ORIGINAL ARTICLE
MORAES, Inaldo Kley do Nascimento [1], OLIVERIA, Sara Coelho [2], DIBAI, Daniela Bassi [3], DIAS, Rosane da Silva [4]
MORAES, Inaldo Kley do Nascimento. Et al. Evaluation of patient safety culture in the hemodynamics sector in a private hospital in São Luís – MA. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 05, Ed. 07, Vol. 02, pp. 43-56. July 2020. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/health/safety-culture, DOI: 10.32749/nucleodoconhecimento.com.br/health/safety-culture
ABSTRACT
Patient safety is understood as reducing to the minimum acceptable risks of damage associated with health care. This depends on a safety culture formed from a qualified and safe service, involving all hospital professionals, and constant monitoring of the determining factors for quality health care. The general objective of the study was to evaluate the culture of patient safety in the hemodynamics sector in a private hospital in São Luís. This is a cross-sectional, descriptive, quantitative study conducted in the hemodynamic sector of the cardiology center of Hospital São Domingos, through the HSOPSC – Hospital Survey on Patiente Safety Culture questionnaire divided into 12 dimensions, the perception of each of them is described by the percentage of positive responses. Participants were 69 professionals, of which 47 (68%) were women, 16 (23%) were nurses, 30 (43%) worked in the hospital between 1 and 5 years, 33 (48%) with weekly workload between 20 and 39 hours. Regarding the dimensions evaluated the “Expectations on the supervisor/boss” (79%); “Organizational learning / continued improvement” (90%); “Teamwork within the unit” with (78%) and “hospital management support” (91%) considered strong. In addition, 52 (68%) participants reported not having submitted or completed any adverse event reports in the last 12 months. Therefore, the patient safety culture of the sector has potential for improvement in almost all dimensions evaluated.
Keywords: Adverse events, risk management, patient safety, patient safety culture, care.
1. INTRODUCTION
In recent years the importance of an effective safety culture has been gaining increasing attention from the field of health organizations, as it is essential in the hospital environment in an attempt to improve health care, and thus reduce the risks of adverse events. Since, due to the increased complexity of health care, the chances of incidents, errors and failures became higher (REIS, 2013).
It is important to point out that patient safety is understood to reduce to the minimum acceptable risks of damage associated with health care (BRASIL, 2013). This depends on a safety culture formed from a qualified and secure service, defined from team and individual behavior regardless of the hierarchical position occupied (ALVES et. al., 2015; OLIVEIRA et. al., 2014).
In order to improve the culture of patient safety in Brazil, the Ministry of Health in 2013 created the Institution of the National Patient Safety Program (PNSP), with the objective of preventing, monitoring and reducing the damage and errors caused to patients during health care through the implementation of risk management and patient safety centers in the various areas of care , management and organization of health services (BRASIL, 2013).
During the first 3 years after the creation of the PNSP, a total of 2,333 Patient Safety Centers (NSP) were implanted in the country. In the same period, it was possible to observe a significant increase in the number of reports of adverse events (BRASIL, 2016). During the period from January 2014 to July 2017, an ANVISA reported a total of 50,735 incidents related to health care, and in hemodialysis services 224 incidents were reported (BRASIL, 2017).
Among the damages caused to the patient due to failure to provide health care, we highlight the increase in hospital stay, hospital costs, the need for new interversions, social costs, emotional damage and, in more severe cases, death (SIMAN; CUNHA; BRITO, 2017; MILAGRES, 2015). In addition, the health professionals involved due to the lack of understanding and the punitive character still existing in some institutions may feel guilty, afraid, ashamed and embarrassed. This fact contributes to them not noting the adverse event that occurred (DUARTE et. al., 2015; DIAS et al., 2014).
In a study conducted by Neves (2017), with the objective of evaluating hemorrhages in patients undergoing cardiac catheterization, found that of the 616 cases included in the study, in 95 there were bleeding events (15.4%) up to 1 hour after catheterization in the first evaluation and 343 bleeding events (55.7%) up to 48 hours during the second evaluation; in addition, 9 (1.5%) deaths were recorded up to the first hour after catheterization and 12 (1.9%) up to 48 hours after catheterization. This shows a high number of hemorrhagic events.
