ORIGINAL ARTICLE
BORGES, Renato Melo Brazão Pinheiro [1], PIERONI, Thamiris Cunha [2], VELAZQUEZ, Raphaela Kummrow Santos [3], LUZ, Larissa Santos da [4], ALVES, Giovana Carvalho [5], PICANÇO JUNIOR, Olavo Magalhães [6]
BORGES, Renato Melo Brazão Pinheiro. Et al. Analysis of the prevalence of burnout syndrome in surgeons in the state of Amapá, Amazon, Brazil. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year. 07, Ed. 07, Vol. 06, p. 37-62. July 2022. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/burnout-syndrome-in-surgeons, 10.32749/nucleodoconhecimento.com.br/health/burnout-syndrome-in-surgeons
ABSTRACT
Burnout Syndrome (BS), first reported in 1970, appears as a chronic response to interpersonal stressors that occur in the work situation. It is supported by three pillars: Emotional Exhaustion (EE), Depersonalization (DP) and reduced Professional Fulfillment (PF). It usually occurs in individuals whose professions carry relational responsibilities. Physicians are among the most affected, especially surgeons, who need constant attention and dexterity, a factor that predisposes them to excessive stress and psychiatric illnesses. The objective of this study was to analyze the prevalence of Burnout syndrome in surgeons in the state of Amapá, based on the question: What is the prevalence of Burnout syndrome in surgeons working in the state of Amapá? The methodology used was a quantitative and qualitative study, with a situational questionnaire and the Maslach Burnout Inventory Questionnaire (MBI) answered by surgeons in the state of Amapá, between March 2016 and August 2016. The study followed resolutions number 466 of 2012 and number 510 of 2016, of the National Council of Ethics in Research (CONEP). There was a predominance of male surgeons, with a mean age of 42.76 years, most of whom were married or in a stable relationship, who had more than 10 years of medical training and who do not do or do up to 4 night shifts per month. General surgeons were present, in addition to eleven other subspecialties. Regarding the MBI questionnaire, about 25% of those surveyed have a high level of emotional exhaustion, the same number have a high level of depersonalization, and just over 10% have low professional fulfillment. 2.94% have criteria for the diagnosis of Burnout Syndrome. 38.23% showed alteration in at least one of the three spheres. The subspecialties that obtained the worst results were: Vascular Surgery, Oncological Surgery, Neurosurgery and Urology. Thus, although this group has a higher Burnout syndrome rate than the general population, it still has levels lower than those found worldwide.
Keywords: Burnout, Professional burnout, exhaustion Syndrome Professional, Surgeons.
1. INTRODUCTION
According to Nogueira-Martins (2005), illness, suffering, despair and death are situations commonly experienced by medical professionals. Thus, they represent stressing factors inherent to medical work, which permeate both medical education and professional practice. In addition, the anxiogenic nature of the medical task is expressed with maximum intensity, especially in the hospital environment.
The statements made by Nogueira-Martins (2005) are confirmed by the list of the most stressful professions (HSE, 2003), in which the following are listed: doctors, nurses, teachers, police officers and stock market investors; these careers have a higher risk of stress-related pathologies, including psychiatric ones. According to Scott and Hawk (1986), 47% of physicians are screened positive for mental illness, and 29% have clinical symptoms of depression.
In 1970, the New York psychoanalyst Freudenberger first reported the Burnout Syndrome (BS) that would become a silent epidemic of modern society (MASLACH et al., 2001; SPIELBERGER and REHEISER, 2005). Burnout is a psychosocial syndrome that arises as a chronic response to interpersonal stressors that occur in the work situation (MASLACH et al., 2001). BS is supported by three pillars: Emotional exhaustion, Depersonalization and reduced Professional Fulfillment.
Emotional Exhaustion (EE) is the initial trait of the syndrome, and it translates into social isolation, exhaustion of emotional resources, with a feeling of lack of energy, intolerance, irritability, depression, tension and susceptibility to diseases, headaches, nausea, among others (CHERNISS, 1980; WHO, 1998).
In the Depersonalization (DP) dimension, unconscious defense of the emotional charge, there is dehumanization, insensitivity to patients’ problems, negative, skeptical and cynical attitudes are perceived (MOURA et al., 2018).
Low Professional Fulfillment (PF) is the response to the individual’s negative self-assessment, resulting in feelings of incompetence, low esteem, and personal recrimination (MOURA et al., 2018).
BS is also called “careless caregiver syndrome” in allusion to the facts that 1) it occurs in individuals whose professions carry relational responsibilities (health professionals, teachers, police forces and social services), that is, they provide help services; and 2) neglect self-care in terms of health – 70% of physicians do not have regular check-ups (MILLER and MCGOWEN, 2000) and self-medicate.
In contrast to the pillars of BS, several authors describe that improving support for work would reduce the search for individual solutions to the difficulties arising from this work, breaking down the variables that would trigger the syndrome. This would be a protective factor for job satisfaction and a factor in dealing with Burnout (LIMA et al., 2013).
The high level of stress in medical surgeons can lead to serious manifestations such as depression, anxiety, divorces (or breakups), alcoholism, substance abuse and suicide (BALCH et al., 2011).
Lima et al. (2013) in their production highlights as effects of Burnout on health systemic arterial hypertension, myalgia, arthralgia, headache, insomnia, anxiety, irritability, demotivation and deconcentration.
In the meantime, it can be seen that, over time, the professional environment starts to have an increase in the frequency of physicians who prioritize financial and competitive values, overlapping humanistic precepts (LIMA et al., 2013).
The competitive and stressful environment in the medical environment begins with the selection processes for admission to the undergraduate course and lasts during training, becoming even more intense, depending on the chosen medical residency. It is common for resident physicians to report behavioral and organic disorders, such as daytime sleepiness, depression and burnout (FABICHAK et al. 2013). Jarruche and Mucci (2022), in their research with 102 resident physicians, found alarming numbers among those enrolled in general surgery, which corroborates the idea of stress and competitiveness as triggers for Burnout.
In Brazil, Ordinance No. 400 of the Ministry of Health provides for the norms and standards of installation and construction in health services and defines the Surgical Center as “a set of elements intended for surgical activities, as well as anesthetic recovery, and can be considered a complex organization by virtue of its characteristics and specialized assistance”. This ordinance aimed to provide the patient with adequate human and material resources, in order to minimize the risk of complications (MS, 1977).
From this definition, it is inferred that the surgical environment demands constant attention, responsibility and dexterity from surgeons. High expectations originate in this environment, predisposing surgeons to stress and psychiatric illnesses such as, for example, Burnout Syndrome.
Given the above and assuming that researchers work in the medical area of the state, it is inferred the importance of investigating the prevalence of Burnout Syndrome in surgeons in the State of Amapá, in order to identify whether this index is higher or lower than the expected. The question that guided the research was: What is the prevalence of Burnout syndrome in surgeons working in the state of Amapá?
