INTEGRATIVE ARTICLE
SIMÃO, Felipe Eduardo Pissolati [1], MAGALHÃES, Maria da Consolação [2]
SIMÃO, Felipe Eduardo Pissolati. MAGALHÃES, Maria da Consolação. Hospitalizations for conditions sensitive to primary care: an integrative review of the Brazilian literature. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 06, Ed. 04, Vol. 02, p. 27-58. April. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/conditions-sensitive, DOI: 10.32749/nucleodoconhecimento.com.br/health/conditions-sensitive
ABSTRACT
Hospitalizations for Conditions Sensitive to Primary Care have been used as an indicator of the quality of the first level of health care. The objective of this work is to analyze the national scientific production, aiming to identify notes referring to: types of data; health financing; social determinants of health and the articulation of Health Care Networks. This is an integrative literature review carried out in Medline, Lilacs and Scielo databases. After applying the inclusion and exclusion criteria, 39 works were selected for analysis. Results demonstrate the need for caution in the evaluation of secondary data of the indicator and the need to expand the use of complementary strategies that help in the identification of factors associated with hospitalization. Being the indicator of hospitalizations sensitive to primary care, strategic for the planning of actions and the correct use of health resources. A great association of avoidable hospitalizations with social determinants and conditions of health was identified, however, being this theme and the articulation, communication of the Health Care Network, with the smallest number of works developed. Thus, we can conclude that it is necessary to expand studies focused on these themes, aiming at pointing out actions and policies that contribute to the development and formation of participatory teams and to change the hegemonic paradigm of health work processes.
Keywords: Hospitalization, Hospitalization, Primary Health Care, Quality of health care.
1. INTRODUCTION
Hospitalization for Conditions Sensitive to Primary Care (ICSAP) is a concept that has been applied in several countries as an indirect indicator of the effectiveness of the first level of health care and used as a marker of quality and access to primary health care (PHC). The indicator reveals the health situation of an individual or the population itself, allowing reflection on the organization of health services as well as on the health status of the population, grouping different causes of hospital admission of conditions particularly managed in primary health care (PHC) (RODRIGUES-BASTOS et al., 2013; AVELINO et al., 2014; MALVEZZI, 2018; NEDEL et al., 2011).
Health promotion and protection, early diagnosis and treatment of the illness process, control and monitoring of chronic conditions are imperative to reduce hospitalizations for sensitive conditions. PHC with low resolution, thus, is associated with the maintenance of high rates of ICSAP, which has unnecessary costs and displacements, including readmissions and prolonged hospital stay (ALFRADIQUE et al., 2009; MORETTI et al., 2016).
In the international context, we can identify numerous investigations on indicators of hospital activity as a measure of the effectiveness of PHC. Scientific studies carried out in Canada and Europe demonstrate the concern regarding the definition and validation of lists of health problems which coordinated actions would reduce injuries and hospitalizations (ALFRADIQUE et al., 2009; RODRIGUES-BASTOS et al., 2013).
The concept of primary care sensitive health problems originated in the 1990s in the United States of America (USA). Ambulatory Care Sensitive Conditions, translated into Portuguese as Condições Sensíveis à Atenção Primária (CSAP), was coined by Billings et al. (1993) as an outcome of the concept of preventable deaths. Starting from this point, the aim was to contemplate adaptations seeking territorial and context specificities to be applied. Rehem et al. (2013) point out as an example that, in Spain, to improve the indicator, greater specificity is sought, analysis by municipalities, seeking to increase the problem-solving capacity by identifying problematic health regions that need better coordination between levels of care. The Organization for Economic Cooperation and Development (OECD) uses this indicator, through its member countries, as an indicator of access to quality care (RODRIGUES-BASTOS et al., 2013; REHEM et al., 2013).
In Brazil, with the implementation of the Unified Health System (SUS), consolidated by the Federal Constitution of 1988, the impetus for the formation of integrated, regionalized and decentralized care networks began, which aim to guarantee access to health. Health networks are organizations of service sets with common goals and cooperative, interdependent actions for continuous care. PHC has a fundamental role in the ordering of flows and counterflows of the health care system, with the exception of urgent cases (COSTA et al., 2014; REHEM et al., 2013).
Currently, the country is still experiencing major changes in the structure of the Unified Health System. Starting in 1994, five years after the beginning of the SUS and facing obstacles in its implementation, the Programa Saúde da Família (PSF)[3], which was extended to the Estratégia Saúde da Família (ESF)[4], designed the strategy to improve access, quality and promotion of PHC. Since the Política Nacional de Promoção da Saúde (PNPS)[5] only became a reality in 2006 and only approved in 2014, thus favoring the dimension of the social determinants and conditions of health involved in the health-disease process and with the purpose of intersectoriality. In Brazil, PHC has a structuring character in municipal health systems, seeking to increase rationality in the use of care levels, functioning as a guiding element of care. Avelino et al. (2014), records in their work PHC attributions such as first contact, longitudinality, integration, coordination, family focus and community orientation, centralizing health promotion and disease prevention actions, directing to meet social health needs and improving the quality of life, playing an important role as a communication center for the network. Thus, enabling the reorganization of demands as a way of changing the hospital-centered and medical-centered care model, influences of the Cartesian paradigm (MALTA et al., 2018; ALFRADIQUE et al., 2009; NEDEL et al., 2011; AVELINO et al., 2015; MALVEZZI, 2018).
Thus, aiming at a quality service, at the three levels of health care, we must consider the interpersonal relationships in the care process, valuing the multiprofessional format, which ensures an expanded view of the subject. Therefore, developing humanized articulations, perceiving the user as a subject endowed with subjectivity. In addition, the establishment of multidisciplinary teams expands the performance in relation to the determinants of the health-disease process. In 2008, the Family Health Support Centers (Nasf) were created in Brazil, proposing to expand the matrix support to the actions of PHC teams, thus aiming to reduce indiscriminate referrals to other levels of care (COSTA et al., 2014; CARDOSO et al., 2013; MORETTI et al., 2016).
Focusing on primary care as a priority in the organization of health care is a global trend, appearing as a fundamental component of health reform in many countries. First planned as a way to reduce hospital expenses, PHC is currently gaining importance in valuing integrality, longitudinality of care to the detriment of an exclusively curative, inefficient focus, in order to supply the traditional model of care (CARDOSO et al., 2013; NEDEL et al., 2013; NEDEL et al. al., 2011; NUNES, 2018; MALTA et al., 2018).
In this way, with the purpose of developing yet another tool to contribute to the country’s health network, the Ministry of Health (MOH) consulted several Brazilian specialists to prepare the draft of Ordinance SAS nº221, of April 17, 2008, which publishes the Brazilian List of Hospitalizations for Conditions Sensitive to Primary Care. The adoption of this indicator began by the State Health Departments, which emerged in the Brazilian literature from 2001 onwards, following a systematic discussion within the scope of MOH technicians, managers, researchers and specialists, in 2007, which, together with the conceptual frameworks of the model proposed by authors from other countries, supported the construction of the Brazilian indicator, whose purpose is that timely and quality action can avoid hospitalizations and their frequency. The Brazilian list of ICSAP has 19 groups of causes and 74 hospitalization diagnoses, in accordance with the tenth revision of the International Classification of Diseases and Causes of Death (ICD-10) (ALFRADIQUE et al., 2009; REHEM et al., 2013; CARDOSO et al., 2013; RODRIGUES-BASTOS et al., 2013).
Studies carried out in Brazil indicate that access to quality health care in PHC may be linked to the reduction of ICSAP, that lower rates of these hospitalizations are related to the quality of care and the population’s access. The concentration of scientific articles reveals a growing interest in the use of the ICSAP indicator around the world, but still little is known about fundamental issues for the management of the Brazilian health system, requiring deeper knowledge about how structure, organization, processes of work are associated with the variation of ICSAP (MALVEZZI, 2018; PEREIRA et al., 2014; CARDOSO et al., 2013; ALFRADIQUE et al., 2009; AVELINO et al., 2015; RODRIGUES-BASTOS et al., 2013; NEDEL et al., 2010).
