ORIGINAL ARTICLE
DIAS, Claudio Alberto Gellis de Mattos [1], ARAÚJO, Maria Helena Mendonça de [2], SILVA, Anderson Walter Costa [3], OLIVEIRA, Euzébio de [4], DENDASCK, Carla Viana [5], FECURY, Amanda Alves [6]
DIAS, Claudio Alberto Gellis de Mattos. et al. Confirmed cases of tuberculosis in Brazil between 2015 and 2019. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year. 07, Ed. 11, Vol. 01, pp. 153-160. November 2022. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/confirmed-cases, DOI: 10.32749/nucleodoconhecimento.com.br/health/confirmed-cases
ABSTRACT
Tuberculosis (TB) is a communicable disease considered serious. The time difference between obtaining test results from a patient and starting treatment increases the chance of transmitting tuberculosis. The purpose of this article was to verify the number of confirmed cases of tuberculosis in Brazil between 2015 and 2019 according to the notification region, age group, form of the disease and closure situation. For this, a qualitative and quantitative research was carried out. Quantitative data were taken from the IT department of the Brazilian Unified Health System (DATASUS)[7]. Regions of the country with the highest HDI seem to deal better with the transmission, treatment and cure of tuberculosis. The economically active population, with greater exposure to other people, are the most affected group due to the type of transmission. The pulmonary type of tuberculosis affects the largest number of people due to the form of airborne transmission and also the performance of the body’s immune system, with the fight being maintained at the cavity level. The high rate of success in the treatment (cure) reflects that there is a real possibility of combating the bacillus. Unfortunately, the abandonment rate demonstrates how bad a social imbalance can do to public health.
Keywords: Tuberculosis, DATASUS, Epidemiology, Public Health.
INTRODUCTION
Tuberculosis (TB) has been known since antiquity and, currently, its forms, transmission and treatment are completely known thanks to technological and scientific advances (Martins et al., 2016). It is a transmissible disease considered serious, appearing on the list of diseases that kill the most in the world (Silva, F. T. et al., 2020).
TB is caused by an elongated bacterium called Koch’s Bacillus (KB). Its scientific name is Mycobacterium tuberculosis and it is transmitted mainly by droplets of saliva through the air, when the infected person coughs or sneezes (Jesus et al., 2020).
Tuberculosis can affect various parts of the human body. Most cases occur within the cavity of the lung and are called the pulmonary type. However, the bacillus can settle in other organs, such as lymphatic vessels, bones, joints, meninges, central nervous system and gastrointestinal tract. In these cases, it is called extrapulmonary tuberculosis (Rocha et al., 2020).
Social differences tend to increase the spread of TB. Age, income, unemployment, living conditions and access to health are factors that make it difficult to control this disease (Oliveira et al., 2021).
There are also gender differences in commitment. Men whose lives are associated with alcoholism and the use of illicit substances appear as the highest number of infected people, to the detriment of females (Oliveira, A. V. S. D. et al., 2020).
Economic activity also influences the group considered more vulnerable to the disease. Economically active men between 21 and 50 years old are the age group with the highest number of infections (Thomé et al., 2020).
Brazil’s regional conditions also appear to affect the number of cases in each of the five regions. This makes it more difficult to control the disease in the country (Cortez et al., 2021).
The time difference between obtaining the test results of a patient and starting treatment increases the chance of transmission of tuberculosis, especially in the pulmonary form. The Brazilian Unified Health System (SUS)[8] has implemented Rapid Molecular Tests (RMT) that speed up the identification of infected individuals (Oliveira, L. F. D. et al., 2020). Early diagnosis associated with agile treatment are considered the most efficient measures to control and combat the spread of tuberculosis (Valença et al., 2020).
OBJECTIVE
Check the number of confirmed cases of tuberculosis in Brazil between 2015 and 2019 according to the notification region, age group, form of the disease and closure situation.
METHOD
The research is qualitative and quantitative, which implies that “the quantitative and qualitative treatments of the results can be complementary, enriching the analysis and final discussions” (Schneider et al., 2017). From then on, data were taken from the IT department of the Brazilian Unified Health System (DATASUS). Information was extracted from the page Cases of Tuberculosis – Since 2001 (SINAN), which is located within the Epidemiological and Morbidity item. Tuberculosis data were selected according to notification region, age group, form of disease and closure situation. The period chosen to collect the information was from 2015 to 2019.
