ORIGINAL ARTICLE
MONTEIRO, Lis Mayra Dantas [1], FACCO, Lucas [2], FECURY, Amanda Alves [3], ARAÚJO, Maria Helena Mendonça de [4], OLIVEIRA, Euzébio de [5], DENDASCK, Carla Viana [6], SOUZA, Keulle Oliveira da [7], DIAS, Claudio Alberto Gellis de Mattos [8]
MONTEIRO, Lis Mayra Dantas. Et al. Number of cases of leprosy in Brazil from 2010 to 2015. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 05, Ed. 11, Vol. 25, pp. 62-70. November 2020. ISSN:2448-0959, Access link in: https://www.nucleodoconhecimento.com.br/health/leprosy-in-brazil, DOI: 10.32749/nucleodoconhecimento.com.br/health/leprosy-in-brazil
ABSTRACT
Leprosy is considered an infectious disease, caused by the bacterium Mycobacterium leprae also known as Hansen’s Bacillus. In addition to being a disease with gradual evolution, leprosy depends on the relationship between the parasite and the host. The aim of this study was to show the number of leprosy cases in Brazil between 2010 and 2015 in Brazil. The research was carried out at DATASUS (http://datasus.saude.gov.br/). With the advancement of public policies, the number of cases of the disease in Brazil decreased between 2010 and 2015. It has a higher prevalence in males and the highest rate of patients is found in older age groups, that is, in adults. The disease incubation period (which can vary from 2 to 7 years). In view of this, several problems can be triggered at the individual level, such as debilitating and psychological physical disorders. With a view to reducing the number of cases of the disease in the country and making the diagnosis as early as possible, the clinical findings and tests available for this detection should be analyzed.
Keywords: Epidemiology, Hansen’s disease, Mycobacterium leprae.
INTRODUCTION
Leprosy is considered an infectious disease, as it needs direct contact with the bacillus to be transmitted between people. It is caused by the bacterium Mycobacterium leprae also known as Hansen’s bacillus. This disease is only detected, on average, between 2 to 7 years of incubation and the symptoms usually appear from 11 to 16 days. In this symptomatic phase, interpersonal transmission is possible, and normally, only a small portion gets sick (BRASIL, 2002; OLIVEIRA et al., 2016).
Leprosy can be classified into two forms: Paucibacillary leprosy or Multibacillary leprosy. In the Paucibacillary variation, the patient has resistance to bacilli, with up to five skin lesions. Bacilli are found in smaller numbers in the body, not being enough for transmission to other people. In this case, there is the possibility of spontaneous cure. Multibacillary leprosy makes up the so-called transmitter group, with six or more skin lesions. The sick have no defense against the bacteria, eliminating them through the airways (BRASIL, 2002; BRASIL, 2016). Contagion usually occurs through direct contact between a susceptible person and an untreated patient, usually a family member (BRASIL, 2015).
In addition to being a disease with gradual evolution, leprosy depends on the relationship between the parasite and the host. When the host has an efficient defense system, it tends not to manifest the disease. For various reasons, such as socioeconomic vulnerability and living with many people in the same environment, it can affect individuals of various ages and both sexes (BRASIL, 2002).
Symptoms may appear on the skin or in the nervous system. In the skin they are usually characterized by lesions with loss or increased sensitivity. Pigment spots, plaques, infiltrations, tubers and / or nodules may appear. In the nervous system, symptoms may appear as physical disabilities and, depending on the degree of the disease, deformities in the extremities of the body (BRASIL, 2002; FREITAS, 2015).
The treatment of leprosy is done with the combination of several drugs, called polychemotherapy or PQT. For patients with the Paucibacillary form, two types of antibiotics are used. For those with Multibacillary form, three types of antibiotics are recommended (BRASIL, 2002; FREITAS, 2015).
According to the Ministry of Health, the number of new cases registered in Brazil during the years surveyed was 193,021 patients. (BRASIL, 2017).
GOAL
Show the number of leprosy cases in Brazil from 2010 to 2015 in Brazil.