In view of this, the present study had as its research question: To explore aspects associated with social determinants of health, related to ICSAP and to evaluate, in the Brazilian literature, the production on the articulation of Health Care Networks, associating them with the indirect indicator of effectiveness of PHC. With the hypothesis that the social determinants of health, as well as the articulation of the Health Care Network are influential variables in the rates of ICSAP.
Our objective was to know the Brazilian scientific production referring to the indicator Admissions/Hospitalizations due to sensitive conditions in primary health care, specifically aiming to: Identify notes regarding the types of data used in research; observe indications on health financing; associate social determinants of health; explore existing information on the articulation of the health care network.
2. METHODOLOGY
The methodological process of the present study comprised two stages. First, an exploratory search for reference articles on the topic of Hospitalizations for Sensitive Conditions to Primary Care was undertaken and the indications and citations of the analyzed studies were followed up until the saturation criterion was reached. In this way, the study objectives and research questions were defined.
Subsequently, it was decided to carry out careful work in the design of an integrative review, unveiling the production of knowledge in Brazilian literature on the subject. The integrative review indicates current knowledge about a specific topic, coordinating the identification and analysis of the results of independent articles (SOUZA et al., 2010). This study design is intended to provide a synthesis of the current condition of knowledge on a given topic, pointing out gaps and possibilities for carrying out new studies (MENDES et al., 2008).
Based on this premise, what was recommended in the work of Mendes, Silveira and Galvão (2008) was followed for the preparation of this review. Objectives and research questions were formulated to be answered and a search was successively carried out in the main databases recognized in the scientific health area.
Data were collected in July 2020, using three databases to obtain the sample of scientific articles to be evaluated. Medical Literature Analysis and Retrieval System Online (MEDLINE); Latin American and Caribbean Literature on Health Sciences (LILACS), which were accessed through the Virtual Health Library (VHL) – operational platform of the Pan American Health Organization; and Scientific Electronic Library Online (SCIELO).
In the research carried out, the Health Science Descriptors (DeCs) of subjects that correspond to the theme selected for review were used as a search strategy. The indicator Hospitalizations for Conditions Sensitive to Primary Care was divided by the descriptors existing on the official website of the structured and multilingual DeCs vocabulary. DeCs is a vocabulary that was developed from MeSH (Medical Subject Headings) aiming at the use of common terminology for research in multiple languages, also assisting in the retrieval of information (DECS/MESH, 2020). The descriptors were used: Hospitalization, Hospitalization, Primary Care; added by the words: “avoidable” OR “sensitive”.
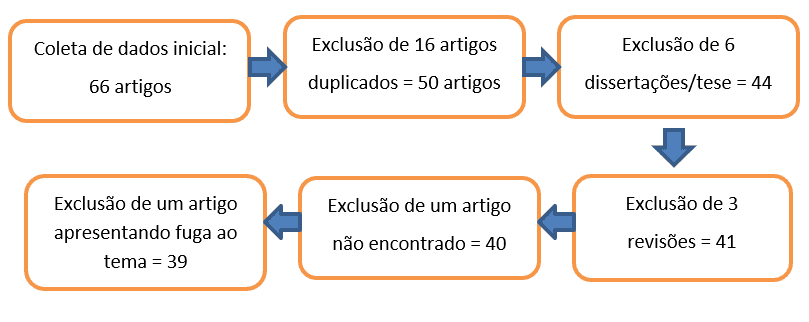
The searches were carried out based on the inclusion criteria of original, complete articles in Portuguese – this being an assessment of the national conditions of the topic addressed, published in scientific journals in the last five years. Based on these results, the following exclusion criteria were applied: duplicate publications, dissertation/thesis works, bibliographic reviews and theme escape, the latter being identified by reading the abstracts of the sample surveyed.
Based on these criteria, it was possible to verify, in the indexed information sources, 66 article titles. Of these, 39 made up the final sample. The phases of the sample definition of the present study are represented in the flowchart of Figure I.
Figure I – Flowchart of the study selection process.
For the characterization of the sample and analysis of the works, the articles were read in full and analyzed with the creation of synthetic tables containing the organization of the composition of the sample information.
3. RESULT
The final study sample was defined in 39 scientific articles. The database with the largest number of works in the sample was on the Lilacs platform, comprising 19 articles; followed by Medline 16 and Scielo 4 articles. The 39 articles that met the proposed criteria were read in full and listed in Table – I, presenting information regarding the database, authors, title and year of publication.
Table I – Database, Authors, Title, Year of publication.
| N.º | Data base | Authors | Title | Year |
| 1. | Lilacs | Freitas et al. | Internações de adolescentes por condições sensíveis à atenção primária em uma regional de saúde | 2018 |
| 2. | Lilacs | Previato et al. | Diminuição de internações por condições sensíveis à atenção primária em idosos no estado do Paraná | 2017 |
| 3. | Lilacs | Pazo et al. | Panorama das internações por condições sensíveis à atenção primária no Espírito Santo, Brasil, 2000 a 2014 | 2017 |
| 4. | Lilacs | Costa et al. | Tendência temporal das internações por condições sensíveis à atenção primária em crianças menores de cinco anos de idade no Ceará, 2000 a 2012 | 2017 |
| 5. | Lilacs | ARRUDA, Jocinei Santos de; COSTA, Juvenal Soares Dias da. | Internações por condições sensíveis à atenção primária em Novo Hamburgo, Rio Grande do Sul | 2017 |
| 6. | Lilacs | BRASIL, Vinicius Paim; COSTA, Juvenal Soares Dias da. | Hospitalizações por condições sensíveis à atenção primária em Florianópolis, Santa Catarina – estudo ecológico de 2001 a 2011 | 2016 |
| 7. | Lilacs | CAMELO, Shinzato Marina; REHEM, Tania Cristina Morais Santos Barbara. | Internações por condições sensíveis à atenção primária em pediatria no Distrito Federal: Um estudo ecológico exploratório | 2019 |
| 8. | Lilacs | Santos et al. | Hospitalização de crianças por condições sensíveis à atenção primária | 2015 |
| 9. | Lilacs | MARIANO, Tatiana da Silva Oliveira; NEDEL, Fúlvio Borges. | Hospitalização por condições sensíveis à atenção primária em menores de cinco anos de idade em Santa Catarina, 2012: estudo descritivo | 2018 |
| 10. | Lilacs | Rehem et al. | Quais aspectos contribuem para a ocorrência de internações por condições sensíveis à atenção primária? | 2016 |
| 11. | Lilacs | Tagliari et al. | Impacto da estratégia saúde da família nas internações hospitalares por condições sensíveis à atenção primária | 2016 |
| 12. | Lilacs | Lima et al. | Perfil dos atendimentos por condições sensíveis à atenção primária à saúde em uma unidade de Pronto Atendimento | 2019 |