RESULTS
The results found in this research are described and also demonstrated in the texts and graphics below.
Figure 01 In this graph we can see the percentage of confirmed cases of Tuberculosis (TB) according to the region of Brazil in which they were notified, between the years 2015 and 2019
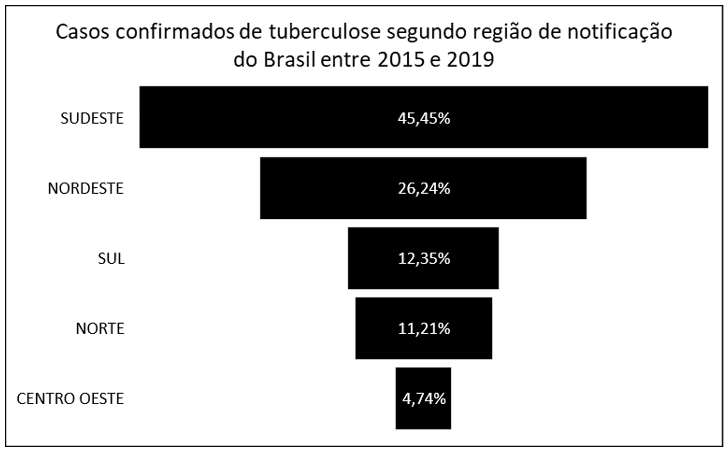
It can be noted that the southeast region of Brazil had the highest number of cases (45.45%). After this region, in decreasing order of number of confirmed cases, appear the northeast (26.24%), south (12.35%) and north (11.21%). The lowest number of confirmed TB cases occurred in the Midwest region (4.74%).
Figure 2 In the following graph, it is possible to verify the percentage of confirmed cases of Tuberculosis (TB) according to age group, distributed in years, between 2015 and 2019
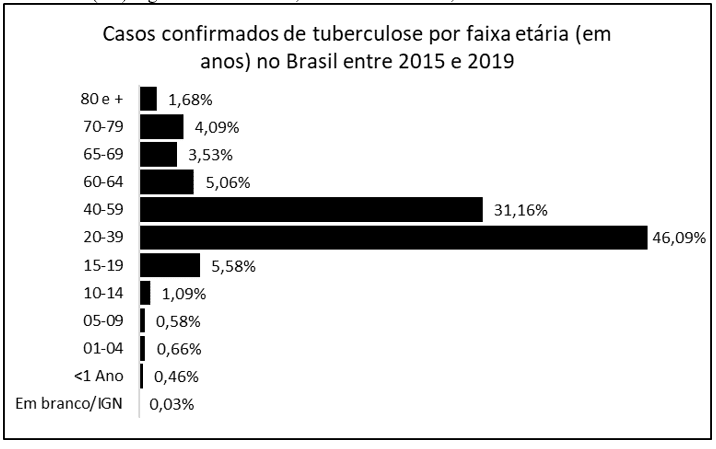
It is possible to distinguish in the graph that the highest percentage of confirmed cases between the years 2015 to 2019 occurred in the age group between 20 and 39 years old (46.09%), followed by 40 to 59 years old (31.16%). Among the other numbers of cases are the ranges from 15 to 19 years old (5.58%), 60 to 64 years old (5.06%), 70 to 79 years old (4.09%), 65 to 69 years old (3, 53%), 80 and over (1.68%) and 10 to 14 years (1.09%). The other ranges appear with less than 1% of confirmed TB cases.
Figure 3 The following graph shows the percentage of confirmed cases of Tuberculosis (TB) according to the form of the disease, between 2015 and 2019
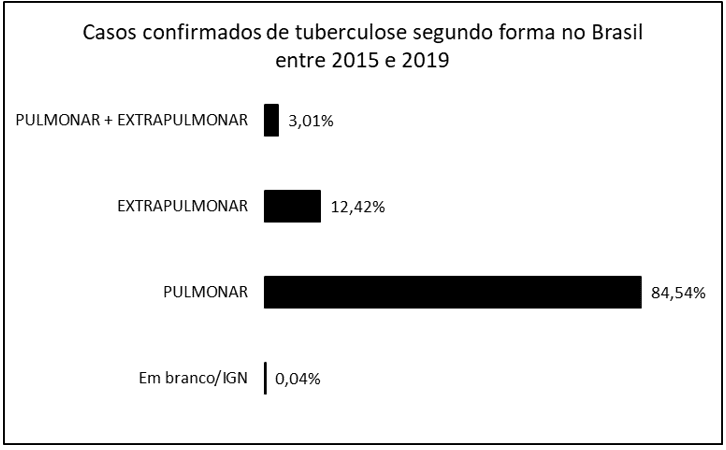
The data that appear in the graph above show the largest amount being reported as the pulmonary form (84.54%). The extrapulmonary form was reported in 12.42% of cases and the mixed form (pulmonary and extrapulmonary) in 3.01%.