Thus, the objective of this study was to analyze the prevalence of Burnout syndrome in surgeons in the state of Amapá.
2. METHODOLOGY
A quantitative and qualitative study was carried out from October 2015 to November 2016, with the target population consisting of surgeons from the State of Amapá. The only inclusion criterion is that the participants were medical surgeons, residing and working in the state. Surgeons who did not meet the inclusion criteria or who refused or withdrew from participating were excluded from the study.
To calculate the sample size, the criteria established based on the sampling theory of Cochran (1977) were followed, with a sample error of 5% as a reference.
This research followed all the ethical principles of the Declaration of Helsinki (ASSOCIAÇÃO MÉDICA MUNDIAL, 1964), preserving the confidentiality of information sources. The study also met the ethical considerations set out in resolutions number 466 of 2012 and number 510 of 2016, of the National Council for Ethics in Research (CONEP), approved under CAAE[7] 52996816.6.0000.0003 (BRASIL, 2012).
The responsible researchers explained in detail to the volunteer participant, in clear and direct language, the nature of the research, its objectives, methods, expected benefits, ensuring the absence of vices (simulation, fraud or error), dependence, subordination or intimidation. The voluntary participant was free to refuse to participate or withdraw their consent, at any stage of the study, without any penalty and without prejudice to their care. Confidentiality was guaranteed to him, ensuring privacy regarding the confidential data involved in this study (GAIVA, 2009).
To substantiate the consent of the research participants, they were asked to sign a Terms of Free and Informed Consent (TCLE)[8], prepared by the responsible researcher, authorizing their participation. This document, composed of two copies, had one of them retained by the participant and the other archived by the researcher. Both were signed by each party.
The research conferred minimal risks on participants, which were carefully avoided. Risks include suffering or anxiety during the application of the questionnaires, in addition to the possibility of discomfort in answering some questions in the questionnaires.
As a data collection instrument, two questionnaires were used. The first, situational, consists of (1) personal data and (2) professional academic data. The second is the Maslach Burnout Inventory Questionnaire.
The researchers were responsible for carrying out this research within the stipulated period, based on the principles of bioethics at all stages, in order to identify populations with scores corresponding to the Syndrome, and at high risk of developing it.
The research developed as follows:
1st stage: Training of the participating researchers regarding the interpretation of the Maslach Burnout Inventory questionnaire responses.
2nd stage: Establishment of a list of surgeons residing and working in the State of Amapá through information provided by the Regional Council of Medicine of Amapá (CRM-AP).
3rd stage: Active search of selected physicians and application of the two questionnaires.
4th stage: Analysis and interpretation of the data obtained.
In this study, the statistical analysis of the data consisted of processing the information in a convenient way for the subsequent definitive analysis, checking the quality of the data, in order to verify the occurrence of errors, atypical observations, missing data or other peculiarities. After these initial procedures, a descriptive analysis of the data was performed, in order to visualize the frequencies of each variable and the fulfillment of the objectives of the study.
For the construction of graphs and tables, Excel and Word programs were used, components of the Microsoft Corporation Office package.
3. BURNOUT SYNDROME
Coming from the English language, Burnout is understood as “burning after wear and tear” (SOARES et al., 2012). In 1970 the New York psychoanalyst Freudenberger first reported this syndrome, which would become a silent epidemic in modern society (MASLACH et al., 2001; SPIELBERGER and REHEISER, 2005).
Burnout syndrome develops as a chronic response to emotional and interpersonal stressors at work. It occurs more frequently in professionals who are highly involved with people, including medical professionals (PEJUŠKOVIĆ et al., 2011), but little is known about its prevalence (SOARES et al., 2012). Research reveals that the medical profession is clearly among the 100 most stressful professions (IRZYNIEC et al., 2010), with anesthesiology being known as the most exhausting medical specialty (JAKUBAS-KOLAT, 2008). The qualities of work are recognized as an important risk factor for the health of professionals, and directly influence the quality of the service provided to patients by their doctors, and the safety of the patients they assist (RAMA-MACEIRAS and KRANKE, 2013).
It is characterized by: (1) Emotional exhaustion: the professional perceives that he does not have the energy that the work requires; (2) Depersonalization: the professional creates a barrier so that the problems and sufferings of others do not interfere in his life, becoming rigid and cold in the face of the suffering of another person; and (3) reduced professional fulfillment with a constant feeling of dissatisfaction, causing feelings of incompetence and low self-esteem (FRASQUILHO, 2005).
In Brazil, the Social Security Regulation was approved in 1999 through Decree No. 3048, which, in Annex II, deals with Pathogenic Agents that cause Occupational Diseases. In this sense, in Group 5 of the International Classification of Diseases (ICD-10), item XII of the table of Work-Related Mental and Behavior Disorders mentions the “Feeling of Being Finished” (“Burnout Syndrome”, “Professional Burnout Syndrome ”) as synonymous with burnout (TRIGO et al., 2007).
According to the Ministry of Health (2001), among the professionals who most develop Burnout syndrome are those who have direct contact with the users of their care or service. Thus, nurses, doctors, teachers and police, for example, are among the most affected groups (MILLER and MCGOWEN, 2000).
The study carried out by the Federal Council of Medicine, under the coordination of Barbosa et al. (2007), with a sample of 7,700 physicians from all over Brazil. The research shows that most of them (57%) have some worrying degree of Burnout, with 33.9% being described as having moderate manifestation and 23.1% falling into a severe level of the syndrome.
3.1 BURNOUT SYNDROME AND DOCTORS SURGEONS
In the medical field, Burnout Syndrome is more common than depression, suicide and substance abuse and can affect work and the quality of medical care (PEJUŠKOVIĆ et al., 2011). Society expects medical professionals to be infallible, creating professional pressure that is often unsustainable (BARBOSA et al., 2012). The areas with the highest rates of this syndrome are surgery, general practice, psychiatry, pediatric psychiatry, internal medicine, intensive care medicine, oncology (PEJUŠKOVIĆ et al., 2011) and anesthesiology (JAKUBAS-KOLAT, 2008).
Another relevant factor is the lack of control over the schedule during medical school and residency, which contribute to the lifestyle habits that can lead to Burnout Syndrome (BALCH and SHANAFELT, 2010).
Balch and Copeland (2007) have already stated that the transformation that comes from dedication to deleterious work is subtle. Surgeons, because they believe they are more resistant than doctors of other specialties and because they are characterized by commitment, self-sacrifice and focus, become more vulnerable to overwork and the imbalance between personal and professional life (BALCH et al., 2009).
The operating room is the surgeon’s environment for long periods, a complex place with technical challenges, with unpredictable work biases and great expectations about the outcome of the surgeries, which imposes a high load of stress on these professionals, which can be generator of exhaustion and depression (PULCRANO et al., 2016).