Although institutions are committed to providing better patient care and reducing adverse events through safety measures and protocols that ensure this effect. Sectors that perform invasive procedures, such as the hemodynamics sector, do not have well-defined protocols as opposed to what are observed in the emergency and emergency, (UTI – Intensive care unit) and CDI sectors that have protocols already established.
Thus, considering the importance that the discussion of the theme has for safer patient care and aiming to contribute to the reduction of risks and negative impacts that adverse events bring in different aspects in the life of the patient and health professionals, the present study aimed to evaluate the culture of patient safety in the hemodynamics sector in a private hospital in São Luís (MA).
2. METHODOLOGY
This is a cross-sectional study, descriptive with a quantitative approach, carried out in the hemodynamics sector of the Hospital São Domingos in São Luís – MA. This is considered a hospital of high complexity, due to the technology employed in procedures and the services provided in all areas of medicine, performing major surgeries, vascular, urological, oncological, clinical emergencies, surgical, cardiology, cardiac surgeries, nephrology, neurology, traumatology.
The sampling was non-probabilistic, it was for convenience, considering the staff of professionals in the sector. It was used as inclusion criterion to be working in the sector regardless of the length of service and as an exclusion criterion to be away for medical leave, during vacation and the questionnaires filled out in the wrong way to the point of impairing the analysis of the variables. Eight questionnaires were disregarded for meeting the last exclusion criterion, resulting in a sample of 69 professionals.
To evaluate the safety culture of professionals, the HSOPSC – Hospital Survey on Patiente Safety Culture, created by the Agency for Health Care Research And Quality (AHRQ) and validated in Brazil by Reis (2013) was used. The HSOPSC consists of questions about patient safety, adverse events, leadership, communication and management, makes it possible to know the perception about the work unit, and in general about the entire institution, emphasizes errors, perceptions of errors and dimensions of the patient safety culture (REIS, 2013).
It consists of 42 questions divided into 12 dimensions, which are: Frequency of events notified; Perception of security; Expectations about supervisor/ boss; Organizational learning / continued improvement; Teamwork in the unit; Opening of communication; feedback and communication about errors; Non-punitive response to errors; adequacy of professionals; Support of hospital management; Teamwork between units and passage of shifts / transfers. In addition to the 12 dimensions, the HOSPSC has questions regarding the number of notifications of safety incidents, general note of patient safety and work aspects of professionals.
The possibilities of answers to each question were based on the likert type of 5 alternatives: (1=strongly disagree, 2=slightly disagree, 3=neither disagree nor agree or sometimes, 4=agree slightly and 5=strongly agree). For the interpretation of the data, the scores of each item were converted into a score that totals 100 points, considered desirable. Thus, the scores began to assume the following values: Strongly disagree=0, disagree slightly=25, neutral=50, agree slightly=75 and strongly agree=100. Some items have a reverse score, that is, in these questions a reduced score represents a positive attitude.
The percentage of positive responses for each dimension was obtained using the following formula (SORRA; NIEVA, 2004, p. 35): “% of positive responses from dimension X = [number of positive responses to items in dimension X / total number of responses valid for items in dimension X (positive, neutral and negative, excluding missing data)] x 100 ”
The percentage of positive responses allows the identification of strong and fragile areas in patient safety. The dimensions that obtained more than 75% of positive responses were considered “strong areas of patient safety” in the hospital. Similarly, “fragile areas of patient safety” and which need improvements, those that obtained 50% or less of positive responses (REIS, 2013).
The data were evaluated by the IBM SPSS Statistics 20 program (2011). The descriptive data of categorical variables were presented by absolute frequency and percentages.Then, the mean and 95% confidence interval (95% CI) were estimated. percentage of positive responses from each of the 12 dimensions of the safety culture.
After agreeing to participate in the research, each participant received a copy of the instrument and two copies of the Informed Consent Form (TCLE). After signing the TCLE by the participant, he received one copy and the other was held by the researcher. This research was approved by the Ethics Committee in Research with Human Beings of the CEUMA University Under the opinion 3.107.901.