| 13. | Lilacs | Bordignon et al. | Análise das internações por condições sensíveis à atenção primária no Oeste de Santa Catarina | 2017 |
| 14. | Lilacs | Pereira et al. | Estratégia Saúde da Família no município do Rio de Janeiro: Avaliação da cobertura e internações por condições cardiovasculares | 2018 |
| 15. | Lilacs | Zarlotti et al. | Internações por condições sensíveis à atenção primária após a implantação da estratégia saúde da família no município de Petrópolis/RJ | 2017 |
| 16. | Lilacs | Oliveira et al. | Internações por condições sensíveis à atenção primária em Minas Gerais, entre 1999 e 2007 | 2017 |
| 17. | Lilacs | SOUZA, Dayane Kelle; PEIXOTO, Sérgio Viana. | Estudo descritivo da evolução dos gastos com internações hospitalares por condições sensíveis à atenção primária no Brasil, 2000-2013 | 2017 |
| 18. | Lilacs | Costa et al. | Tendências das internações por condições sensíveis à atenção primária e fatores associados em Porto Alegre, RS, Brasil | 2016 |
| 19. | Lilacs | Sales et al. | Internações hospitalares por condições sensíveis à atenção primária à saúde | 2019 |
| 20. | Medline | Castro et al. | Condições socioeconômicas, oferta de médicos e internações por condições sensíveis à atenção primária em grandes municípios do Brasil | 2015 |
| 21. | Medline | Carneiro et al. | Tecobé no Marajó: tendência de indicadores de monitoramento da atenção primária antes e durante o Programa Mais Médicos para o Brasil | 2018 |
| 22. | Medline | Araujo et al. | Estrutura e processo de trabalho na atenção primária e internações por condições sensíveis | 2017 |
| 23. | Medline | Lôbo et al. | Internações por condições sensíveis à atenção primária de menores de um ano, de 2018 a 2014, no estado de São Paulo, Brasil | 2019 |
| 24. | Medline | Pinto et al. | Internações por condições sensíveis à atenção primária (ICSAP) no Distrito Federal: comparação com outras capitais brasileiras no período de 2009 a 2018 | 2019 |
| 25. | Medline | Silva et al. | Tendências das internações por condições cardiovasculares sensíveis à atenção primária à saúde no município de Senador Canedo, Goiás, 2001-2016 | 2019 |
| 26. | Medline | PINTO, Luiz Felipe; GIOVANELLA, Ligia. | Do programa à Estratégia Saúde da Família: expansão do acesso e redução das internações por condições sensíveis à atenção básica (ICSAB) | 2018 |
| 27. | Medline | Junior et al. | Efeitos da Estratégia Saúde da Família nas internações sensíveis à atenção primária em menores de um ano na Bahia, Brasil | 2018 |
| 28. | Medline | Cavalcante et al. | Internações por condições sensíveis à atenção primária: estudo de validade do SIH/SUS em hospital do Distrito Federal, Brasil, 2012 | 2016 |
| 29. | Medline | Costa et al. | Hospitalização por condições sensíveis à atenção primária em Pelotas: 1998 a 2012 | 2017 |
| 30. | Medline | Junior et al. | Tendências dos gastos e das internações por condições sensíveis à atenção primária em menores de cinco anos na Bahia, Brasil | 2018 |
| 31. | Medline | MORIMOTO, Tissiani; COSTA, Juvenal Soares Dias da. | Internações por condições sensíveis à atenção primária, gastos com saúde e Estratégia Saúde da Família: uma análise de tendência | 2017 |
| 32. | Medline | Rodrigues et al. | Tendência das internações e da mortalidade de idosos por condições sensíveis à atenção primária | 2019 |
| 33. | Medline | Souza et al. | Relações entre a atenção primária e as internações por condições sensíveis em um hospital universitário | 2018 |
| 34. | Medline | BOTELHO, Janaina Fujardo; PORTELA, Margareth Crisóstomo. | Risco de interpretação falaciosa das internações por condições sensíveis à atenção primária em contextos locais, Itaboraí, Rio de Janeiro, Brasil, 2006-2011 | 2017 |
| 35. | Medline | Gonçalves et al. | Programa Mais Médicos no Nordeste: avaliação das internações por condições sensíveis à atenção primária à saúde | 2016 |
| 36. | Scielo | MAGALHÃES, Alessandra Leonardo Alvares; MORAIS NETO, Otaliba Libânio de. | Desigualdades intraurbanas de taxas de internações por condições sensíveis à atenção primária na região central do Brasil | 2017 |
| 37. | Scielo | Caldart et al. | Fatores associados à pneumonia em crianças Yanomami internadas por condições sensíveis à atenção primária na região norte do Brasil | 2016 |
| 38. | Scielo | Santos et al. | Internações por condições sensíveis à atenção primária à saúde em população idosa no estado do Rio Grande do Norte, Brasil, no período de 2008 a 2016 | 2019 |
| 39. | Scielo | Pitilin et al. | Internações sensíveis à atenção primária específicas de mulheres | 2015 |
Source: Authors, 2020.
It is observed in the selected studies that in all five years of the studied period there were works involving the analyzed theme, with the year 2015 comprising 7.69% of the sample (3 articles), 2016: 17.94% (7 articles), 2017: 33.33% (13 articles), 2018 and 2019, with 20.51% (8 articles in each year). The sample data analyzed periods between 1998 and 2018, thus encompassing evidence-based scientific data that comprised 20 years of work on public health policies involving the ICSAP indicator Information described in Table – II.
Different age groups were found, reaching children under one year old, adolescents, 60 years old or more, and 35.89% (14 articles) of the sample indicated age group as the cut-off for analysis (Table – II). In the present study, it was possible to identify that 12.82% (5 articles), of the entire sample analyzed, support the hypothesis that extremes of age have a greater number of hospitalizations. 25.64% (10 articles) showed that men were the highest percentage of ICSAP and 12.85% (5 articles) indicated that they were female. 2.56% (one article) indicated no difference between the sexes; 5.12% (two articles) indicate that there is a gender difference in the prevalence of each sensitive disease.
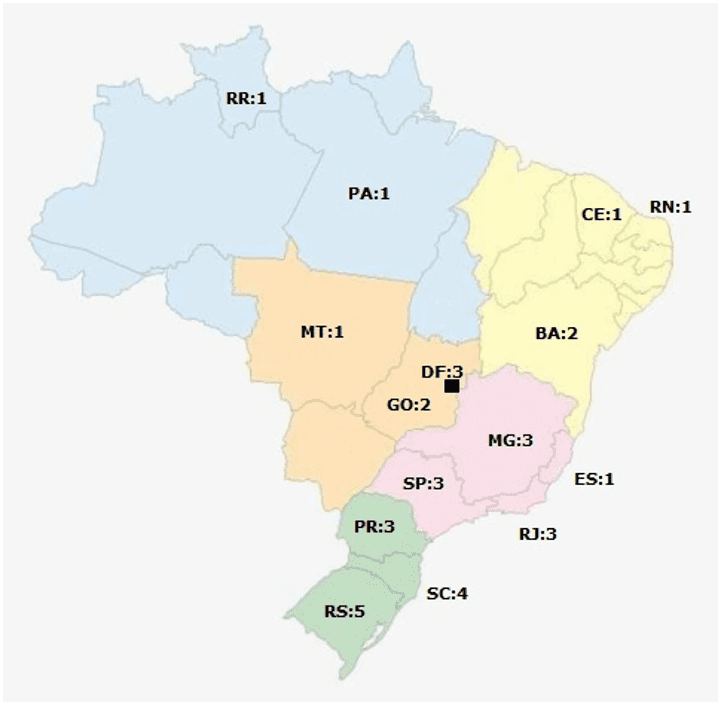
The distribution of the works in the national territory was also expressive, with 10.25% of the studies (4 articles) having national coverage. The sample presents studies carried out in all geoeconomic regions of Brazil, with the South region with 30.76% (12 articles) of the works, the Southeast with 25.64% (10 articles), the Midwest with 15.38% (6 articles), Northeast with 12.82% (5 articles) and North with 5.12% (2 articles), as can be seen in Figure 1. The sample comprises 33.33% of works at the municipal level; 28.20% at the state level; 7.69% Federal District; 2.56% working data at a regional level and 10.25% at a national level, with the other studies (17.94%) involving specific conditions such as: hospital, emergency care unit, health microregions, archipelago and indigenous population of a given region (Table – II).