Burnout makes the professional less motivated, confident, and efficient in their assignments. The syndrome makes work difficult and reduces the individual’s productive capacity. Thus, it would be best for the professional, together with the hospital, to seek ways to circumvent the situation, through forms of relaxation and leisure, and psychological and/or psychiatric evaluation (SOARES et al., 2011).
It is known that training and surgical practice are already stressors, in addition to other determinants such as lack of autonomy and high volume of patients (MIKALAUSKAS et al., 2012), however, little is known about factors that contribute to the development of Burnout in this population (JESSE et al., 2015).
In 2008, a study carried out by the American College of Surgeons (ACS) with a sample of 8000 physicians found that 40% met the criteria for Burnout, 32% had emotional exhaustion, 26% demonstrated depersonalization and 13% had a poor perception of professional accomplishment. It was found that younger surgeons or those with children between the ages of 5 and 21 are at higher risk, as are the subspecialties of trauma, urology, otolaryngology, vascular and general surgery. This study also reports that the best way to prevent Burnout Syndrome is to actively nurture and protect physical, emotional, psychological and spiritual well-being, from medical school to retirement (DIMOU et al., 2016).
3.2 BURNOUT SYNDROME: DIAGNOSIS
Three questionnaires can be used for the diagnosis of the syndrome, the Staff Burnout Scale for Health Professionals (SBS-HP) by Jones (1980), the Maslach Burnout Inventory (MBI) by Maslach and Jackson (1986) and the Burnout Measure (BM) de Pines and Aronson. The MBI is the most used instrument for measuring the syndrome, as it does not depend on the occupation of the interviewee and the origin of the sample (TAMAYO and TROCCOLI, 2009).
The current version consists of 22 items in Likert format (in the form of statements), each of these items is assigned degrees of intensity ranging from: 0 (never), 1 (a few times a year), 2 (once per month), 3 (a few times a month), 4 (once a week), 5 (a few times a week) and 6 (every day). Completing this questionnaire takes an average of 10 to 15 minutes. It is composed of 3 subscales: “emotional exhaustion”, “depersonalization” and “personal fulfillment”.
“Emotional exhaustion” – consists of 9 questions (1, 2, 3, 6, 8, 13, 14, 16, and 20), which reflect feelings of being emotionally exhausted and exhausted by work. “Depersonalization” – formed by 5 items (5, 10, 11, 15 and 22) that describe impersonal responses. “Personal fulfillment” – consisting of 8 questions (4, 7, 9, 12, 17, 18, 19 and 21), which describe feelings in terms of ability and successes achieved in working with people – this is inversely correlated with the syndrome.
Low scores are those that indicate values below 34 and the reliability of the scale is around 0.9. A low level of burnout reproduces itself in low scores on the “emotional exhaustion” and “depersonalization” subscales; and high scores on “personal fulfillment”. An average burnout level is represented by average values in the scores of the three subscales. Finally, a high level of burnout translates into high scores for the “emotional exhaustion” and “depersonalization” subscales, and low scores for “personal fulfillment”, that is, for the measurement of the three dimensions of the test, we have ratio intervals, which relate to qualitative attributions, have been established.
Thus, “emotional exhaustion” is considered to have a high burnout level when the values are above 27 points. The medium level is identified when the values are between 19-26 points, and the low Burnout level when the points are below 19.
As for “depersonalization”, scores above 10 represent high levels of Burnout, between 6-9 points average levels of Burnout, and less than 6 indicate low levels. So, finally, “personal fulfillment” occurs in the opposite way to the previous ones, with scores greater than or equal to 40 considered as a low level of Burnout, scores between 34-39 considered as an average level of Burnout, and scores lower or higher equal to 33 considered as a high level of Burnout.
4. RESULTS
The research was carried out in the state of Amapá, with questionnaires applied in the cities of Santana and, mainly, Macapá. We interviewed 34 surgeons, subspecialized or not, from March to August 2016.
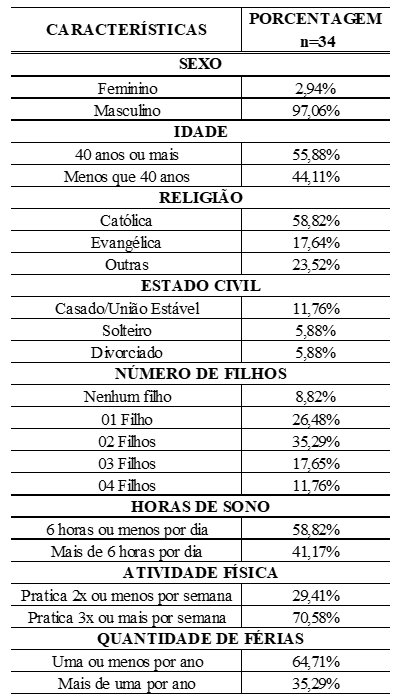
In the population studied, there was a predominance of males (97.05%), the mean age was 42.76 years, most of them married or in a stable relationship (88.23%). Regarding the length of time in the profession, 88.35% had more than 10 years, with an average of 17.97 years of medical practice (Table 1).
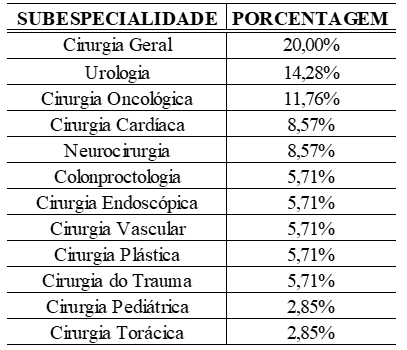
The spectrum of surgical specialties was presented as follows: 20.0% general surgeons, 14.28% urologists, 11.76% oncology surgeons, 8.57% cardiac surgeons, 8.57% neurosurgeons, 5.71% coloproctologists, 5.71% plastic surgeons and 5.71% vascular surgeons, 5.71% endoscopists, 5.71% trauma surgeons, 2.85% pediatric surgeons and 2.85% thoracic surgeons; totaling 12 surgical specialties (Table 1).
Table 1. Distribution of surgeons interviewed by subspecialty, by percentages
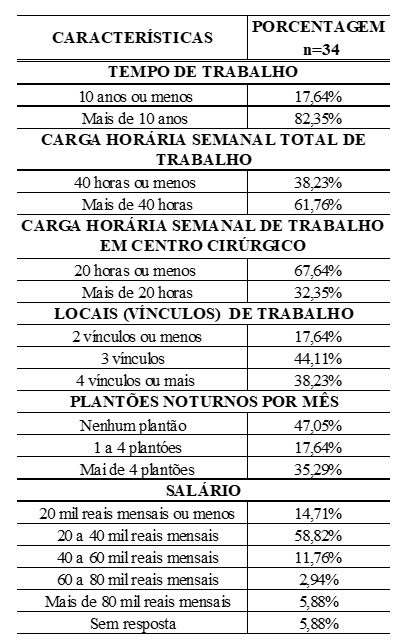
Among those surveyed, 58.82% reported sleeping 6 hours or less per night and 41.17% slept more than 6 hours per night. When asked about the weekly workload, 38.23% answered 40 hours or less and 61.76% more than 40; and 67.64% said they spend 20 hours or less in Surgical Centers per week and 32.35% more than 20 hours. Regarding night shifts, 47.05% do not do it, 17.64% do it between 1 and 4 per month and 35.29% do 5 or more per month (Tables 2 and 3).