METHOD
The research was conducted at DATASUS (http://datasus.saude.gov.br/), with leprosy data being taken from the following steps: in the “Access to Information” tab, “Health Information (TABNET)” “and right after,” Epidemiological and Morbidity “was clicked. On the next page when clicking on “Hansen’s disease cases – Since 2001 (SINAN)”, the option “Hansen’s disease – since 2001” was chosen, and in geographic scope, “Brazil by Region and Federation Unit” was chosen. Data were collected from 2010 to 2015, choosing: online the options “Diagnostic year”, “Region”, “Sex”, “Age group”, “Detection mode”, “Diagnostic evaluation” and “Skin lesion”. In the column field the option “Not active” and in content the phrase “Patients per Service” were used for the line options above. After the selection, these data were compiled in the Excel tool, Office component of Microsoft Corporation. Bibliographical research carried out in the laboratory of the Federal Institute of Education, Science and Technology of Amapá, Campus Macapá, located at: Rodovia BR 210 KM 3, s / n – Bairro Brasil Novo. CEP: 68.909-398, Macapá, Amapá, Brazil.
RESULTS
Figure 1 shows the number of leprosy cases in Brazil between 2010 and 2015. It is observed that in the last few years there has been a decrease in the number of cases, with a small increase in the number of 2014 compared to the year 2013.
Figure 1 Number of leprosy cases in Brazil between 2010 and 2015.
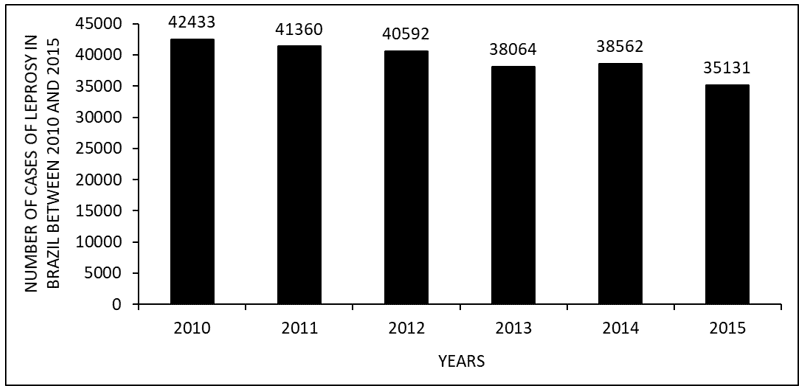
Figure 2 shows the number of leprosy cases in Brazil between 2010 and 2015, by regions of the country. The data show that the largest number of visits occurs in the Northeast and the minority in the South.
Figure 2 Shows the number of leprosy cases in Brazil between 2010 and 2015, by regions of the country.
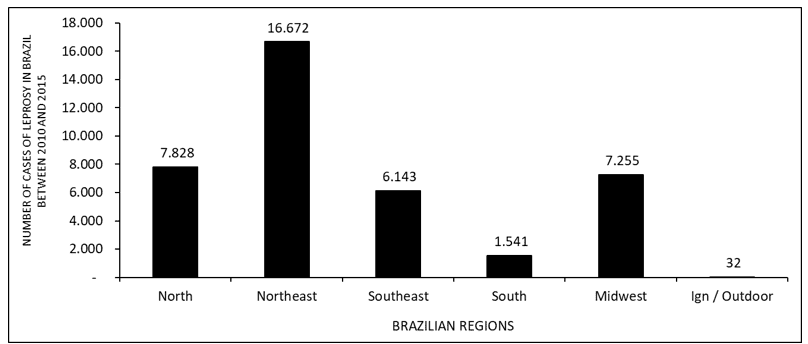
Figure 3 shows the number of leprosy cases in Brazil between 2010 and 2015, according to gender. Where it is observed that there is a greater number of occurrences in males when compared to females.
Figure 3 Shows the number of leprosy cases in Brazil between 2010 and 2015, according to gender.