Table II – Study period, Age Group, Geographical Scope.
| N.º | Study period | Age Group | Geographic Scope |
| 1. | 2010 to 2014 | 10 to 19 years | Health Region (RS) |
| 2. | 2000 to 2012 | 60 to 74 years | State |
| 3. | 2000 to 2014 | State | |
| 4. | 2000 to 2010 | Under 5 years old | State |
| 5. | 1998 to 2012 | Municipal | |
| 6. | 2001 to 2011 | Municipal | |
| 7. | 2008 to 2017 | 0 to 9 years | Hospital Regional |
| 8. | 2007 to 2011 | Under 5 years old | Municipal |
| 9. | 2012 | Under 5 years old | State |
| 10. | 2008 | Health microregion of the city of São Paulo | |
| 11. | 1998 to 2007 | Municipal | |
| 12. | 2015 to 2016 | Emergency care unit | |
| 13. | 2008 to 2013 | West Region of Santa Catarina | |
| 14. | 2008 to 2013 | Municipal | |
| 15. | 1999 to 2013 | Municipal | |
| 16. | 1999 to 2007 | State | |
| 17. | 2000, 2005, 2010, 2013 | National | |
| 18. | 1998 to 2012 | Municipal | |
| 19. | 2008 to 201 | State | |
| 20. | 1998 to 2012 | National | |
| 21. | 2011 to 2015 | Marajó Archipelago | |
| 22. | 2012 to 2014 | National | |
| 23. | 2008 to 2014 | Under 1 year old | State |
| 24. | 2009 to 2018 | Federal District | |
| 25. | 2001 to 2016 | 30 to 69 years | Municipal |
| 26. | 2001 to 2016 | National | |
| 27. | 2000 to 2012 | Under 1 year old | State |
| 28. | 2012 | Federal District Hospital | |
| 29. | 1998 to 2012 | Under 1 year old | National |
| 30. | 2000 to 2012 | Under 5 years old | State |
| 31. | 2003 to 2012 | Municipal | |
| 32. | 2008 to 2012 | Seniors (60 years and over) | State |
| 33. | March a June de 2016 | 18 years or older | Hospital Universitário |
| 34. | 2006 to 2011 | Municipal | |
| 35. | September of 2012 of August of 2015 | Northeast Region | |
| 36. | 2008 to 2013 | Municipal | |
| 37. | 2011 to 2012 | Children between 0.1 and 59.9 months | Indigenous population of the North Region |
| 38. | 2008 to 2016 | Seniors (60 years and over) | State |
| 39. | March to June of 2013 | 14 years or older | Municipal |
Source: Authors, 2020.
Figure 1 – Georeferencing of studies in Brazil.
Regarding the specific theme of scientific works, there were different approaches, however, with 84.61% of the productions in line with the Brazilian List of Sensitive Conditions for Primary Care. 92.30% of the articles used secondary data (Table III), such as data from the Hospital Information System (HIS), Inpatient Hospital Authorization (IHS), medical records, data from the Brazilian Institute of Geography (IBGE), Information System Primary Care (SIAB), among others; and 7.69% used a mixed form between secondary data and primary data collected through interviews, questionnaires and assessment instruments.
Of this sample, 64.10% (25 articles) used an ecological study design; 10.25% (4 articles) descriptive; 7.69% (3 articles) cross-sectional; 5.12% (2 articles) qualitative; 5.12% (2 articles) epidemiological; 5.12% (2 articles) regressive and 2.56% (one article) sectional. As can be seen in Table – III.
Table III – Study design, Data source, LBCSAP Citation.
| N.º | Study design | Data source | Quote the LBCSAP |
| 1. | Ecological Retrospective | Secondary | Yes |
| 2. | Ecological | Secondary | Yes |
| 3. | Time series ecological | Secondary | Yes |
| 4. | Time series ecological | Secondary | Yes |
| 5. | Ecological | Secondary | Yes |
| 6. | Ecological | Secondary | Yes |
| 7. | Exploratory ecological | Secondary | Yes |
| 8. | Descriptive | Secondary | Yes |
| 9. | Descriptive | Secondary | Yes |
| 10. | Qualitative | Mixed | No |
| 11. | Ecological | Secondary | Yes |
| 12. | Ecological Exploratory Description | Secondary | Yes |
| 13. | Descriptive | Secondary | No |
| 14. | Cross-sectional Epidemiological | Secondary | Yes |
| 15. | Ecological | Secondary | Yes |
| 16. | Ecological | Secondary | Yes |
| 17. | Descriptive | Secondary | Yes |
| 18. | Ecological | Secondary | Yes |
| 19. | Time series ecological | Secondary | No |
| 20. | Descriptive analysis and cross-sectional study | Secondary | Yes |
| 21. | Linear regression model, time series | Secondary | Yes |
| 22. | Ecological | Secondary | No |
| 23. | Ecological | Secondary | Yes |
| 24. | Ecological | Secondary | No |
| 25. | Ecological | Secondary | No |
| 26. | Time series ecological | Secondary | Yes |
| 27. | Longitudinal ecological | Secondary | Yes |
| 28. | Descriptive epidemiological and criterion validation study | Secondary | Yes |
| 29. | Ecological | Secondary | Yes |
| 30. | Ecological | Secondary | Yes |
| 31. | Time series ecological | Secondary | Yes |
| 32. | Time series ecological | Secondary | Yes |
| 33. | Transversal seccional | Mixed | Yes |
| 34. | Logistic regression model | Secondary | Yes |
| 35. | Exploratory, evaluative | Secondary | Yes |
| 36. | Ecological | Secondary | Yes |
| 37. | Observational epidemiological | Secondary | Yes |
| 38. | Ecological | Secondary | Yes |
| 39. | Sectional study | Mixed | Yes |
Source: Authors, 2020.
Regarding the rates of ICSAP indicated in the total sample, it was possible to assess that 89.74% of the scientific works presented rates of ICSAP; of this universe, 45.71% (16 articles) indicated a reduction in the rates of ICSAP during the study period, and in some articles of this percentage, stability or increase in specific sample cuts is also indicated; 14.28% (5 articles) indicated stability in the rates and 5.71% (two articles) indicated an increase in ICSAP. 16 studies (45.71%) reported only the percentage of ICSAP in relation to the total number of hospitalizations, with this percentage varying from 17.1% to 93% when in hospitalized Yanomami children. 25.71% of this sample indicates that ICSAP continues to have high rates.
Addressing the correlation between access to health and ESF coverage with rates of ICSAP, which is very evident in the Brazilian literature, 84.61% (33 articles) of the total sample mentioned this association. Of this universe, 45.45% (15 articles) highlighted a negative correlation between ICSAP and the coverage of the Family Health Strategy (ESF); 33.33% (11 articles) included as a research objective (Table – IV) the assessment of the correlation of access and coverage of the ESF with the ICSAP; 15.15% (5 articles) did not indicate a significant correlation; 3.03% (one article) indicated the presence of higher rates of ICSAP with the presence of PHC care. Since 84.84% (28 articles) explain that the increase in ESF coverage is not the only factor influencing ICSAP.
It is also found in the literature, association of rates of ICSAP with health expenditures, whether hospital care expenditures, at the primary care level, or expenditures as a whole. 33.33% (13 articles) of the total sample of the review addressed this correlation, and from this universe, 61.53% (8 articles) included the evaluation of the correlation between expenditures and ICSAP as the objective of the study (Table – IV).
Regarding the determining and conditioning factors of health. It was identified that 82.05% (32 articles), of the total sample of studies, indicate the influence of associated factors, determinants and social determinants of health, with the outcome of hospitalization for ACSC; and only 15.62% (5 articles) of this universe include as a study objective (Table – IV) associated factors that determine or influence the occurrence of these hospitalizations. Among these, socioeconomic and sociodemographic variables were mentioned, as well as education, self-care, emotional and psychological issues, gender, age group, marital status, cultural characteristics, among others.
Regarding the relationship between communication and organization of the health care network, it is possible to assess that only 7.69% of the total sample, three articles, had as their central focus of the study (Table – IV), an issue related to the dynamics of the network of health care, team work processes and their communication.