Table 2. Personal data
The proportion of 17.64% had up to 2 employment contracts, 44.11% had 3 contracts and 38.23% had 4 or more contracts, including public and private hospitals and clinics (Table 3).
Table 3. Academic-professional data
When examining the questions of the MBI subscales, with regard to Emotional Exhaustion, 32.35% of the surgeons felt sucked into work at least once a week; 38.24% felt consumed at the end of a working day, 17.65% felt frustrated with their jobs at least once a week and 20.59% felt like they were at the end of the line at least a few times a year (Table 4).
Table 4. Percentage of the relative frequency of each item in the MBI, within the corresponding dimension, for the physicians interviewed
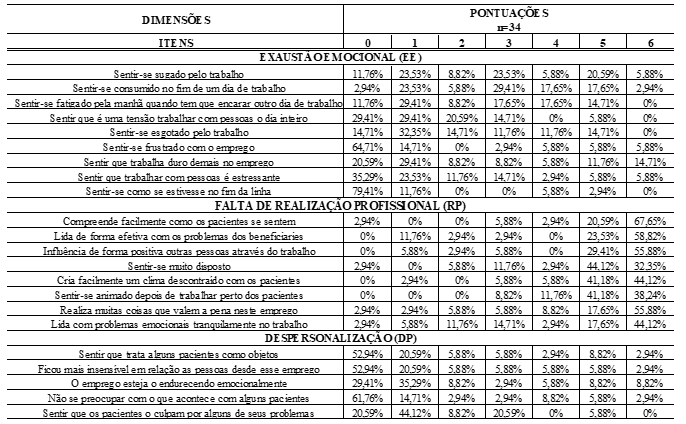
Regarding Depersonalization, the results showed that 47.06% felt that they treated some patients as an object at least a few times a year; 70.59% felt that the job was hardening them; 52.94% never felt they had become more insensitive towards people with this profession; 61.76% are always concerned about what happens to patients; 17.65% felt that they did not care about what happens to some patients at least once a week and 26.47% felt that patients blame them for some of their problems at least a few times a month (Table 4).
Analyzing Personal Fulfillment, 20.59% do not deal with emotional problems calmly at work, up to once a month; 88.24% can easily understand how patients feel at least a few times a week; 85.29% easily create a relaxed atmosphere with patients at least a few times a week; 100% feel excited after working with patients at least a few times a month (Table 4).
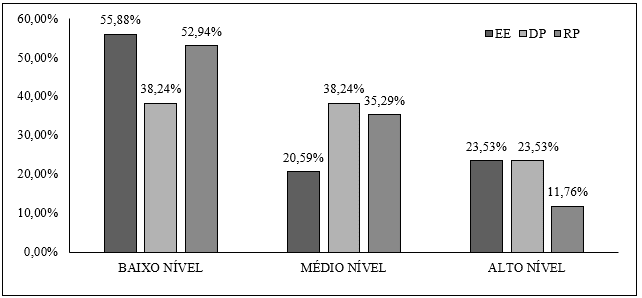
The questionnaire concluded that: (I) Regarding EE: 23.53% had a high level, 20.59% had a medium level, and 55.88% had a low level; (II) DP: 23.53% high level, 38.24% medium level and 38.24% low level; (III) PF: 11.76% have low personal fulfillment, 35.29% have average, and 52.94% have a high PF rate (Graph 1).
Graph 1. Distribution of interviewed surgeons regarding the spheres of the MBI
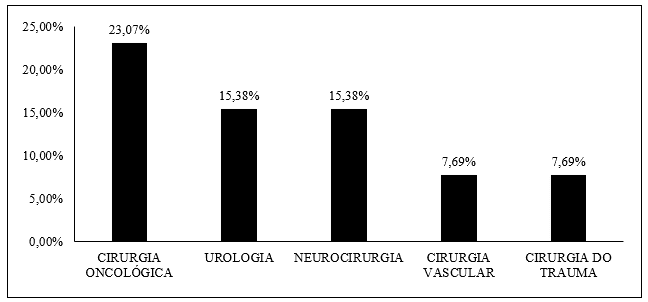
Regarding the 38.23% of respondents who showed changes in at least one of the spheres, 69.23% were subspecialized, and the surgical subspecialties that appeared the most, in descending order, were: oncological surgery (23.07%), neurosurgery (15.38%), urology (15.38%), trauma surgery (7.69%) and vascular surgery (7.69%) (Graph 2).
It is noteworthy that 75% of oncology surgeons and 66.66% of neurosurgeons who responded to the questionnaire had alterations in at least one sphere; of surgeons who had some risk for BS: 100% practice physical activity regularly and 84.62% sleep six hours or less per night.
Graph 2. Distribution of surgeons with a high level of BS in one sphere or more by MBI by subspecialty
Among those who had a high level of EE, it is noted that 100% work in at least three locations, 87.50% work more than 40 hours a week, 62.50% work night shifts, 87.50% have more than ten years of medical training and 75.0% remain in surgical centers for 20 hours or less per week.
Regarding those who had a high level of DP, 75.0% are over 40 years old, 87.50% have graduated for more than 10 years, 75.0% practice physical activity at least three times a week.
Analyzing individuals with low PF, it is noted that 50.0% have been trained for ten years or less, 75.0% spend 20 hours or less in surgical centers, 75.0% do not work night shifts, 75.0% have subspecialty.
5. DISCUSSION
According to Ramirez et al. (1995), only individuals who have a high level of Burnout characteristics can be identified as having the syndrome. Thus, it was found that 2.94% of respondents met the diagnostic criteria for Burnout Syndrome. In two Brazilian scientific works, the numbers presented were similar: Tucunduva et al. (2006) found the syndrome in 3% of cancer physicians in their sample, and Lima et al. (2013) in 5.1% of pediatricians and gynecologists from a hospital in Recife. In contrast, Balch et al. (2010) found 40% of individuals with the syndrome among 7905 American surgeons, as in most other studies (SOARES et al., 2012; LU et al., 2015). This variation, also found in the study by Lima et al. (2013), may be related to the adoption of the MBI, which is considered more rigorous in the diagnosis because it interrelates the three dimensions of the syndrome, or with the small sample, thus limiting the analysis (MIKALAUSKAS et al., 2012).