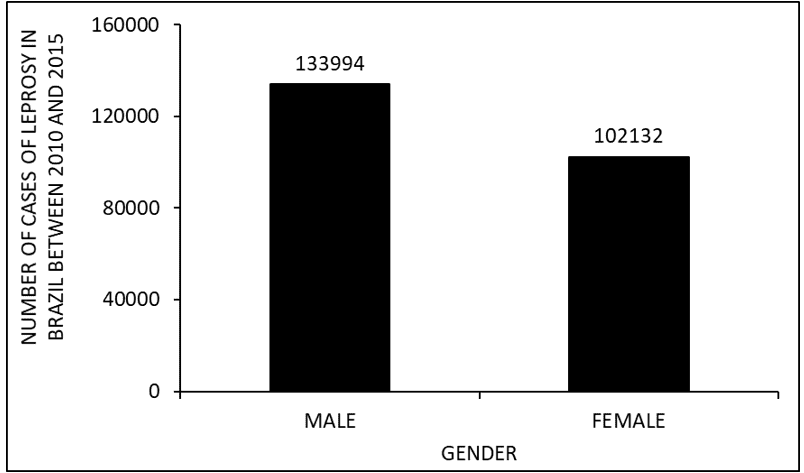
Figure 4 shows the number of leprosy cases in Brazil between 2010 and 2015, by age group. Where there is a higher rate of occurrence of the disease in adults aged 20 to 64 years, and lower in children aged 1 to 9 years and elderly people aged 80 and over.
Figure 4 Shows the number of leprosy cases in Brazil between 2010 and 2015, by age group.
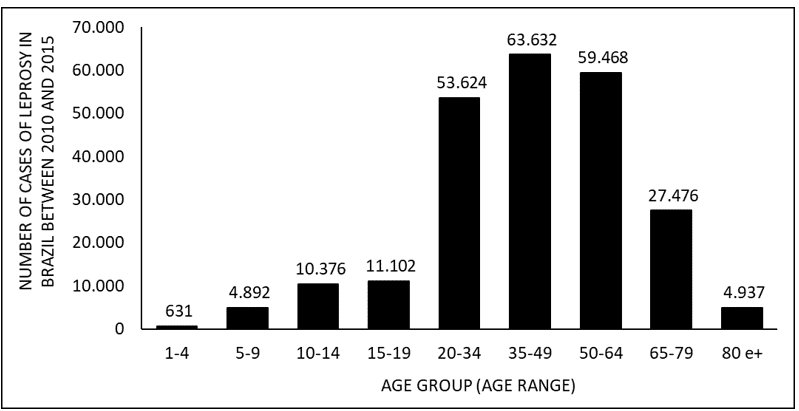
Figure 5 shows the number of leprosy cases in Brazil between 2010 and 2015, according to the detection mode. The main way of detecting the disease is referrals, followed by spontaneous demand.
Figure 5 Shows the number of leprosy cases in Brazil between 2010 and 2015, according to the detection mode.
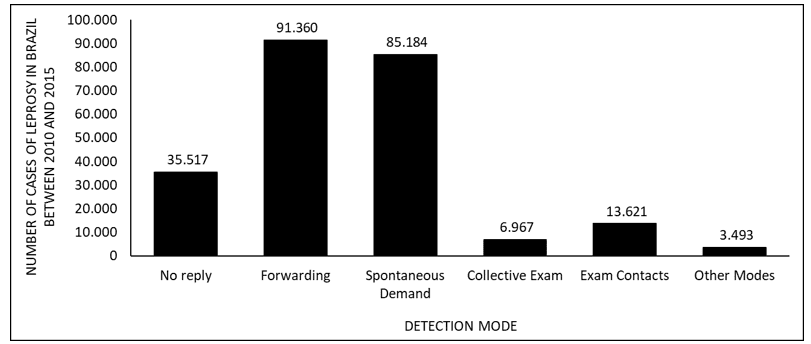
Figure 6 shows the number of leprosy cases in Brazil between 2010 and 2015, by types of skin lesion. The data show the majority of patients have 2 to 5 skin lesions and the minority does not have any lesions.
Figure 6 Shows the number of leprosy cases in Brazil between 2010 and 2015, by type of skin lesion.
