. 1999.
SÁNCHEZ, l. et al. Education strategy to promote the participation of the community in the prevention of dengue fever. Panama Magazine. Public health, v. 24, n. 1, p. 61-69, 2008.
SERUFO, j. c. et al. Dengue fever: A new approach. Journal of the brazilian society of tropical medicine, v. 33, n. 5, p. 465-476, Sept./out., 2000.
SETÚBAL, Sergio; OLIVEIRA, Solange a. de. Infectious and parasitic diseases: Department of clinical medicine, Apr. 2006.
SHARMA, Marcia. Nursing care in infectology. São Paulo: Atheneu, 2006.
SHARMA, s. et al. Comparative study between the monthly rainfall and the number of dengue cases reported. Rev. Bethlehem, 2003.
TAUIL, Pedro l. critical aspect of the control of dengue fever in Brazil, Public health, Rio de Janeiro, v. 18, no. 3, may/jun. 2002.
TEIXEIRA, M. G.; BARRETO, M. L.; WAR, Z. Epidemiology and prevention of dengue fever. v. 8, n. 4, Brasilia, Dec. 1999.
TORRES, Eric M. Dengue Fever. Advanced studies, v. 22, no. 64, p. 35-52, 10, 2008.
VERONESSI, Richard. Infectious diseases. V. 3. Rio de Janeiro: Guanabara koogan, 2004-.
VIEGAS, S.; OLIVEIRA, r. Epidemiology of dengue in the years 2009 and 2010 in the city of DOURADOS/MS, gilded:[S.n.], 2009.
VITA, w. p. et al. Dengue: clinical and laboratory Alerts of severe disease evolution. [S.l.:S.n.], 2008.
[1] Studen by Amazon Metropolitan College FAMAZ
[2] Studen by Amazon Metropolitan College FAMAZ
[3] Studen by Amazon Metropolitan College FAMAZ
[4] Biomedical. Doctorate in Tropical Diseases. Lecturer and researcher at the Federal University of Amapá, AP. And lecturer of the Graduate program of the Center for Tropical Medicine at the University of Pará – UFPA.
[5] Biologist. Doctor in theory and research. Lecturer and researcher at the Federal Institute of Amapá-IFAP.
[6] Biologist. Doctor of medicine/Tropical Diseases. Lecturer and researcher at the Federal University of Pará; A researcher at the Graduate program of the Core of Tropical Medicine at the University of Pará – UFPA.