Table IV – Objectives of the studies of the evaluated sample.
| N.º | Objective |
| 1. | To analyze hospitalizations due to conditions sensitive to Primary Care of adolescents in the second health region of Paraná from 2010 to 2014. |
| 2. | To analyze Hospitalizations for Sensitive Conditions to Primary Care (ICSAP) in the elderly by causes and coverage of the Family Health Strategy (ESF). |
| 3. | To describe the time series of hospitalizations for conditions sensitive to primary care (ICSAP) in the state of Espírito Santo, from 2000 to 2014, according to sex, age group, municipal size, macro-regions and cause groups, and to investigate the factors associated with the occurrence of these hospitalizations. |
| 4. | To analyze the temporal trend and describe the causes of Hospitalizations for Conditions Sensitive to Primary Care (ICSAP) in children under five years of age in Ceará, Brazil, in 2000-2012. |
| 5. | To analyze the trend of hospitalizations for conditions sensitive to primary care (ICSAP) in Novo Hamburgo, comparing it with the rest of the State of Rio Grande do Sul, and relating it to financial investments in health and coverage of the Family Health Strategy (ESF) in the municipality, from 1998 to 2012. |
| 6. | To evaluate the trend of hospitalization rates for conditions sensitive to primary care (ICSAP) in the city of Florianópolis, Santa Catarina, Brazil, from 2001 to 2011, and to verify its correlation with financial investment in health and population coverage by the Health Strategy of the Family (ESF). |
| 7. | To characterize the hospitalizations of children aged zero to nine years due to conditions sensitive to primary care, in a regional hospital in the Federal District, between 2008 and 2017. |
| 8. | To characterize the hospitalizations of children under five years of age due to conditions sensitive to primary care, in Cuiabá, Mato Grosso, between 2007 and 2011. |
| 9. | To describe the proportions and rates of hospitalization for Primary Care Sensitive Conditions (CSAP) in children under 5 years of age in the state of Santa Catarina, Brazil, in 2012. |
| 10. | Understand the reasons that determine or influence the occurrence of ICSAP from the point of view of users and professionals of Primary Care. |
| 11. | Correlate the rates of hospitalizations due to Conditions Sensitive to Primary Care and the implementation of the Family Health Strategy in the city of Passo Fundo, Rio Grande do Sul, from 1998 to 2007, evaluating hospital admissions for preventable causes. |
| 12. | To describe care for sensitive conditions in primary care in an emergency care unit. |
| 13. | To analyze the records of Hospitalizations for Sensitive Conditions to Primary Care in 25 municipalities in the western region of Santa Catarina. |
| 14. | To evaluate the coverage of the Family Health Strategy in the city of Rio de Janeiro from 2008 to 2013, and to verify its correlation with hospitalizations for cardiovascular diseases sensitive to Primary Care. |
| 15. | Quantify hospitalizations for conditions sensitive to primary care (ICSAP), comparing them with the gross rate of hospitalizations and analyze their frequency with the coverage of the Family Health Program (PSF) in Petrópolis/RJ. |
| 16. | To analyze the rates of Hospitalizations for Sensitive Conditions to Primary Care in the health regions of Minas Gerais, from 1999 to 2007. |
| 17. | To analyze the proportions of expenses with hospitalizations for conditions sensitive to primary care (ICSAP) in relation to the total expenses with hospitalizations financed by the Unified Health System (SUS) in Brazil, in 2000, 2005, 2010 and 2013, according to sex, age group and groups of causes. |
| 18. | To analyze the trend of ICSAP relating them to financial investments in health and ESF coverage in the city of Porto Alegre, Rio Grande do Sul, from 1998 to 2012. |
| 19. | To analyze hospital admissions due to conditions sensitive to Primary Health Care (PHC) in the state of Minas Gerais. |
| 20. | To analyze the variables associated with the occurrence of hospitalizations for conditions sensitive to primary health care in Brazilian municipalities with a population of over 50 thousand inhabitants, separately by the five major regions of the country. |
| 21. | To evaluate the performance of the Family Health Strategy after the implementation of the Mais Médicos Program (PMMB) in the territory of Marajó-PA-Brazil, through the historical series of four primary care indicators in the period 2011-2015: population coverage, proportion of live births of mothers for prenatal consultations, hospitalization rates due to a condition sensitive to primary care (ICSAP) and infant mortality rate. |
| 22. | To investigate whether characteristics of the structure of basic health units and the work process of primary care teams are associated with the number of hospitalizations due to conditions sensitive to primary care. |
| 23. | To describe the causes and trends of Hospitalizations for Conditions Sensitive to Primary Care (ICSAP) in children under one year old, between 2008 and 2014, in the state of São Paulo, Brazil. |
| 24. | Compare with the last decade, standardized rates of hospitalizations for conditions sensitive to primary health care (ICSAP) in the Federal District (DF), comparing them with selected capitals, age groups and ICSAP groups. |
| 25. | To analyze the trend of hospitalization rates for cardiovascular conditions sensitive to primary health care (CCSAP). |
| 26. | To evaluate the effects of the implementation of the Family Health Strategy over the last two decades in Brazil, demonstrating the access provided and the trend of hospitalizations for sensitive conditions in primary care (ICSAB). |
| 27. | To evaluate the effect of expanding the coverage of the Family Health Strategy (ESF) on hospitalizations for conditions sensitive to primary care (ICSAP) in children under one year of age. |
| 28. | To describe hospitalizations for conditions sensitive to primary care, with an emphasis on DIP, and to validate the HIS/SUS, regarding the registration of hospitalizations for these conditions, at the Hospital Regional do Paranoá, Distrito Federal, Brazil, in 2012. |
| 29. | To verify the trend of hospitalization rates for conditions sensitive to primary care in the city of Pelotas, Rio Grande do Sul, from 1998 to 2012. |
| 30. | To analyze the trend of Hospitalizations for Sensitive Conditions to Primary Care and the expenses with these hospitalizations in children under five years old residing in Bahia, from 2000 to 2012. |
| 31. | To analyze the temporal trend of hospitalizations for conditions sensitive to primary care (ICSAP), relating it to health expenditures and the coverage of the Family Health Strategy (ESF), in the city of São Leopoldo, Rio Grande do Sul, in the period from 2003 to 2012. |
| 32. | To analyze the trend of hospitalization and mortality rates of the elderly due to conditions sensitive to primary care (CSAP) in the state of Santa Catarina, Brazil, from 2008 to 2015. |
| 33. | To analyze the relationships between the presence and orientation of Primary Health Care and hospitalizations for conditions sensitive to primary care in a university hospital. |
| 34. | To characterize hospitalizations for conditions sensitive to primary care (ICSAP), identify associated factors and explore the impact on them of the closure of a hospital, among residents of Itaboraí, a municipality with high rates of ICSAP in the State of Rio de Janeiro, Brazil, feeding the debate on the indiscriminate use of the indicator for inferences about the expansion and quality of primary care. |
| 35. | To evaluate the Mais Médicos Program in the Northeast Region, using hospitalizations for CSAP as an indicator of the effectiveness of the ESF, contextualizing them by the ratio of doctors per 10,000 inhabitants in the federative units. |
| 36. | To evaluate the rates of ICSAP and the causes in the intra-urban areas of the city of Goiânia-Goiás. |
| 37. | To analyze factors associated with pneumonia in Yanomami children hospitalized for conditions sensitive to primary care (ICSAP). |
| 38. | To identify hospital admissions due to conditions sensitive to primary health care (ICSAP) in the elderly in the state of Rio Grande do Norte (RN), Brazil. |
| 39. | To analyze hospitalizations for specific primary care sensitive conditions (ICSAP) in women and the factors that determine or influence the occurrence of these hospitalizations (socioeconomic, sociodemographic factors and health control). |
Source: Authors, 2020.
4. DISCUSSION
Studies on hospitalizations for conditions sensitive to primary care, as we have seen, showed, in 84.61% of the sample, adequacy with the List of Conditions Sensitive to Primary Care (LBCSAP); Morimoto and Costa (2017), Costa et al. (2016) and Arruda and Costa (2017) emphasize that the creation of the LBCSAP allows comparability between national studies, contributing to the improvement and consolidation of the indicator in the country. On the other hand, Santa et al. (2016) point out that “the LBCSAP is only partially used to evaluate PHC, because in fact it is better for evaluating the health care network”.