Figure 4 In the following graph, it is possible to verify the percentage of confirmed cases of Tuberculosis (TB) by closure situation, between the years 2015 and 2019
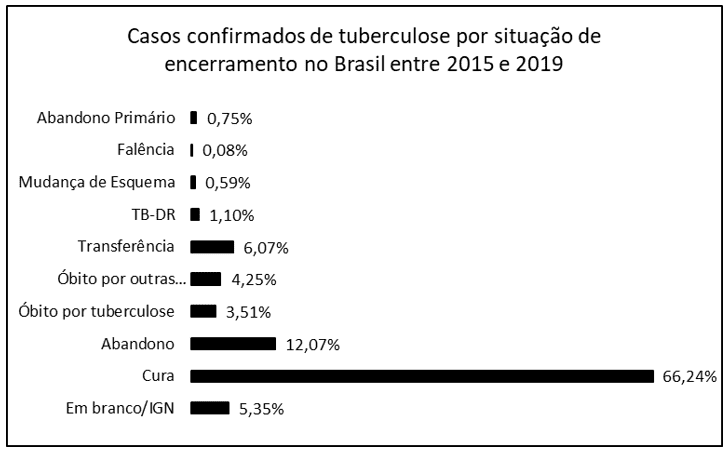
The graph above demonstrates that the highest notifications were of cure (66.24%). The level of abandonment of treatment reached 12.07%. This is followed by patient transfer (6.07%), death from other causes (4.25%), deaths from TB (3.51%), XDR TB (Drug Resistant Tuberculosis) 1.10%, change of regimen (0. 59%), primary dropout (0.75%) and bankruptcy (0.08%).
DISCUSSION
In Brazil. The southeast region had the highest number of cases (45.45%) (graph 1). The southeast region has the largest population in the country, therefore with a greater possibility of transmission between people. It has been reported that there is a relationship between the number of people in a population and the incidence of communicable diseases such as tuberculosis. The Midwest of the country (with 4.74% of TB cases) has one of the best Human Development Indexes (HDI) among regions. A satisfactory index could explain the lower percentage in this region. Studies point to lower morbidity from tuberculosis in places with better HDI (Cortez et al., 2021). Social differences can also affect the number of cases in each location, taking into account the transmission rate of the bacteria (Oliveira et al., 2021).
The most affected age groups are between 20 and 39 years old (46.09%) and 40 to 59 years old (31.16%), as we can see in Graph 2. having greater ability to move around and interact within society, they would be more exposed to contagion (Pedro and Oliveira, 2013). Another parameter that can be used to explain a higher rate in these age groups is economic activity. Women and especially men, between 21 and 50 years old, have more contact with other human beings due to their daily work (Thomé et al., 2020).
The results unequivocally point to the pulmonary form as the type of tuberculosis that affects the highest number of infected people (84.54%) (graph 3). The greatest transmission of TB occurs from individual to individual through droplets expelled orally or nasally(Jesus et al., 2020). The bacillus lodges in the bronchi, bronchioles and lung alveoli, initiating the infection. There is little chance that it leaves the air system to infect other parts of the body, as the immune system begins to fight it in these parts. This is probably why the rates for these types of Tb are so much higher than the percentages for other types (Martins and Miranda, 2020).
Graph 4 shows a high cure rate (66.24%), but with a notable level of abandonment (12.07%). Infected patients are treated with drugs that are usually long-lasting or have little effect, depending on the sensitivity or resistance presented (Silva, D. R. et al., 2020). This factor associated with TB is more infectious in individuals with lower social structure and, consequently, cultural structure seems to influence the decision to abandon treatment. The lack of understanding of the disease and its consequences, as well as the treatment, can lead the patient to this wrong decision (Berra et al., 2020).