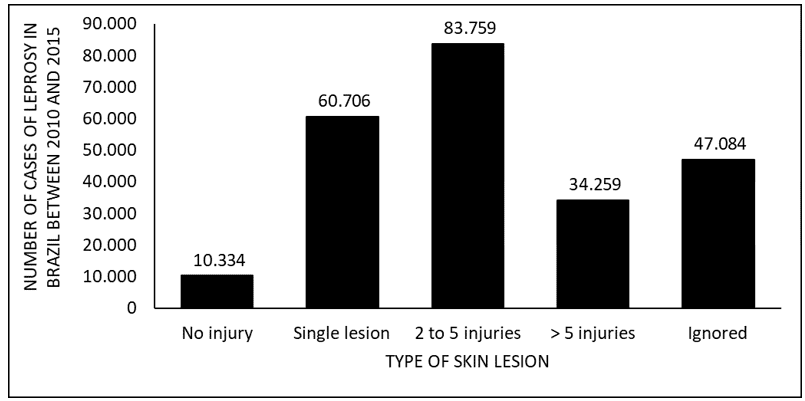
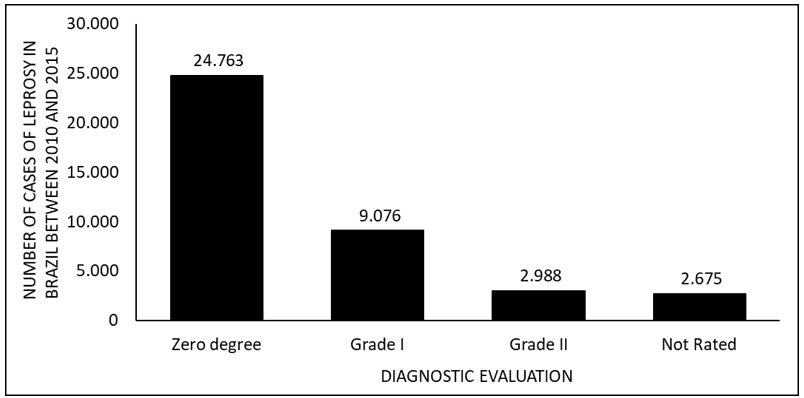
Figure 7 shows the number of leprosy cases in Brazil between 2010 and 2015, by diagnostic evaluation. The data show that the majority of cases are from grade zero and the minority from grade II of the disease.
Figure 7 Shows the number of leprosy cases in Brazil between 2010 and 2015, by diagnostic evaluation.
DISCUSSION
During the years 2010 to 2015, it was observed that there was a decrease in the number of patients treated with leprosy, with a small increase in 2014 (figure 1). The data are corroborated by the literature. The decrease was probably due to the implementation of public policies to face the disease, such as early diagnosis and successful treatment, which leads to a cure. The increase in the number of 2014 is probably due to the campaign to detect new cases of the disease (BRASIL, 2015; 2017; 2017a).
The number of leprosy cases shows more visits in the northeast and less in the south (figure 2). According to the literature, this high number of infected in the Northeast is probably due to the high rate of transmission, which occurs during the festive seasons. Time when the basic health units do not work. In the southern region, the probable cause of the low rate of sick people refers to the distance between health services and the patient, making access difficult and contributing to the evolution of the disease, with a high degree of physical disability (ROCHA, 2015).
According to gender, during the years 2010 to 2015, men had a higher incidence of the disease than women (figure 3). When comparing the data with the literature, it is observed that the probable cause of this high index is due to the fact that men are more exposed to the disease than women, taking time to seek health services and abandoning treatment before cure. This makes it susceptible to developing the characteristic deformity of the disease (ARAGOSO et al., 2014; ARANTES et al., 2010).
In terms of occurrence, older individuals predominate among those infected. One of the prevalent factors for this aspect is the incubation time of the bacterium (Mycobacterium leprae), which can extend from two to seven years and, thus, presenting itself in adulthood and, together with that, ends up culminating in possible psychological impairments, since, with the appearance of physical problems – amplified by the delay in diagnosis – the patient may find himself unable to perform his professional activity and, therefore, difficulty in contributing economically in the family context. In addition, with the occurrence of family cases, the chance of children becoming ill may increase (VELÔSO, 2018).