Another trend identified is the use of secondary data, mainly from the Hospital Information System (HIS), in 92.30% of the studies evaluated. Carneiro et al. (2018) point out that the use of this type of data enables information on health conditions relatively quickly, with wide access and low cost.
The analysis of hospitalizations registered in the HIS also has the advantage of wide coverage of approximately 70% of hospitalizations in the country, as it only represents hospitalizations carried out in the public network of services managed or contracted to SUS. It should be noted that these studies are based on data from hospitalization episodes, not on individuals, the event being the object of the HIS record (ZARLOTTI et al., 2017; PEREIRA et al., 2018; MARIANO; NEDEL, 2018).
The trend of association between the decrease in ICSAP rates with a view to implementing the ESF and the increase in coverage in recent years can be verified by the large expansion in the number of Family Health teams in the last twenty years (TAGLIARI et al., 2016; PINTO; GIOVANELLA, 2018). Even though there are still numerous problems in the quality of healthcare and insufficient development of PHC attributes, the expansion of coverage was accompanied by a set of converging public health policy actions that sought to qualify the care processes in PHC (PINTO; GIOVANELLA, 2018). However, expanding access alone does not guarantee the performance and effectiveness of the care provided (TAGLIARI et al., 2016).
Several transformations during the construction of the SUS have stimulated the reduction of ICSAP in several locations in the country (COSTA et al., 2016). It should be noted that Brazil’s continental dimension and complexity make it difficult to implement standards of a generalized nature. Thus, the ESF must focus on promoting equity and not abdicating integrality, in line with providing a greater possibility of qualified care to the population (PEREIRA et al., 2018).
Such evidence is associated with that established by the Ministry of Health (MS), which recommends that, for the consolidation stage of the Programa de Expansão e Consolidação Saúde da Família (PROESF)[6], there must be 60% coverage for cities with a population size of 100,000 to 500,000 inhabitants and 50% coverage in municipalities between 500,000 and 2,000,000 inhabitants (MORIMOTO; COSTA, 2017; COSTA et al., 2016).
These indications reinforce the MS’s assumption that the ESF is a strategy for reorganizing the care model, which is structured through the treatment of the population as a subject integrated into the family, household and community, aimed at increasing the network’s problem-solving capacity, promoted through intersectoral actions, linking professionals and services with the community (TAGLIARI et al., 2016). Therefore, care is needed in interpreting the association between the reduction of ICSAP and the process of expanding the ESF. It is essential to observe contextual issues that can converge to explain the event (BOTELHO; PORTELA, 2017).
Botelho and Portela (2017) point out that “the use of the indicator for inferences about the expansion and quality of care cannot do without the consideration of factors related to the organization and practices of health services”. Thus, the improvement of health indicators in recent years is a consequence of complex processes and a set of social policies combined with the expansion of the ESF (PINTO; GIOVANELLA, 2018). Souza et al. (2018) indicate that there is a strong current that points out that the reduction in hospitalizations is associated with the quality of PHC actions and not merely its presence.
Another important point to be analyzed is health financing, as ensuring access to health does not only presuppose the removal of physical obstacles, but the obtaining of adequate services and resources (MORIMOTO; COSTA, 2017). And, despite the mentioned decrease in ICSAP, expenses with sensitive hospitalizations are still significantly high, and these expenses are relevant for the health system (SALES et al., 2019).
Santos et al. (2019) in a study carried out in Rio Grande do Norte, point out that although the rates of ICSAP have reduced over time, the average number of days of stay and the average amount spent per hospitalization has increased. They point out that in order for us to have lower expenses with hospitalizations, it is important to act in the development of actions that go beyond the curative model and advance in the construction of a care model focused on prevention and health promotion.
We can say that the reduction of sensitive hospitalizations is a strategic issue in the face of insufficient resources, managing to represent savings and reinvestment in the sector that coordinates health care (CAMELO; REHEM, 2019). This is justified because, as described by Costa et al. (2017), health financing has been considered a crucial issue in the consolidation of the SUS. Health expenditures have historically been insufficient and the disparity between levels of care affects primary care much more. In Brazil, federal spending on PHC was 21.0%, and this level of care is responsible for meeting up to 80% of health demands (MORIMOTO; COSTA, 2017).
Thus, cost-effective actions aimed at disease prevention and control constitute an activity with great potential to reduce ICSAP, thus promoting less suffering for users and their families, in addition to allowing a reduction in expenses in the entire health care network (CARNEIRO et al., 2018). Junior et al. (2018) point out that, in addition to the financial impact, it is also necessary to consider the psychological and social damage inseparable from the hospitalization of people deprived of adequate assistance at the primary care level. In this way, the ICSAP indicator is useful in the situational diagnosis, supporting action programs and the correct application of resources (PAZÓ et al., 2017).
The reduction of hospitalizations for sensitive conditions, with the maintenance of a high degree, can translate into the complexity of the social determinants of health, indicating the concentration of professionals, which should also be thought of according to the characteristics of the epidemiological profile of states and municipalities. Differences in the occurrence of ICSAP may indicate particularities regarding social, economic and environmental determinants of health and, especially, characteristics of health care (GONÇALVES et al., 2016).
Castro et al. (2015) state that factors related to socioeconomic and demographic conditions, offer of services and professionals were associated with the proportion of sensitive hospitalizations, in a differentiated way between the regions of the country. These differences reveal the importance, in addition to biological characteristics, of factors such as “education, work, family income, economic development of the region, that is, the economic and social conditions in which they live” (FREITAS et al., 2018). The lack of approximation with social determinants of health such as education, income, leisure, housing conditions, acts as an exogenous factor that contributes to the increase in hospitalization rates (PITILIN et al., 2015).
In a study on the panorama of ICSAP in Espírito Santo, Pazó et al. (2017) corroborate that each increase in the Gini index, which shows the increase in inequality, was accompanied by an increase in the risk of hospitalization, with a higher risk of ACSC associated with a worsening of the Human Development Index (HDI).Although the health advances seen in Brazil, old challenges remain, such as the effective change in the care model, with improvements in the quality and effectiveness of actions, as well as challenges that transcend the health sector, such as, for example, investment in infrastructure and reduction of social inequalities (CASTRO et al., 2015).
We show that ICSAP harm both the health system, the individual and society, causing psychosocial, psychobiological and economic damage (SOUZA et al., 2018). The need for improvement in the PHC structure is even higher as ICSAP are often in consortium with chronic diseases, considering that many of these are part of PHC-sensitive conditions. As a fundamental aspect for welcoming users with chronic conditions, the incorporation of the self-care strategy supported by the work process of the teams. For this, it is necessary to emphasize the central role of the user in managing their own health (SANTA et al., 2016).
Freitas et al. (2018) point out that the processes that determine the subjects’ visit to the health service are related to social, economic and cultural factors. Thus, knowing the determination of the health-disease process can support the elaboration of interventions that aim to change the health reality found in the population and allow the implementation of intersectoral interventions that understand the population’s needs.
In order for the health network to be successful, some challenges need to be overcome, highlighting the adequate qualification of professionals, meeting an organized demand from the perspective of comprehensive care, which implies an organized reference and counter-reference system (TAGLIARI et al., 2016). Souza et al. (2018) tell us that the lack of an effectively organized referral and counter-referral system seems to contribute to unnecessary hospitalizations.
Great efforts seek ways to assist in the evaluation of the performance of the health system in order to enable and implement public policies, humanize care and reduce sensitive hospitalizations (RODRIGUES et al., 2019). The organization of the integrated health care system, in the configuration of Health Care Networks (RAS), organized through an integrated, polyarchic network, of continuous assistance to a defined population, must maintain fluid communication with all levels of care and position itself in opposition to the hegemonic, fragmented, pyramidal system of isolated points and without communication with each other (SANTA et al., 2016).