Tuberculosis transmission affects, with a higher rate, men with low education and income, with unskilled jobs or without structure to live (street dwellers), some are still users of alcohol or illicit drugs. Thus, the vulnerable situation of the present inequality seems to directly influence Mycobacterium tuberculosis infection in Brazil (Nunes et al., 2020).
CONCLUSION
Regions of the country with the highest HDI seem to deal better with the transmission, treatment and cure of tuberculosis.
The economically active population, with greater exposure to other people, are the most affected group due to the type of transmission.
The pulmonary type of tuberculosis affects the largest number of people due to the form of airborne transmission and also the performance of the body’s immune system, with the fight being maintained at the cavity level.
The high rate of success in the treatment (cure) reflects that there is a real possibility of combating the bacillus. Unfortunately, the abandonment rate demonstrates how bad a social imbalance can do to public health.
Educational conditions and economic gains becoming more balanced in our country would probably greatly reduce public spending on care and treatment of infectious diseases and, perhaps, others.
REFERENCES
BERRA, T. Z. et al. Fatores relacionados, tendência temporal e associação espacial do abandono de tratamento para tuberculose em Ribeirão Preto-SP. Rev. Eletr. Enferm., 2020; 22:, , v. 22, n. 58883, p. 1-10, 2020. Disponível em: < https://www.revistas.ufg.br/fen/article/view/58883/34953 >.
CORTEZ, A. O. et al. Tuberculose no Brasil: um país, múltiplas realidades. J Bras Pneumol., v. 47, n. 2, p. 1-11, 2021. Disponível em: < https://www.jornaldepneumologia.com.br/export-pdf/3449/2021_47_2_3449_portugues.pdf >.
JESUS, M. D. C. D. et al. Casos confirmados de tuberculose no Brasil, na Região Norte, no Estado do Amapá e no Município de Macapá, entre 2013 e 2017. Revista Científica Multidisciplinar Núcleo do Conhecimento, v. 1, p. 144-154, 2020. Disponível em: < https://www.nucleodoconhecimento.com.br/saude/tuberculose-no-brasil >.
MARTINS, C. S. C. et al. Perfil epidemiológico da tuberculose na população do Município de Belém-Pará, Brasil: Estudo na Unidade Municipal de Saúde de Fátima. Revista Científica Multidisciplinar Núcleo do Conhecimento, v. 2, p. 129-144, 2016. Disponível em: < https://www.nucleodoconhecimento.com.br/saude/perfil-epidemiologico-da-tuberculose >.
MARTINS, V. D. O.; MIRANDA, C. V. D. Diagnóstico e tratamento medicamentoso em casos de tuberculose pulmonar: Revisão de literatura. RSM – Revista Saúde Multidisciplinar, v. 1, n. 7, p. 01-10, 2020. Disponível em: < http://revistas.famp.edu.br/revistasaudemultidisciplinar/article/view/111/109 >.
NUNES, C. C. et al. Aspectos socioeconômicos e a coinfecção tuberculose/hiv no brasil: Uma revisão da literatura. Educ. Ci. e Saúde, v. 7, n. 2, p. 162-179, 2020.
OLIVEIRA, A. H. et al. Necessidades de saúde das pessoas com tuberculose pulmonar. Rev. Enferm. UFSM, v. 11, p. 1-18, 2021. Disponível em: < https://periodicos.ufsm.br/reufsm/article/view/43901/html >.
OLIVEIRA, A. V. S. D. et al. Perfil epidemiológico da tuberculose no Nordeste do Brasil: série temporal de 2008 a 2018 Research, Society and Development, v. 9, n. 2, p. 1-17, 2020. Disponível em: < https://rsdjournal.org/index.php/rsd/article/view/2129/1748 >.
OLIVEIRA, L. F. D. et al. Tuberculose: avaliação do tempo entre a identificação dos sintomas e o início da terapêutica. Rev Bras Enferm., v. 73, n. 6, p. 1-6, 2020. Disponível em: < https://www.scielo.br/pdf/reben/v73n6/pt_0034-7167-reben-73-06-e20180902.pdf >.
PEDRO, A. S.; OLIVEIRA, R. M. D. Tuberculose e indicadores socioeconômicos: revisão sistemática da literatura. Rev Panam Salud Publica. 2013;33(4):294–301, v. 33, n. 4, p. 294–301, 2013. Disponível em: < https://www.scielosp.org/pdf/rpsp/2013.v33n4/294-301/pt >.