In order to diagnose leprosy, and its consequent classification and staging, several aspects are analyzed. Such verified factors may vary according to the classification used, two of the main ones being Ridley and Jopling’s based on histopathological, clinical, bacilloscopic and immunological characteristics; the classification of the World Health Organization (WHO) uses the bacilloscopic index in its classification, establishing that, if there are a maximum of five lesions at the cutaneous level and nerve trunk, we have Paucibacillary leprosy. If there are more than five lesions, at the cutaneous level and nerve trunk, then there is multibacillary leprosy. However, if there is availability to perform bacilloscopy on the patient and the positive result is contacted, the classification is automatically based on multibacillary (LASTÓRIA and ABREU, 2012).
Depending on the form of leprosy manifestation, various affections may be physically present in the infected individual whose bacillus is active, among them: granulomatous lesions (which may appear in different formats, such as nodules or papules), edema, symptoms caused when nerve trunks are affected (such as muscle atrophy, weakness and pain), immunological problems, sensory, motor weaknesses, acute and systemic inflammatory processes and other implications for the organism (PESSOA, 2019).
Leprosy, in order that it does not trigger serious afflictions for the individual, must be diagnosed early, using the clinical logic and recommended tests. If the diagnosis occurs late, the implications may be greater. In addition, epidemiology and its respective control are necessary for there to be broad knowledge of the disease’s prevalence situation, thus reflecting on the contingent of cases, because, if the control is not effective, there may be greater spread of the disease and, therefore, a significant increase in the number of cases. The search for medical assistance in the initial stage of the disease culminates in the prevalence of cases belonging to degree zero (in which the muscle segments and their respective sensitivities are preserved, characterizing, in most cases, a good prognosis of the patient) (PESSOA, 2019; BRASIL, 2018).
CONCLUSION
With the advancement of public policies aimed at combating leprosy, based on the early diagnosis and treatment, the number of cases of the disease in Brazil, at a majority level, decreased between the years 2010 to 2015.
Leprosy is more prevalent in males, and the probable cause of this reality is the greater exposure of men to this pathology, since the demand for health services occurs in a less comprehensive way and, in addition, the greater abandonment of the disease. treatment, leading to disease progression and the consequent appearance of the individual’s organic weaknesses.
In addition, the highest rate of patients is found in older age groups, that is, in adults, and the main factor responsible for this is the disease incubation period (which can vary from 2 to 7 years). In view of this, several problems can be triggered at the individual level, such as debilitating and psychological physical disorders, and family, since, with the emergence of weakness, economic difficulties may arise as a result of the loss of paid professional activity.
With a view to reducing the number of cases of the disease in the country and making the diagnosis as early as possible, the clinical findings and tests available for this detection should be analyzed. If the patient is able to have his diagnosis made in the initial stage of the disease, there is usually a good prognosis, and his organic health can be very preserved, maintaining the sensitivity and integrity of his muscle segments.
REFERENCES
ARAGOSO, I.; CARVALHO, R.M.B.; SOUSA, C.M.; VIEIRA, G.D. Hanseníase em Rondônia: incidência e características dos casos notificados, 2001 a 2012. Epidemiologia e Serviços de Saúde, v.23, n.2, Brasília, jun. 2014.
ARANTES, C.K.; FILIPE, M.S.; GARCIA, M.L.R.; NARDI, M.T.; PASCHOAL, V.D.A. Avaliação dos serviços de saúde em relação ao diagnóstico precoce da hanseníase. Epidemiologia e Serviços de Saúde, v.19, n.2, Brasília, jun. 2010.
BRASIL. Ministério da Saúde. Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Guia para o controle da hanseníase. 1ª ed., Brasília (DF): Ministério da Saúde, 2002. Disponível em: <http://bvsms.saude.gov.br/bvs/publicacoes/guia_de_hanseniase.pdf> Acesso em: 24 ago 2017.