3. RESULTS
The study included 69 professionals. Of these 47 (68%) were female, as the age group was predominance of individuals aged between 31 and 40 years. Among the professionals who answered the survey, 15 (22%) were doctors, 16 (23%) nurses, 15 (22%) nursing technician, 9 (13%) radiology technicians, 9 (13%) administrative assistant, 4 (6%) hospitality and 1 (1%) psychologist ( Table 1).
Table 1. Sociodemographic data of the professionals participating in the study, Maranhão, Brazil, 2019 (N= 69).
| Variables | N | % |
| sex | ||
| female | 47 | 68 |
| male | 22 | 32 |
| age | ||
| From 19 to 30 years | 27 | 39 |
| From 31 to 40 years | 28 | 41 |
| From 41 to 50 years | 12 | 17 |
| From 51 to 64 years old | 2 | 3 |
| profession | ||
| doctor | 15 | 22 |
| nurse | 16 | 23 |
| Nursing technician | 15 | 22 |
| Radiology technician | 9 | 13 |
| Administrative assistant | 9 | 13 |
| Hotel | 4 | 6 |
| psychologist | 1 | 1 |
| Total | 69 | 100 |
Source: Prepared by the author (2019).
The variables working time in the specialty, length of work in the hospital and working time in the unit there was a predominance of responses for the period from 1 to 5 years with respective percentages of 28 (41%); 30 (43%) and 36 (52%). As for weekly workload, 33 (48%) reported between 20 and 39 working hours (Table 2).
Table 2. Professional characteristics of the study participants, Maranhão, Brazil, 2019 (N= 69).
| Variables | N | % | |||
| Direct patient contact | |||||
| Yes | 60 | 87 | |||
| No | 9 | 13 | |||
| Working time in the current specialty/profession | |||||
| Less than 1 year | 7 | 10 | |||
| From 1 to 5 years | 28 | 41 | |||
| From 6 to 10 years | 22 | 32 | |||
| From 11 to 15 years | 7 | 10 | |||
| 21 years or older | 5 | 7 | |||
| Working time in this hospital | |||||
| Less than 1 year | 6 | 9 | |||
| From 1 to 5 years | 30 | 43 | |||
| From 6 to 10 years | 24 | 35 | |||
| From 11 to 15 years | 4 | 6 | |||
| From 16 to 21 years or older | 5 | 7 | |||
| Working time in the current area/unit | |||||
| Less than 1 year | 12 | 17 | |||
| From 1 to 5 years | 36 | 52 | |||
| From 6 to 10 years | 22 | 32 | |||
| From 11 to 15 years | 3 | 4 | |||
| From 16 to 21 years or older | 4 | 6 | |||
| Weekly workload | |||||
| Less than 20 hours | 8 | 12 | |||
| Between 20 and 39 hours | 33 | 48 | |||
| Between 40 and 59 hours | 21 | 30 | |||
| Between 60 and 79 hours | 3 | 4 | |||
| Between 80 and 100 hours or more | 4 | 6 | |||
| Total | 69 | 100 | |||
Source: Prepared by the author (2019).
Regarding the dimensions evaluated, four of them appear with a strengthened culture assessment, because they have more than 75% of positive responses, they are: “Expectations about the supervisor/ boss” (79%); “Organizational learning/ continuous improvement” (90%); “Teamwork within the unit” (78%) and “Hospital management support” with (91%). On the other hand, the dimension “Non-punitive response” with (48%) it was considered an area of fragility of patient safety, because it had less than 50% of positive responses (Table 3).