Emotional exhaustion is considered the initial stage and the central factor of burnout (LIMA et al., 2013) as it is the first reaction to the stress generated by the demand for work. Once exhausted, the individual feels physical and emotional fatigue, with difficulty relaxing and performing their activities (BARBOSA et al., 2012). In this research, 23.53% of surgeons with a high level of EE were identified, similarly to Jesse et al. (2015), who found 23.37% in 218 specialist transplant surgeons.
Regarding depersonalization, considered more frequent in surgeons than in other medical areas according to Pejuskovic et al. (2011) and Sharma et al. (2008), the survey showed that 23.53% of respondents had a high level, similar to that found by Balch et al. (2010) in American surgeons and by Mikalauskas et al. (2012) in cardiac surgeons in Lithuania. Tamayo (1997) justifies the lower numbers than expected, because the depersonalization factor deals with the individual’s insensitivity in the relationship with patients. Questions are rarely answered with sincerity due to the influence of social desirability.
There was a large proportion of physicians who gave importance to the people they cared for. This was evidenced by the 52.94% who stated that they had never been more insensitive towards people with this profession and by the 61.76% who stated that they were always concerned about what happened to patients.
The numbers referring to depersonalization reveal a significant impairment of the doctor-patient relationship, since 70.59% felt that the job was hardening them, and 17.65% did not worry about what happens to some patients, at least once per week.
The lack of reciprocity and emotional distance make the doctor-patient relationship impersonal and indicate that the work requires a great deal of effort on the part of these professionals (LIMA et al., 2013). Of the surgeons, 32.35% feel exhausted by work at least once a week, and 38.24% feel consumed at the end of a working day. Situations referring to emotional exhaustion, but which end up being influenced by depersonalization, demonstrate that both positively correlate their aspects (TAMAYO et al., 2002).
The low professional achievement represented by 11.76% of respondents also appears in the work of Balch and Shanafelt (2010), in which 13% have a low level. This is a similar study, which interviewed surgeons from different areas and also analyzed the demographic profile. Mikalauskas et al. (2012) found 42.3% of cardiac surgeons with low professional achievement in their work. A possible justification for such a difference revolves around subspecialization, as the more subspecialized the professional, the greater the risk of developing the syndrome (BALCH and SHANAFELT, 2010). The small percentage found in the present study can also be explained by Barbosa et al. (2012) when he states that this dimension of the syndrome is considered the last reaction to appear, in this way the surgeons of the research in question could be considered at the beginning of the Burnout process.
Visser et al. (2003) and Lima et al. (2013) found that the negative consequences of occupational stress have the protective effect of high professional satisfaction, being also influenced by the working condition, supporting the findings of this research, in which 52.94% of respondents had high levels of professional fulfillment.
Although only 2.94% had completed criteria for the diagnosis of Burnout Syndrome, 14.71% of surgeons were at high risk for the syndrome in two of the three spheres of analysis, and 20.59% in one of the three spheres. If the multidimensionality of Burnout is disregarded, as Grunfeld et al. (2002), that is, if we attribute the presence of the syndrome by finding at least one of the three: high level of EE or DP, and low level of PF, we will have a burnout level of 20.59% of surgeons in the state of Amapá.
Even when we do not consider the multidimensionality of the syndrome, the results found are lower than expected. The surgeons interviewed, despite the stress of the specialty extolled by several authors (SHARMA et al., 2008), are considerably satisfied with their work.
Macapá is the city where 94.12% of respondents work. In the bibliographic review to support this research, data from the IBGE [9] were consulted, which point to this Brazilian capital as the fourth least populous (465,495 inhabitants) and with the lowest cost of living. It has a lower number of doctors per thousand inhabitants (0.44) and its longevity index is 0.715, higher than the Brazilian average of 0.638. Despite being the fifth capital with the largest total area (6,407,123 mk²), it has the third smallest urban area (32.7 mk²), where all four public hospitals in the state are concentrated, and the private hospital associated with SUS[10] (IBGE, 2016).
These data allow us to infer that the city where they work allows surgeons to spend less time commuting from one job to another, or between work and home, as well as having to work less than in other capitals to maintain their standard of living.
The predominance of males in the research sample (97.05%) agrees with the majority of authors who researched on the topic (FLETCHER et al., 2012; BALCH and COPELAND, 2007; GROSS et al., 2000). The survey data are statistically irrelevant to analyze the prevalence of the syndrome according to sex, since the number of female surgeons participating in the survey was small.
The mean and median ages were, respectively, 42.76 years and 39 years (30-63), and 88.35% had more than ten years of medical profession (mean 17.97 years). These data partly explain the low burnout rate in the sample. According to Sharma et al. (2008), the level of Burnout is indirectly proportional to age and time of medical practice, and young surgeons are more likely to develop, mainly, Depersonalization.
Respondents were mostly married or in a stable relationship (88.23%). A significant finding is that 25.0% of depersonalized respondents are divorced, which corresponds to 100% of the divorcees who participated in the survey, which reaffirms the high risk of divorce among surgeons (up to 1.7 higher) shown by Rollman et al. (1997).
The weekly workload is a statistically significant indicator and is directly related to the risk of the syndrome, as well as other psychological illnesses and low job satisfaction, in several studies. This study agrees with this data. Among those surveyed, 61.76% work more than forty hours a week, and of those who have Burnout in one or more spheres, 69.23% do so. In contrast, Morse et al. (1984) did not find a significantly relevant relationship between weekly working hours and professional burnout.
With regard to daily hours of sleep, 58.82% sleep six hours or less. Among the surgeons who had burnout in at least one sphere, 84.61% sleep six hours or less, in agreement with what Mikalauskas et al. (2012), in 2012, in their study on Burnout in cardiac surgeons and anesthesiologists in Lithuania.
In the present study, 61.54% of surgeons who have a high level of Burnout in at least one subscale perform night shifts. However, the number of monthly night shifts of the surgeons in the research is relatively small (47.05% do not do them, and 17.64% do between one and four), which, according to Liselotte et al. (2009), configures a protection factor for Burnout, justifying our presented results.
Regarding the 38.23% of respondents who showed changes in at least one of the spheres, 69.23% were subspecialized (and 30.74% General Surgeons), and the surgical subspecialties that were most affected, in descending order, were cancer surgery (23.07%), neurosurgery (15.38%) and urology (15.38%). Balch et al. (2011) found Burnout in 31.6%, and suicidal ideation in 4.9% of the Oncology Surgeons in their research. In our study, 50.0% of them showed a high level of Emotional Exhaustion. Still in Balch et al. (2011), neurosurgeons achieved burnout in 38.5%, and Urologists had the third highest rate of the syndrome (49.9%).
The only subspecialty that had respondents with a confirmed diagnosis in the three subscales of the MBI was Vascular Surgery, classified by Balch and Shanafelt (2010) as the second (Trauma Surgery was in first place) with a greater propensity for Burnout and lower levels of job satisfaction.