BRASIL. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Diretrizes para vigilância, atenção e eliminação da Hanseníase como problema de saúde pública: manual técnico-operacional. 1ª ed., Brasília (DF): Ministério da Saúde, 2016. Disponível em: <http://www.saude.pr.gov.br/arquivos/File/DiretrizesdoManuaTcnicoOperacionaldeHansenase.pdf> Acesso em: 05 set 2017.
BRASIL. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Eliminar a hanseníase é possível: um guia para os municípios. Brasília (DF): Ministério da Saúde, 2015. Disponível em: <http://bvsms.saude.gov.br/bvs/publicacoes/eliminar_hanseniase_possivel_versao_preliminar.pdf> Acesso em: 05 set 2017.
BRASIL. Boletim Epidemiológico. Brasilía DF. Ministério da Saúde. 49, n. 4, 12p. 2018.
FREITAS, A.A. Resposta imune celular e humoral a proteínas recombinantes do Mycobacterium leprae em pacientes com outras dermatoses. Tese (Doutorado) – Universidade Federal de Goiás, Instituto de Patologia Tropical e Saúde Pública, Program de Pós Graduação em Medicina Tropical e Saúde Pública, Goiânia, 2015. Disponível em: <https:// posstrictosensu.iptsp.ufg.br/up/59/o/AlinedeAraujoFreitas_2015_vers%C3%A3ofinal.pdf> Acesso em: 12 set 2017.
LASTÓRIA, J. C; ABREU, M. A. M. M. Hanseníase: diagnóstico e tratamento. Diagn Tratamento, v. 17, n. 4, p. 173-179, 2012.
OLIVEIRA, Ciane Martins de; et. al. A evolução da assistência ao paciente com Hanseníase: dos leprosários à poliquimioterapia. Revista Científica Multidisciplinar Núcleo do Conhecimento. Ano 01, Vol. 06, Ed. 08, pp. 68-80. Agosto de 2016. ISSN: 2448-0959
PESSOA, M. M. S. F. S. Hanseníase no Brasil: Uma revisão literária, nos anos de 2014 a 2019. 45p. Trabalho de Conclusão de Curso (Graduação de Farmácia) – Universidade Federal do Rio Grande do Norte, Rio Grande do Norte, Natal, 2019.
ROCHA, A.C.A.A. Análise da sazonalidade da incidência de hanseníase segundo regiões geográficas, climas e biomas do Brasil. 2015. 82 f. Dissertação (Mestrado em Ciências Ambientais) – Universidade do Estado de Mato Grosso, Programa de Pós-Graduação em Ciências Ambientais, Cáceres/MT.
VELÔSO, D. S. Perfil clínico-epidemiológico da hanseníase no estado do Piauí, no período de 2009 a 2016. 127p. Dissertação (Mestrado em Medicina Tropical) – Instituto Oswaldo Cruz, Piauí, Teresina, 2018.
[1] Mining technician, graduated from the Federal Institute of Amapá (IFAP).
[2] Student of the Medical Course at the Federal University of Amapá (UNIFAP).
[3] Biomedical, PhD in Tropical Diseases, Professor and researcher of the Course of Medicine at the Federal University of Amapá (UNIFAP).
[4] Physician, Professor and researcher of the Medicine Course at the Federal University of Amapá (UNIFAP).
[5] Biologist, Doctor in Topical Diseases, Professor and researcher of the Physical Education Course at the Federal University of Pará (UFPA).
[6] Theologian, PhD in Psychoanalysis, researcher at the Research and Studies Center Advanced – CEPA.
[7] Sociologist, Master’s student in Anthropic Studies in the Amazon, Member of the Research Group “Laboratory of Education, Environment and Health (LEMAS / UFPA).
[8] Biologist, PhD in Theory and Research of Behavior, Professor and researcher of the Pos-Graduate Program in Professional and Technological Education (PROFEPT), Federal Institute of Amapá (IFAP).
Submitted: November, 2020.
Approved: November, 2020.