Table 3. Number of positive responses for each dimension of the HSOPSC questionnaire and its respective percentages, averages and 95% IC, Maranhão, Brazil, 2019 (N=69).
| Dimensions | N | % | average | IC 95% |
| D1 – General perception of safety | 172 | 62 | 43 | 39,91-46,09 |
| D2 – Frequency of event reports | 121 | 59 | 40,3 | 37,76-42,91 |
| D3 – Expectations about the supervisor/ boss* | 217 | 79 | 54,25 | 50,78-57,72 |
| D4 – Organizational learning/ continued improvement* | 187 | 90 | 62,3 | 59,12-65,54 |
| D5 – Teamwork within the unit* | 214 | 78 | 53,5 | 50,06-56,94 |
| D6 – Opening of communication | 105 | 51 | 35 | 32,62- 37,38 |
| D7 – Non-punitive answers+ | 99 | 48 | 33 | 30,66-35,34 |
| D8 – Adequacy of professionals | 178 | 65 | 44,5 | 41,36-47,64 |
| D9 – Return of information and communication | 141 | 68 | 47 | 44,22-49,78 |
| D10 – Hospital management support * | 188 | 91 | 62,6 | 59,46-65,88 |
| D11 – Teamwork between units | 201 | 73 | 50,25 | 46,92-53,58 |
| D12 – Shift ing / transfers | 167 | 61 | 41,75 | 38,73- 44,77 |
+ Dimensions that present weaknesses (D7); * Dimensions that present strongholds (D3; D4; D5 and D10).
Source: Prepared by the author (2019).
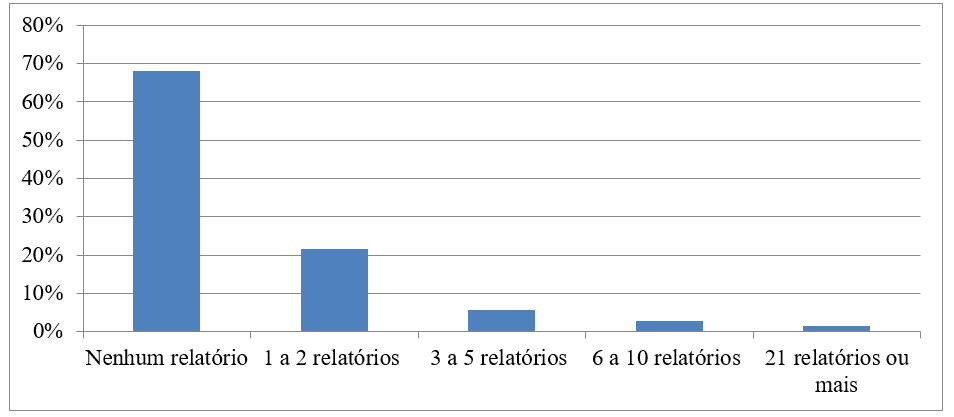
Regarding the notification of adverse events, 47 (68%) participants reported not having submitted or completed any adverse event reports in the last 12 months. The highest number of reports sent among participants was between 1 and 2 reports, 15 (22%) participants fit into this category (Graph 1).
Graph 1. Number of adverse event reports completed and submitted in the last 12 months, Maranhão, Brazil, 2019 (N=69).

Regarding the assessment of the degree of safety, 43 (62%) participants considered it very good, 16 (23%) considered it excellent, 9 (13%) assessed the safety of the sector as satisfactory and the minority 1 (1%) evaluates as bad (Graph 2).
Graph 2. Evaluation of the degree of safety in the hemodynamic sector, according to the participants, Maranhão, Brazil, 2019 (N=69).
4. DISCUSSION
The results of the present study showed potential for improvement in the patient safety culture in the hemodynamics sector in almost all dimensions evaluated, since only 4 of the 12 dimensions evaluated were classified as strengthened, because they obtained more than 75% of positive responses.
The dimension “non-punitive response to errors” also classified as weak in the studies conducted by Andrade et al. (2018); Santiago and Turrini (2015) and Mello and Barbosa (2013) in which the dimension received (36.1%), (18%) and (18%) positive responses, respectively. In addition, 32 (46%) of the participants of the present study answered that they “agree” or “totally agree” with the item “professionals consider that their mistakes can be used against them” which composes the dimension, which suggests the presence of a punitive character in the sector.
The analysis of the section that investigated the number of adverse events reported in the last 12 months by the participants affirms this thought, given the fact that 47 (68%) of the team report not having reported any reports in the last 12 months. Similar results were found in a study conducted in an intensive care unit in which the Survey on Patient Safety in Hospitals questionnaire, also used in the present research, alerted to underreporting of adverse events in which most professionals had not made notifications during the period studied, which may be influenced by the punitive culture that may influence new notifications and improvements in patient safety (MINUZZ; SALUM; LOCKS, 2016).