Of the general surgeons interviewed, 57.14% had a high level of Depersonalization and 85.71% of them work at least one night shift per week, which corresponds to the group of surgeons that most do them in the present research. Balch and Shanafelt (2010) associate General Surgeons’ dissatisfaction with lack of autonomy and a feeling of non-professional growth, and claim greater propensity for personal conflicts and the desire to retire early.
6. CONCLUSION
The purpose of this work was to provide knowledge about the Burnout Syndrome to the surgeons participating in the research, and to analyze its prevalence in the sample, considering the surgical specialty, the socioeconomic profile and the working conditions to which they are submitted.
The guiding question of the study was whether surgeons in the state of Amapá have a high prevalence of the Syndrome. In addition to being evidenced by the world literature, due to the responsibility imposed by the profession and the stress that usually permeates the Surgical Centers, there are structural factors in the state of Amapá, the Brazilian capital with the lowest number of doctors per thousand inhabitants.
The research was carried out in the state of Amapá from March to August 2016, and physicians working in the municipalities of Macapá and Santana were interviewed. Most of them reside in Macapá.
The count of registered surgeons in the state of Amapá was provided by the Regional Council of Medicine of the state and showed a number of fifty-six. Forty surgeons, duly registered in the CRM-AP, were approached, and thirty-four of them agreed to participate in the research.
In view of the explanation about the research and acceptance of the terms and completion of the TCLE, two questionnaires were answered: one personal and academic-professional, and another validated by the MBI. This one with twenty-six fields answered according to a Likert scale, which, when their answers were coded, translated the levels of Depersonalization, Emotional Exhaustion and Personal Fulfillment into high, low or moderate. The syndrome is diagnosed when the worst levels are reached in the three spheres, and it is said to be “high risk” for Burnout when two of the three mentioned spheres are present at the worst levels.
After the active search phase and application of the questionnaires was completed, the tabulation and analysis of the results obtained began.
General surgeons and the following subspecialties were present: urology, oncological surgery, cardiac surgery, neurosurgery, coloproctology, plastic, vascular, endoscopic, trauma, pediatric and thoracic surgery. Only a third of the interviewees worked in 4 or more services (links), and just over sixty percent had a weekly workload of more than 40 hours. Almost half of the sample did not make night shifts, and a third made up to four night shifts per month.
A good portion (38.23%) of those surveyed showed changes in at least one of the three spheres. Of these, 69.23% were subspecialized, and the subspecialties that obtained the worst results were: Vascular Surgery, Oncological Surgery, Neurosurgery and Urology. Hypotheses that explain the numbers found permeate the fact that these specialties concentrate highly complex surgeries, which demand a better hospital structure, often require intensive care beds in the postoperative period, and instruments are not always available in public hospitals in Macapá, such as, for example, surgical staplers.
Regarding the MBI questionnaire, we had about a quarter of those surveyed with a high level of EE, the same number with a high level of DP, and just over ten percent with a low PF. Our sample showed good levels of PF: 52.94% with a high level.
Working in more than three jobs, working more than 40 hours per week, working night shifts, and staying in Surgical Centers for 20 hours or less were risk factors for EE. Being over 40 years old was a risk factor for DP. Ten years or more of medical practice was a risk factor for both. Sleeping six hours or less was a risk factor for changes in all three subscales.
Since only 2.94% completed criteria for the diagnosis of Burnout Syndrome, the guiding question was refuted. The low prevalence can be explained by the adoption of the MBI criteria, considered more rigorous because they interrelate the three dimensions of the syndrome, the small sample, or even facts related to the city where most of the interviewees live (such as low cost of living, and small urban area). This allows us to infer that surgeons spend little time traveling between jobs and between home and work.
Of the difficulties encountered during the research, two stand out: i) Some of the surgeons registered in the CRM-AP do not reside in the state, which made it difficult for researchers to approach and, consequently, reduced the study sample; ii) Some surgeons, when invited to participate, reported that they would no longer operate, and were removed from the research to avoid bias, which also reduced the sample; iii) The amount of research carried out exclusively by medical surgeons internationally is small, and almost scarce at the national level, which reduced the spectrum of comparisons of results.
In this context, we highlight the importance of adopting preventive measures against Burnout, to be developed both by surgeons and by the hospitals and clinics in which they work, to improve the quality of life and work quality of these individuals, as well as the search for guarantee of a humanized doctor-patient relationship.
Finally, Burnout Syndrome was investigated among surgeons in the State of Amapá and a quantitative of 2.94% was found. It is concluded that although this group has a higher rate of this disease than the general population, it has lower levels than those found in other scientific works published worldwide, with the target of research in surgeons.
REFERENCES
ASSOCIAÇÃO MÉDICA MUNDIAL. Declaração de Helsinki. Aprovada na 18ª Assembleia Médica Mundial, Helsinki, Finlândia, 1964 Disponível em: <http://www.ufrgs.br/bioetica/helsin1.htm.>. Acesso em: 03/05/2016
BALCH, C.M.; COPELAND E. Stress and burnout among surgical oncologists: a call for personal wellness and a supportive workplace environment. Ann. Surg. Oncol., v. 14, n. 11, p. 3029-3032, 2007. Disponível em: DOI 10.1245/s10434-007-9588-0. Acesso em: 12/07/2022.
BALCH, C.; SHANAFELT, T. Combating Stress and Burnout in Surgical Practice: A Review. Advances in Surgery, v. 44, p. 29–47, 2010. Disponível em: DOI 10.1016/j.yasu.2010.05.018. Acesso em: 12/07/2022.
BALCH, C.M.; SHANAFELT, T.D.; SLOAN, J.A.; SATELE, D.V.; FREISCHLAG, J.A. Distress and career satisfaction among 14 surgical specialties, comparing academic and private practice settings. Ann. Surg., v. 254, n. 4, p. 558-568, 2011. Disponível em: DOI 10.1097/SLA.0b013e318230097e. Acesso em: 12/07/2022.
BARBOSA, F.T.; LEÃO, B.A.; TAVARES, G.N.S.; SANTOS, J.G.R.P. Burnout syndrome and weekly workload of on-call physicians: cross-sectional study. São Paulo Med J., v. 130, n. 5, p. 282-288, 2012. Disponível em: DOI 10.1590/S1516-31802012000500003. Acesso em: 12/07/2022.
BARBOSA, G.A.; ANDRADE, E. O.; CARNEIRO, M. B.; GOUVEIA, V. V. A saúde dos médicos no Brasil. Brasília: Conselho Federal de Medicina, 2007.
BRASIL. Conselho Nacional de Saúde. Resolução n° 466, 2012. Diretrizes e Normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília, 13 jun. 2013. Seção 1 p. 59.