ROCHA, M. S. D. P. et al. Mortalidade e prevalência da tuberculose pulmonar e extrapulmonar no município de Jataí/GO. Braz. J. of Develop., v. 6, n. 8, p. 61474-61487, 2020. Disponível em: < https://www.brazilianjournals.com/index.php/BRJD/article/view/15516/12767 >.
SCHNEIDER, E. M.; FUJII, R. A. X.; CORAZZA, M. J. Pesquisas Quali-Quantitativas: Contribuições para a pesquisa em ensino de ciências. Revista Pesquisa Qualitativa, v. 5, n. 9, p. 569-584, 2017. Disponível em: < https://editora.sepq.org.br/index.php/rpq/article/download/157/100 >.
SILVA, D. R.; FERNANDA CARVALHO DE QUEIROZ MELLO; MIGLIORI, G. B. Esquemas mais curtos de tratamento da tuberculose: o que há de novo? J Bras Pneumol. 2020;46(2), v. 46, n. 2, p. 1-8, 2020. Disponível em: < https://www.scielo.br/pdf/jbpneu/v46n2/pt_1806-3713-jbpneu-46-02-e20200009.pdf >.
SILVA, F. T. et al. Número de casos confirmados de tuberculose no Brasil entre 2007 e 2016. Revista Científica Multidisciplinar Núcleo do Conhecimento, v. 4, p. 94-104, 2020. Disponível em: < https://www.nucleodoconhecimento.com.br/saude/casos-confirmados-de-tuberculose >.
THOMÉ, H. R.; ANDRADE, S. M. D.; SALAMANCA, M. A. B. Características clínicas, epidemiológicas e georreferenciamento da tuberculose em um centro de referência do oeste do Paraná. R. Saúde Públ., v. 3, n. 1, p. 86-9, 2020. Disponível em: < http://revista.escoladesaude.pr.gov.br/index.php/rspp/article/view/332/118 >.
VALENÇA, Í. M. D. O. et al. Perfil epidemiológico dos casos de tuberculose drogarresistente. REAS/EJCH, n. 56, 2020. Disponível em: < https://acervomais.com.br/index.php/saude/article/view/4334/2560 >.
APPENDIX – FOOTNOTE
7. Departamento de Informática do Sistema Único de Saúde (DATASUS).
8. Sistema Único de Saúde (SUS).
[1] Biologist, PhD in Theory and Research of Behavior, Professor and researcher at the Degree Course in Chemistry at the Instituto de Ensino Básico, Técnico e Tecnológico do Amapá (IFAP), at the Programa de Pós Graduação em Educação Profissional e Tecnológica (PROFEPT IFAP) and at the Postgraduate Program in Biodiversity and Biotechnology of the BIONORTE Network (PPG-BIONORTE), Amapá pole.
[2] Physician, Professor and researcher at the Medical Course at the Universidade Federal do Amapá (UNIFAP).
[3] Physician, Specialist in Systems Management and Health Services. Professor, preceptor and researcher at the Campus Macapá Medicine Course, Universidade Federal do Amapá (UNIFAP).
[4] Biologist, PhD in Tropical Diseases, Professor and researcher at the Physical Education Course at the Universidade Federal do Pará (UFPA).
[5] PhD in Psychology and Clinical Psychoanalysis. Doctorate in progress in Communication and Semiotics at the Pontifícia Universidade Católica de São Paulo (PUC/SP). Master’s Degree in Religious Sciences from Universidade Presbiteriana Mackenzie. Master in Clinical Psychoanalysis. Degree in Biological Sciences. Degree in Theology. He has been working with Scientific Methodology (Research Method) for more than 15 years in the Scientific Production Guidance of Master’s and Doctoral Students. Specialist in Market Research and Health Research. ORCID: 0000-0003-2952-4337.
[6] Biomedical, PhD in Tropical Diseases, Professor and researcher at the Campus Macapá Medicine Course, Universidade Federal do Amapá (UNIFAP), and at the Programa de Pós-graduação em Ciências da Saúde (PPGCS UNIFAP), Pro-Rector of Research and Postgraduate Graduation (PROPESPG) from the Universidade Federal do Amapá (UNIFAP).
Submitted: November, 2022.
Approved: November, 2022.