Moreover, although, according to the professionals, they frequently report adverse events that occurred in the sector in cases where the error is identified and corrected before affecting the patient and when errors occur with potential or without harming the patient, the results found in the dimension “Frequency of event reports” contradict those found in the number of notifications made in the last 12 months in which a low number of reports were observed. In a study developed by Costa (2014), in two public hospitals in Paraná, with 282 professionals, he found similar results in which (77.8%) of the professionals had not been notified in the last 12 months and according to the dimension “Frequency of event reports” employees frequently reported existing errors. This fact demonstrates the importance of encouraging notification and guidance on how to perform it properly so that the perception of employees and the number of reports made are equated.
The high percentage of positive responses (90%) the dimension “Organizational learning/ continuous improvement” and “Hospital management support” (91%) demonstrates that professionals perceive the existence of continuous improvement measures in the institution aimed at improving and empowering them (WEGNER et al., 2016). (86,9%) of the professionals responded positively to the item “errors have led to positive changes here” that make up the dimension “Organizational learning/ continuous improvement”, demonstrating a positive view on this characteristic.
Although not classified as strong, the dimension “Return of information and communication” received a significant percentage of positive responses (68.1%) compared to those found in the literature, as in the studies by Mello and Barbosa (2017) and Minuzzi et. Al. (2016) who obtained respectively (27.1%) and (20.81%) of positive responses to this dimension, composed of the items “we receive information about changes implemented from the event reports”, “we are informed about the errors that happen in this unit” and “in this unit we discuss ways to prevent errors by preventing them from happening again”. This suggests that, even with a possible notification deficit, those that are performed are used in order to avoid recurrence.
Another point that differs from the data found in the literature discerns about the patient’s safety assessment and the dimension “general perception of safety”, both with percentages of (62%) for very good. In studies conducted by Mello and Barbosa (2017), in two adult UTI of public hospitals, in which the response of (77.7%) for the degree of safety was very good/acceptable, diverging from the low percentage of positive responses of the dimension “perception of the degree of safety” (25.9%). Just like Tomazoni et. al. (2015), in a descriptive-exploratory study in four neonatal UTI, in the state of Santa Catarina, brazil, with a sample of 181 professionals. It was observed that the safety level was assessed was (83%) for very good and acceptable already the dimension received (36%) positive responses.
According to Mello e Barbosa (2017), the discrepancy in the aforementioned studies is due to the perception of professionals that there are problems in patient safety, which culminates in a worse assessment of patient safety, however, if the patient has a positive perception about the preventive measures of errors the evaluation will be positive. Another justification would be the fact that the two studies were conducted in public hospitals while the present study was conducted in a private hospital of high complexity.
Comparative study conducted by Andrade et al. (2018), in hospitals with different types of management – federal, state and private- observed that the factors work overload and infrastructure deficits in addition to complaints from managers themselves regarding insufficient funding for the acquisition of insum, medicines and equipment would be possible justifications for only the private hospital to have reached levels of strength (>75%) positive responses. This may justify the difference between the findings in the literature and the results of the present study.
The fact that the dimensions “Expectations on the supervisor/ boss” (79%) have been classified as strengthened and the expressive percentage of positive responses attributed to the dimension “Teamwork between units” (73%) suggests that the team feels supported within the unit by its supervisors besides demonstrating to be a harmonic work environment in which professionals are willing to help co-workers in the face of adversity (MELLO; BARBOSA, 2013).
Studies aimed at the study of the patient safety culture in the hemodynamics sector are still rare in the literature.Because it is an area that offers risks, both to the patient and to the professional, it should be improved explored. Since, it is an environment with risk of contamination by microorganisms, accidents with sharp tools, high emotional and mental load that together are characterized as a set of sector-specific risks (NASCIMENTO, 2013).
In the present study it was possible to observe that, although it has percentages of positive responses higher than those found in other studies, the sector has areas with potential for improvement. Mainly, in the need for a non-punitive culture, which stimulates notifications so that it is possible to know and combat more efficiently the causes and consequences of errors and adverse events of the sector (SOUZA et. al., 2015).