BRASIL, ANVISA. Portaria n. 400 de 6 de dezembro de 1977. Dispõe sobre norma e padrões de instalação e construção em serviços de saúde. Distrito Federal, Brasília: Diário Oficial da União, 06 de dezembro de 1977. Disponível em:<http://e-legis.bvs.br/leisref/public/showAct.php?id=1121>. Acesso em: 03/05/2016
CONSELHO FEDERAL DE MEDICINA. Demografia Médica no Brasil. São Paulo:
Conselho Regional de Medicina do Estado de São Paulo: Conselho Federal de Medicina, 2013.
CHERNISS, C. Professional Burnout in human service organizations. New York: Praeger, 1980.
COCHRAN, W.G. Sampling techniques. 3rd.ed. New York: John Wiley, 1977. 428p.
DIMOU, F. M.; ECKELBARGER, D.; RIALL, T. S. Surgeon Burnout: A Systematic Review. J Am Coll Surg, v. 222, n. 6, p. 1230–1239, 2016. Disponível em: DOI 10.1016/j.jamcollsurg.2016.03.022. Acesso em: 12/07/2022.
FLETCHER, A.M.; PAGEDAR, N.; SMITH, R.J.H. Factors correlating with Burnout in practicing otolaryngologists. Otolaryngol Head Neck Surg., v. 146, n. 2, p. 234-239, 2012. Disponível em: DOI 10.1177/0194599811428585. Acesso em: 12/07/2022.
FRASQUILHO, M.A. Medicina, uma jornada de 24 horas? Stress e Burnout em médicos: prevenção e tratamento. Saúde Mental, v. 23, n. 2, 2005.
GAIVA, M.A.M. Pesquisa envolvendo crianças: aspectos éticos. Revista Bioética, v. 17, n. 1, p. 135-146, 2009.
GROSS, C.P.; MEAD, L.A.; FORD, D.E.; KLAG, M.J. Physician, heal thyself? Regular source of care and use of preventive health services among physicians. Arch. Intern. Med., v. 160, n. 21, p. 3209-3214, 2000. Disponível em: DOI 10.1001/archinte.160.21.3209. Acesso em: 12/07/2022.
GRUNFELD, E.; WHELAN, T.J.; ZITZELSBERGER, L.; WILLAN, A.R.;
MONTESANTO, B.; EVANS, W.K. Cancer care workers in Ontario: prevalence of Burnout, job stress and job satisfaction. JAMC, v. 163, n.2, p. 166-169, 2002.
HSE. Health and safety regulation – A short guide. London UK, 2003. Disponível em: < https://www.hse.gov.uk/pubns/hsc13.pdf >. Acesso em: 04 julho 2022.
IBGE. INSTITUTO BRASILEIRO DE GEOGRAFIA E ESTATÍSTICA. 2016. Disponível em: <http://www.ibge.gov.br/home/>. Acesso em: 03/05/2016
IRZYNIEC, T.; KONODYBA-SZYMAŃSKI, P.; SZCZERBA, H. Identyfikacja zagrożeń oraz ocena ryzyka zawodowego lekarzy medycyny (wstępne wyniki). J. Ecol. Health, v. 14, p. 295–302, 2010. Recuperado de https://bibliotekanauki.pl/articles/271618. Acesso em: 12/07/2022
JAKUBAS-KOLAT, J. Zjawisko stresu w pracy zespołu anestezjologicznego. Anest. Rat., v. 1, p. 66–69, 2008. Recuperado de https://www.akademiamedycyny.pl/wp-content/uploads/2016/05/201301_AiR_002.pdf. Acesso em: 12/07/2022
JARRUCHE, L. T., MUCCI, S. Síndrome de Burnout em profissionais da saúde: revisão integrativa. Revista Bioética, v. 29, n. 1 pp. 162-173, 2021. Disponível em: DOI 10.1690/1983-80422021291456. Acesso em: 12/07/2022.
JESSE, M.T.; ABOULJOUD, M.; ESHELMAN, A. Determinants of Burnout Among Transplant Surgeons: A National Survey in the United States. American Journal of Transplantation, v. 15, p. 772-778, 2015. Disponível em: DOI 10.1111/ajt.13056. Acesso em: 12/07/2022.
LIMA, R. A. S. et al. Vulnerabilidade ao burnout entre médicos de hospital público do Recife. Ciência e Saúde Coletiva, v. 18, n. 4, p. 1051-1058, 2013. Disponível em: DOI 10.1590/S1413-81232013000400018. Acesso em: 12/07/2022.
LISELOTTE, E.; BERGQUIST, A.K.; ARNBERG, K. Business collaboration as a prerequisite for learning and innovation: A study of structural fund projects. Lund: Studentlitteratur, v. 1, p. 217-230. 2009.
MASLACH, C.; SCHAUFELI, W.B.; LEITER, M.P. Job Burnout. Annual Review Psychology, n. 52, p. 397-422, 2001.
MIKALAUSKAS, A.; SIRVINSKAS, E.; MARCHERTIENE, I.; MACAS, A.; SAMALAVICIUS, R.; KINDURIS, S.; BENETIS, R. Burnout Among Lithuanian Cardiac Surgeons and Cardiac Anesthesiologists. Medicina (Kaunas), v. 48, n. 9, p. 478-484, 2012. Disponível em: DOI 10.3390/medicina48090071. Acesso em: 12/07/2022.
MILLER, N.; MCGOWEN, R. The painful truth: physicians are not invincible. South Medical Journal. v. 93, n. 10, p. 966-973, 2000. Disponível em: DOI 10.1097/00007611-200093100-00004. Acesso em: 12/07/2022.
MS. Ministério da Saúde do Brasil. Portaria nº400. Brasília DF: Ministério da Saúde 1977.
MS. Ministério da Saúde do Brasil. Doenças relacionadas ao trabalho: manual de procedimentos para os serviços de saúde. Brasília: Ministério da Saúde do Brasil, 2001.
MORSE, R.M.; MARTIN, M.A.; SWENSON, W.M.; NIVEN, R.G. Prognosis of physicians treated for alcoholism and drug dependence. JAMA, v. 251, n. 6, p. 743746, 1984. Disponível em: DOI 10.1001/jama.1984.03340300035024. Acesso em: 12/07/2022.
MOURA, A. A. P. ; PINHEIRO, F. F. ; PINGARILHO, J. G. ; DIAS, C.A.G.M. ; OLIVEIRA, E. ; DENDASCK, C. V. ; ARAUJO, M. H. M. ; FECURY, A. A. Burnout syndrome in professionals from a basic health unit of Macapá,-Amapá, Brazil. Revista Científica Multidisciplinar Núcleo do Conhecimento, v. 04, p. 05-21, 2018. https://www.nucleodoconhecimento.com.br/biologia/sindrome . DOI: 10.32749/nucleodoconhecimento.com.br/biologia/sindrome. Acesso em: 10/07/2022
NOGUEIRA-MARTINS, L.A. Residência Médica: estresse e crescimento. São Paulo: Casa do Psicólogo, 2005.