The organization of the health network is fundamental as it ensures the continuity of care at other levels of care, being articulated in flows and circuits, by the various knowledge of a multidisciplinary team. Because, by reorganizing the work process, with a multi-professional team as the axis, we enable the growth of the number of visits and the quality of the health system (SANTA et al., 2016).
Araújo et al. (2017), in a study carried out on the structure and work process in PHC and ICSAP, demonstrate that of the characteristics of the work process, the ESF receiving matrix support was the only variable that showed a direct association with the outcome of ICSAP. The authors suggest that PHC quality should be invested in the organization of the work process. In this sense, Pereira et al. (2018) indicate that professionals must have a diversified and complex arsenal of technological resources, and interventions go beyond curative, biological practices. This is one of the great challenges in promoting quality and comprehensive care to the population, with the PHC coordinating the network.
In this way, prioritizing the planning and development of intersectoral actions, qualified listening, referral to resolve necessary demands, accountability and bonding with the assisted population, conceptualizes the service and increases resolution (CARNEIRO et al., 2018). Sales et al. (2019) say that the reduction in the number of ICSAP is the representation of the organization of the health system, however these numbers did not decrease even more because the health services find it difficult to work in an integrated way.
Studies based on secondary data, such as data from the HIS, have recognized limitations as they are susceptible to possible instability or quality bias (BORDIGNON et al., 2017). The HIS, an information system powered by Inpatient Hospital Authorization (IHA), goes through problems such as the chance of underreporting, misclassification of diagnosis of hospitalization, impossibility of distinguishing between readmissions or hospital transfers, offering only the main diagnosis, imprecision of the data on the municipality of origin, which limits the verification of the basic health unit of origin (CAMELO; REHEM, 2019; ZARLOTTI et al., 2017; SOUZA; PEIXOTO, 2017).
It is current in the national literature, as pointed out by Magalhães and Morais Neto (2017), in a study on intra-urban inequalities in ICSAP rates, that the use of data from the HIS has the limitation of using data that are aimed at the billing of hospitalizations, financed by the SUS, thus tending to record more expensive procedures, hiding ICSAP occurrences. Despite this, since the creation of the SUS, there has been a recognized advance in system audits, which may have minimized the problem (PITILIN et al., 2015; MARIANO; NEDEL, 2018).
Such limitations require caution in interpretation and that the denominators used to calculate the coefficients are the populations effectively exposed to the risk of hospitalization. Caldart et al. (2016) point out that, even if the HIS provides a restricted collection of information on socioeconomic conditions, clinical and demographic characteristics; employing a search strategy for complementary data helps to identify factors associated with hospitalization. Pinto Junior et al. (2018) indicate that, even with limitations, there is a substantial body of scientific evidence that warns of consistency in the use of HIS, presence of improvements and expansion in its use in research in the field of public health (TAGLIARI et al., 2016).
5. FINAL CONSIDERATIONS
The studies evaluated showed that the ICSAP are strongly related to determining factors and social determinants of health. This theme, along with the organization, communication and articulation/dynamics of the levels of complexity, were the least explored themes as objectives of the sample studies, however they can be seen as an integral part of the advances and the need for improvements to reduce the rates of avoidable hospitalizations and for the correct use of health resources.
Most of the studies in the sample cited the LBCSAP as a reference for the development of the ICSAP indicator in Brazil and for comparability of studies, however, a large number of studies used secondary data to the detriment of the use of complementary strategies that would help to obtain proximal data from the patient and of the care network, which would indicate greater data consistency.
In this way, this integrative review contributes to current discussions, bringing knowledge about the ICSAP theme, coordinating the analysis of independent scientific works. Implying notes for actions, public health policies and the development of new studies. As well as, giving light to the need to form participatory multiprofessional teams that are capable of organizing and articulating Health Care Networks, aiming at the integrality of the subject, to overcome the hegemonic paradigm of health work processes.
REFERENCES
AVELINO, C. C. V. et al. Qualidade da atenção primária à saúde: uma análise segundo as internações evitáveis em um município de Minas Gerais, Brasil. Ciênc. saúde coletiva, Rio de Janeiro, v. 20, n. 4, p. 1285-1293.
ALFRADIQUE, M. E. et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP – Brasil). Cad. Saúde Pública, Rio de Janeiro, v. 25, n. 6, p. 1337-1349, 2009.
ARRUDA, J. S. de; COSTA, J. S. D. da. Internações por condições sensíveis à atenção primária em Novo Hamburgo, Rio Grande do Sul. Revista Brasileira de Medicina de Família e Comunidade, Rio de Janeiro, v. 12, n. 39, p. 1-11, 2017.
ARAUJO, W. R. M. et al. Estrutura e processo de trabalho na atenção primária e internações por condições sensíveis. Rev. Saúde Pública, São Paulo, v. 51, 75, 2017.
BORDIGNON, M. et al. Análise das internações por condições sensíveis à atenção primária no oeste de Santa Catarina. Revista Baiana de Saúde Pública. v. 41, n. 2, p. 410-423. 2017.
BORDIGNON, M. et al. ANÁLISE DAS INTERNAÇÕES POR CONDIÇÕES SENSÍVEIS À ATENÇÃO PRIMÁRIA NO OESTE DE SANTA CATARINA. Revista Baiana de Saúde Pública, [S.l.], v. 41, n. 2, 2018.
BOTELHO, J. F.; PORTELA, M. C. Risco de interpretação falaciosa das internações por condições sensíveis à atenção primária em contextos locais, Itaboraí, Rio de Janeiro, Brasil, 2006-2011. Cad. Saúde Pública, Rio de Janeiro, v. 33, n. 3, e 00050915, 2017.
CAMELO, M. S.; REHEM, T. C. M. S. B. Internações por condições sensíveis à atenção primária em pediatria no Distrito Federal: Um estudo ecológico exploratório. REME – Rev.Min.Enferm. 23: e-1269, 2019.
CALDART, R. V. et al. Fatores associados à pneumonia em crianças Yanomami internadas por condições sensíveis à atenção primária na região norte do Brasil. Ciênc. saúde coletiva, Rio de Janeiro, v. 21, n. 5, p. 1597-1606, 2016.
COSTA, J. S. D. da et al. Hospitalizações por condições sensíveis à atenção primária em Pelotas: 1998 a 2012. Rev. bras. epidemiol., São Paulo, v. 20, n. 2, p. 345-354, 2017.
COSTA, J. S. D. da et al. Tendência das internações por condição sensível à atenção primária e fatores associados em Porto Alegre, RS, Brasil. Ciênc. saúde coletiva, Rio de Janeiro, v. 21, n. 4, p. 1289-1296, 2016.
COSTA, J. P. et al. Resolubilidade do cuidado na atenção primária: articulação multiprofissional e rede de serviços. Saúde debate, Rio de Janeiro, v. 38, n. 103, p. 733-743, 2014.
CARDOSO, C. S. et al. Contribuição das internações por condições sensíveis à atenção primária no perfil das admissões pelo sistema público de saúde. Rev Panam Salud Publica. v. 34, n. 4, p. 227-234, 2013.
CARNEIRO, V. B. et al. Tecobé no Marajó: tendência de indicadores de monitoramento da atenção primária antes e durante o Programa Mais Médicos para o Brasil. Ciênc. saúde coletiva, Rio de Janeiro, v. 23, n. 7, p. 2413-2422, 2018.
CASTRO, A. L. B. de et al. Condições socioeconômicas, oferta de médicos e internações por condições sensíveis à atenção primária em grandes municípios do Brasil. Cad. Saúde Pública, Rio de Janeiro, v. 31, n. 11, p. 2353-2366, 2015.
DECS/MESH. Descritores em ciências da saúde, 2020. Vocabulário estruturado e multilíngue. Disponível em: <https://decs.bvsalud.org/sobre-o-decs/>. Acesso em: 18 nov. 2020.