5. FINAL CONSIDERATIONS
Through this research it was possible to identify that the sector is mostly made up of women, with a predominance of individuals aged between 31 and 40 years and medical professionals, nurses and nursing technicians. Although it presents better results when compared to the literature explored, the sector shows potential for improvement in most aspects studied since only 4 of the 12 dimensions were classified as strengthened. In addition, there was a low rate of notifications in the sector, which contradicts the perception of professionals regarding the frequency of notifications. This fact may have been directly influenced by the punitive culture present in the sector.
The results found can guide the development of new strategies in order to solve the underreporting of the sector and the punitive nature of the notifications that are made so that they can know the adverse events of the sector and avoid recurrences and have as a consequence the improvement in the culture of patient safety in the sector.
It is suggested the development of new research on patient safety in the hemodynamic sector given its importance and lack in the literature of articles addressing this subject.
6. REFERENCES
ALVES, Kisna Yasmin Andrade; SANTOS, Viviane Euzébia Pereira; DANTAS, Cilene Nunes .A análise do conceito segurança do paciente: a visão evolucionária de Rodgers. Aquichan, Chía, v. 15, n. 4, p. 521-528, 2015.
ANDRADE, Luiz Eduardo Lima et. al., Cultura de segurança do paciente em três hospitais brasileiros com diferentes tipos de gestão. Ciênc. Saúde Colet., v.23, n.1, p. 161-172, 2018. Disponível em:< https://www.scielosp.org/article/csc/2018.v23n1/161-172/pt/>. Acesso 12/08/ 2019.
BRASIL. Agência Nacional de Vigilância Sanitária. Assistência Segura: Uma Reflexão Teórica Aplicada à Prática Agência Nacional de Vigilância Sanitária. 2 ed. Brasília: ANVISA, 2017. Disponível em: <http://portal.anvisa.gov.br/documents/33852/3507912/Caderno+1+-+Assist%C3%AAncia+Segura++Uma+Reflex%C3%A3o+Te%C3%B3rica+Aplicada+%C3%A0+Pr%C3%A1tica/97881798-cea0-4974-9d9b-077528ea1573> Acesso em: 24/08/ 2019.
BRASIL. Ministério da saúde. Núcleo de segurança do paciente, Abr. 2016. Disponível em:< http://www.saude.gov.br/acoes-e-programas/programa-nacional-de-seguranca-do-paciente-pnsp/nucleo-de-seguranca-do-paciente> Acesso em: 23/08/ 2019.
Brasil. Ministério da Saúde. Portaria GM/MS nº 529, de 1º de abril de 2013.
COSTA ,Daniele Bernardi da. Cultura de segurança do paciente em serviços de enfermagem hospitalar. 2014. 98f. Dissertação (mestre em saúde)- Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto,2014. Disponível em: <https://www.teses.usp.br/teses/disponiveis/22/22132/tde-06022015-192856/pt-br.php>. Acesso em 07/08/2019.
DIAS, Jéssica David et al. Compreensão de enfermeiros sobre segurança do paciente e erros de medicação. Rev Min Enferm., Belo Horizonte, v.18, n.4, p 866-873; out./dez. 2014.Disponível em:< https://www.reme.org.br/artigo/detalhes/969> Acesso em 07/08/2019.
DUARTE, Sabrina da Costa Machado et al. Eventos adversos e segurança na assistência de enfermagem. Rev Bras Enferm,Rio de Janeiro, v. 68, n. 1, p. 144-154, 2015.
MELLO, Janeide Freitas de,BARBOSA, Sayonara de Fátima Faria. Cultura de segurança do paciente em terapia intensiva: recomendações da enfermagem. Texto & contexto enferm., Florianópolis,v.22, n. 4,p. 1124-1133, Out./Dez., 2013.
MELLO, Janeide Freitas; BARBOSA, Sayonara Fátima Faria. Cultura de segurança do paciente em unidade de terapia intensiva: perspectiva da equipe de enfermagem. Rev. eletrônica enferm., Goiania v. 19, 2017.