PEJUŠKOVIĆ, B.; LEČIĆ-TOŠEVSKI, D.; PRIEBE, S.; TOŠKOVIĆ, O. Burnout syndrome among physicians – the role of Personality dimensions and coping strategies. Psychiatria Danubina, v. 23, v. 4, p. 389-395, 2011. Recuperado de: https://www.researchgate.net/publication/51791575. Acesso em: 10/07/2022
PULCRANO, M.; STEPHEN, R.T; EVANS, M.D; SOSIN, M.M.D. Quality of life and Burnout rates across surgical specialties, a systematic review. JAMA Surgery, v. 151, n. 10, p. 970-978, 2016. Disponível em: DOI 10.1001/jamasurg.2016.1647. Acesso em: 12/07/2022.
RAMA-MACEIRAS, P.; KRANKE, P. Working conditions and professional wellbeing: a link easy to imagine but difficult to prove. Eur. J. Anaesthesiol., v. 30, p 213–215, 2013. Disponível em: DOI 10.1097/EJA.0b013e32835fc894. Acesso em: 12/07/2022.
RAMIREZ, A.J.; GRAHAM, J.; RICHARDS, M.A.; CULL, A.; GREGORY, W.M. Burnout and psychiatric disorder among cancer clinicians. British Journal of Cancer, v. 71, p. 1263- 1269, 1995. Disponível em: DOI 10.1038/bjc.1995.244. Acesso em: 12/07/2022.
ROLLMAN, B.L.; MEAD, L.A.; WANG, N.Y.; KLAG, M.J. Medical specialty and the incidence of divorce. New England J. Med., v. 336, n. 11, p. 800-803, 1997. Disponível em: DOI 10.1056/NEJM199703133361112. Acesso em: 12/07/2022.
SCOTT, C.; HAWK, J. Heal thyself: the health of healthcare professionals. New York: Brunner-Mazel, 1986. Disponível em: DOI 10.1001/jama.1986.03380110108042. Acesso em: 12/07/2022.
SHARMA, A.; SHARP, D.M.; WALKER, L.G.; MONSON, J.R. Stress and Burnout in colorectal and vascular surgical consultants working in the UK National Health Service. Psycho-Oncology, v. 17, p. 570-576, 2008. Disponível em: DOI 10.1002/pon.1269. Acesso em: 12/07/2022.
SOARES, L.R.; LOPES, T.M.O.; SILVA, M.A.O.; RIBEIRO, M.V.A.; JÚNIOR, M.P.A.; SILVA, R.A.; ALVES, R.F.; BUENO, T.G.G.; SALGADO, T.A.; CHEN, L.C. Burnout e pensamentos suicidas em médicos residentes de Hospital Universitário. Revista Brasileira De Educação Médica, v. 36, n. 1, p. 77-82, 2012. Disponível em: https://doi.org/10.1590/S0100-55022012000100011. Acesso em 12/07/2022.
SPIELBERGER, C.D.; REHEISER, E.C.; ANTONIOU, A.G.; COOPER, C.L. (eds). Occupational stress and health. In: Research companion to organizational health psychology. Northampton: Edward Elgar, p. 441-454, 2005. Disponível em: https://doi.org/10.1590/0034-7167-2018-068. Acesso em 12/07/2022.
TAMAYO, M. R. Relação entre a síndrome do Burnout e os valores organizacionais no pessoal de enfermagem de dois hospitais públicos. Dissertação de mestrado não-publicada, Brasília: Universidade de Brasília, 1997.
TAMAYO, M.; TRÓCCOLI, B.T. Burnout no trabalho. In: Mendes, A.M.; Borges, L.O.; Ferreias; M.C., porganizadores. Trabalho em transição, saúde em risco. Brasília: Editora Universidade Brasília, p.45-63, 2002.
TAMAYO, M.; TRÓCCOLI, B.T. Construção e validação fatorial da Escala de Caracterização do Burnout (ECB). Estudos em Psicologia, v. 14, n. 3, p. 213-221, 2009. Disponível em: https://doi.org/10.1590/S1413-294X2009000300005. Acesso em 12/07/2022.
TRIGO, T.R.; TENG, C.T.; HALLAK, J.E.C. Síndrome de Burnout ou estafa profissional e os transtornos psiquiátricos. Revista Psiquiatria Clínica, v. 34, n. 5, p. 223-233, 2007.
TUCUNDUVA, L.T.C.M.; GARCIA, A.P.; PRUDENTE, F.V.B.; CENTOFANTI, G.;
SOUZA, C.M.; MONTEIRO, T.A.; VINCE, F.A.H.; SAMANO, E.S.; GONÇALVES, M.S.; GIGLIO, A.D. A síndrome da estafa profissional em médicos cancerologistas brasileiros. Revista Associação Medicina Brasileira, v. 52, n. 2, p. 108-112, 2006. Disponível em: DOI 10.1590/S0104-42302006000200021. Acesso em 12/07/2022.
VISSER, M.R.M.; SMETS, E.M.A.; OORT, F.J.; HAES, H.C.J.M. Stress, satisfaction and burnout among Dutch medical specialists. DMAJ, v. 168, n. 3, p. 271-275, 2003. Disponível em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC140468/. Acesso em 12/07/2022.
WHO. WORLD HEALTH ORGANIZATION; Guidelines for the primary prevention of mental, neurological and psychosocial disorders: Staff Burnout. In: Geneva Division of Mental Health World Health Organization, p. 91-110, 1998.
APPENDIX – FOOTNOTE
7. Certificate of Presentation of Ethical Appreciation.
8. The Terms of Free and Informed Consent – Termos de Consentimento Livre e Esclarecido (TCLE) are intended to provide research subjects with the broadest possible clarification about the investigation to be carried out, its risks and benefits, so that their willingness to participate (or not) ), is effectively free and conscious.
9. Brazilian Institute of Geography and Statistics.
10. Health Unic System.
[1] Specialization in General Surgery, graduated in Medicine. ORCID: 0000-0001-7321-9167.
[2] Specialization in General Surgery, graduated in Medicine. ORCID: 0000-0002-6160-8410.
[3] Specialization in Gynecology and Obstetrics, graduated in Medicine.
[4] Specialization in General Practice, graduated in Medicine. ORCID: 0000-0003-3823-6812.
[5] Academic of Medicine. ORCID: 0000-0002-6043-018X.
[6] PhD from the Interdisciplinary Surgical Science program at UNIFESP/EPM (2016-20), Master of Science at the Surgical Gastroenterology Program at Escola Paulista de Medicina/Federal University of São Paulo, General Surgeon, Specialist in Surgical Oncology (SCB/AMB) and Surgery of the Digestive System. ORCID: 0000-0003-4972-3448.
Sent: May, 2022.
Approved: July, 2022.