FREITAS, J. S. et al. INTERNAÇÕES DE ADOLESCENTES POR CONDIÇÕES SENSÍVEIS À ATENÇÃO PRIMÁRIA EM UMA REGIONAL DE SAÚDE. Cogitare Enfermagem, [S.l.], v. 23, n. 4, 2018.
GONCALVES, R. F. et al. Programa Mais Médicos no Nordeste: avaliação das internações por condições sensíveis à Atenção Primária à Saúde. Ciênc. saúde coletiva, Rio de Janeiro, v. 21, n. 9, p. 2815-2824, 2016.
MALVEZZI, E. Internações por condições sensíveis a atenção primária: revisão qualitativa da literatura científica brasileira. Saúde em Redes. v. 4, n. 4, p. 119-134, 2018.
MENDES, K. D. S.; SILVEIRA, R. C. C. P.; GALVÃO, C. M. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto contexto – enferm., Florianópolis, v. 17, n. 4, p. 758-764, 2008.
MORETTI, P. G. S.; FEDOSSE, E. Núcleos de Apoio à Saúde da Família: impactos nas internações por causas sensíveis à atenção básica. Fisioter. Pesqui., São Paulo, v. 23, n. 3, p. 241-247, 2016.
MALTA, D. C. et al. O SUS e a Política Nacional de Promoção da Saúde: perspectiva resultados, avanços e desafios em tempos de crise. Ciênc. saúde coletiva, Rio de Janeiro, v. 23, n. 6, p. 1799-1809, 2018.
MORIMOTO, T.; COSTA, J. S. D. da. Internações por condições sensíveis à atenção primária, gastos com saúde e Estratégia Saúde da Família: uma análise de tendência. Ciênc. saúde coletiva, Rio de Janeiro. v. 22, n. 3, p. 891-900, 2017.
MAGALHÃES, A. L. A.; MORAIS NETO, O. L. de. Desigualdades intraurbanas de taxas de internações por condições sensíveis à atenção primária na região central do Brasil. Ciênc. saúde coletiva, Rio de Janeiro, v. 22, n. 6, p. 2049-2062, 2017.
MARIANO, T. S. O.; NEDEL, F. B. Hospitalização por Condições Sensíveis à Atenção Primária em menores de cinco anos de idade em Santa Catarina, 2012: estudo descritivo. Epidemiol. Serv. Saúde, Brasília. v. 27, n. 3, e 2017322, 2018.
NUNES, R. P. Estratégia saúde da família e internações por condições sensíveis à atenção primária: uma revisão sistemática. Rev. APS. v. 21, n. 3, p. 450-460. 2018.
NEDEL, F. B. et al. Conceptual and methodological aspects in the study of hospitalizations for ambulatory care sensitive conditions. Ciênc. saúde coletiva, Rio de Janeiro, v. 16, supl. 1, p. 1145-1154, 2011.
NEDEL, F. B. et al. Características da atenção básica associadas ao risco de internar por condições sensíveis à atenção primária: revisão sistemática da literatura. Epidemiol. Serv. Saúde, Brasília. v. 19, n. 1, p. 61-75, 2010.
PAZÓ, R. G. et al. Panorama das internações por condições sensíveis à atenção primária no Espírito Santo, Brasil, 2000 a 2014. Revista Brasileira de Medicina de Família e Comunidade, Rio de Janeiro. v. 12, n. 39, p. 1-12, 2017.
PEREIRA, F. J. R.; SILVA, C. C. da; LIMA NETO, E. A. Condições Sensíveis à Atenção Primária: uma revisão descritiva dos resultados da produção acadêmica brasileira. Saúde debate, Rio de Janeiro. v. 38, n. spe, p. 331-342, 2014.
PEREIRA M. H. B. et al. Estratégia Saúde da Família no Município do Rio de Janeiro: avaliação da cobertura e internações por condições cardiovasculares. Rev Fund Care Online. v. 10, n. 3, p. 605-611, 2018.
PITILIN, E. B. et al. Internações sensíveis à atenção primária específicas de mulheres. Ciênc. saúde coletiva, Rio de Janeiro, v. 20, n. 2, p. 441-448, 2015.
PINTO JUNIOR, E. P. et al. Tendência dos gastos e das internações por condições sensíveis à Atenção Primária em menores de cinco anos na Bahia, Brasil. Ciênc. saúde coletiva, Rio de Janeiro, v. 23, n. 12, p. 4331-4338, 2018.
PINTO JUNIOR, E. P. et al. Efeito da Estratégia Saúde da Família nas internações por condições sensíveis à atenção primária em menores de um ano na Bahia, Brasil. Cad. Saúde Pública, Rio de Janeiro, v. 34, n. 2, e 00133816, 2018.
PINTO, L. F.; GIOVANELLA, L. Do Programa à Estratégia Saúde da Família: expansão do acesso e redução das internações por condições sensíveis à atenção básica (ICSAB). Ciênc. saúde coletiva, Rio de Janeiro, v. 23, n. 6, p. 1903-1914, 2018.
RODRIGUES-BASTOS, R. M. et al. Internações por condições sensíveis à atenção primária em município do sudeste do Brasil. Rev. Assoc. Med. Bras., São Paulo, v. 59, n. 2, p. 120-127, 2013.
REHEM, T. C. M. S. B. et al. Registro das internações por condições sensíveis à atenção primária: validação do sistema de informação hospitalar. Rev. Latino-Am. Enfermagem, Ribeirão Preto, v. 21, n. 5, p. 1159-1164, 2013.
RODRIGUES, M. M.; ALVAREZ, A. M.; RAUCH, K. C. Tendência das internações e da mortalidade de idosos por condições sensíveis à atenção primária. Rev. bras. epidemiol., São Paulo, v. 22, e 190010, 2019.
SANTA, T. C. M. S. et al. Quais aspectos contribuem para a ocorrência de internações por condições sensíveis à atenção primária?. Ver Bras PRomoç Saúde, Fortaleza, v. 29, p. 138-147, 2016.
SALES, K. G. S. et al. Internações hospitalares por condições sensíveis à atenção primária à saúde. Rev Bras Promoç Saúde. 32:9664. 2019.
SOUZA, M. T. de; SILVA, M. D. da; CARVALHO, R. de. Revisão integrativa: o que é e como fazer. Einstein (São Paulo), São Paulo. v. 8, n. 1, p 102-106, 2010
SOUZA, D. K. de; PEIXOTO, S. V. Estudo descritivo da evolução dos gastos com internações hospitalares por condições sensíveis à atenção primária no Brasil, 2000-2013. Epidemiol. Serv. Saúde, Brasília, v. 26, n. 2, p. 285-294, 2017.
SOUZA, L. A. de et al. Relações entre a atenção primária e as internações por condições sensíveis em um hospital universitário. Rev. Gaúcha Enferm., Porto Alegre, v. 39, e 2017-0067, 2018.
SANTOS, K. M. R. dos et al. Internações por condições sensíveis à atenção primária à saúde em população idosa no estado do Rio Grande do Norte, Brasil, no período de 2008 a 2016. Rev. bras. geriatr. gerontol., Rio de Janeiro, v. 22, n. 4, e 180204, 2019.
TAGLIARI, A. B. et al. Impacto da estratégia saúde da família nas internações hospitalares por condições sensíveis à atenção primária. Revista Baiana de Saúde Pública. v. 40, n. 4, p. 876-891, 2016.
ZARLOTTI, C. et al. Internações por condições sensíveis à atenção primária após a implantação da estratégia saúde da família no município de Petrópolis/RJ. Rev Fund Care Online. v. 9, n. 3, p. 811-817. 2017.
APPENDIX – FOOTNOTE
3. Brazilian Family Health Program.
4. Brazilian Family Health Strategy.
5. National Health Promotion Policy in Brazil.
6. Brazilian Family Health Expansion and Consolidation Program.
[1] Psychologist – Graduating from the Multiprofessional Residency Program in Hospital Care.
[2] Doctor in Nursing.
Sent: February, 2021.
Approved: April, 2021.