MILAGRES, L. M. Gestão de riscos para segurança do paciente: o enfermeiro e a notificação dos eventos adversos. 2015. 80f. Dissertação (mestre em Tecnologia e comunicação no cuidado em saúde e enfermagem) – Universidade Federal de Juiz de Fora, Juiz de Fora, 2015. Disponível em: :<http://www.ufjf.br/pgenfermagem/files/2010/05/Disserta %C3%A7%C3%A3o-Lidiane-Miranda-Milagres.pdf/>. Acesso 12/08/ 2019.
MINUZZI, Ana Paula; SALUM, Nádia Chiodelli, LOCKS; Melissa Orlandi Honório. Avaliação da cultura de segurança do paciente em terapia intensiva na perspectiva da equipe de saúde. Texto & contexto enferm., , v.25,n.2. 2016.
NASCIMENTO, Vidal do Nascimento; CARVALHO, Yanara Pinheiro; SOUSA, Pryscila Correia de. Conhecimento dos riscos do setor de hemodinâmica: uma investigação com profissionais de saúde. In: seminário nacional de pesquisa em enfermagem,17,2013,Natal.Anais do 17° SENPE,RN:ABEn.p.1834-1836, 2013.
NEVES, Marta Isabel Cláudio. Eventos hemorrágicos no doente submetido a cateterismo cardíaco. 2017. 94f. Dissertação (mestre em Engenharia Biomédica) – Instituto Superior de Engenharia de Lisboa – Escola Superior de Tecnologia da Saúde de Lisboa,Lisboa, 2017. Disponível em:< https://repositorio.ipl.pt/handle/10400.21/8356> Acesso em: 16/10/2019.
OLIVEIRA, Roberta Meneses et al. Estratégias para promover segurança do paciente: da identificação dos riscos às práticas baseadas em evidências. Esc Anna Nery, Rio de Janeiro, v. 18, n. 1, p. 122-129, 2014.
REIS, Claudia Tartaglia. A cultura de segurança do paciente: validação de um instrumento de mensuração para o contexto hospitalar brasileiro. 2013.217f. Tese (Doutorado em ciências na área de saúde pública) – Escola Nacional de Saúde Pública Sergio Arouca, Rio de Janeiro, 2013. Disponível em:<https://www.arca.fiocruz.br /handle/icict/14358> Acesso em: 11/08/2019.
SANTIAGO, Thaiana Helena Roma ; TURRINI, Ruth Natalia Teresa . Cultura e clima organizacional para segurança do paciente em Unidades de Terapia Intensiva. Rev. Esc. Enferm. USP., São Pauo, p. 123-130, 2015.
SIMA N, Andréia Guerra ; CUNHA, Simone Graziele Silva; BRITO, Maria José Menezes. A prática de notificação de eventos adversos em um hospital de ensino. Rev esc enferm USP, São Paulo, v. 51, 2017.
SORRA, Joann; NIEVA, Veronica. Survey on Patient Safety Culture. Rockville, MD: Agency for Healthcare Research and Quality, 2004.
SOUZA, Verusca Soares de et al. Erros e eventos adversos: a interface com a cultura de segurança dos profissionais de saúde. Cogitare enferm., Curitiba, v. 20, n. 3,p. 475-482, 2015.
TOMAZONI, Andréia et al. Avaliação da cultura de segurança do paciente em terapia intensiva neonatal. Texto & contexto enferm., Florianopolis v. 24, n. 1, p. 161-169, 2015.
WEGNER, Wiliam et al. Educação para cultura da segurança do paciente: Implicações para a formação profissional. Esc Anna Nery , Rio de Janeiro, v. 20,n.3, 2016.
[1] Master’s degree in Health Program sand service management, specialist in Cardiology and hemodynamics nursing, nurse.
[2] Physiotherapy student.
[3] PhD in Physiotherapy, Master in Physiotherapy, graduated in physiotherapy.
[4] Guidance counselor. PhD in Health Sciences, Specialization in traumatology and orthopedics, graduated in physiotherapy.
Submitted: May, 2020.
Approved: July, 2020.