ORIGINAL ARTICLE
ALVES, Giovana Carvalho [1], OLIVEIRA, Kamila Freitas de [2], GUIMARÃES, Amanda Wosny [3] FECURY, Amanda Alves [4], REGO, Natássia Maia de Sá [5], OLIVEIRA, Euzébio de [6], DENDASCK, Carla Viana [7], DIAS, Claudio Alberto Gellis de Mattos [8]
ALVES, Giovana Carvalho. Et Al. Frequency Of Aids Cases Identified In Brazil Between 2012 And 2016. Revista Científica Multidisciplinar Núcleo do Conhecimento. 04 Year, Ed. 05, Vol. 03, pp. 37-44, May de 2019. ISSN: 2448-0959
ABSTRACT
Introduction: Acquired immunodeficiency syndrome (AIDS) is caused by a virus. Reproduction of this invader in the body causes failure of the defense system. The most common form of transmission is by unprotected sexual activity and sharing with used syringes. There are several symptoms that can manifest in people with HIV (fever, diarrhea, night sweats, opportunistic diseases and weight loss). Treatment of people infected with the HIV virus is usually done using drugs called antiretrovirals. Aim: This study aims to show the frequency of AIDS cases identified in Brazil between 2012 and 2016. Method: This research was carried out in the database DATASUS (http://datasus.saude.gov.br/). Data were collected referring to regions of Brazil, gender, age group, schooling, and race/color. Results: The highest mean frequency of cases appears in the data from the Brazilian Southeast region (10,286), followed by the South region (6,260), Northeast region (5,916), North region (2,522) and Midwest region (2,007). The highest percentage of the frequency of cases was in the age group of 20 to 49 years (79.02%), followed by 50 to 64 years (15.13%), 65 or more years (2.28%), 15 to 19 years (2.38%) and 0 to 14 years (1.19%). The frequency of cases was higher in males. From 2012 to 2013 there was an increase in the number of cases in the male gender (from 19,920 to 20,244) and in the years 2013 to 2016 there was a decrease (from 20,244 to 15,242). In the female gender there was a decrease from 2012 to 2016 (from 10,545 to 6,346), almost half of the initial value of this sex. The ethnic brown group had a larger number of cases (44.39%), followed by white (44.15%), black (10.70%), yellow (0.44%) and indigenous (0.32%). The frequency of cases was higher in complete brazilian secondary education (23.80%), followed by incomplete 5th to 8th grade (21.10%), elementary school (11.93%), complete college education (9.88%), incomplete 1st to 4th grade (8.42%), the complete 4th grade (6.74%), the incomplete college (5.88%) and the unlettered (2, 79%). Conclusion: If effective health education, awareness of risk behaviors, decentralization of outpatient services and coordination and communication among health professionals is possible, there would probably be a decrease in new cases of HIV / AIDS in Brazil.
Keywords: Epidemiology, HIV, AIDS, Health
INTRODUCTION
Acquired immunodeficiency syndrome (AIDS) is caused by a virus. Reproduction of this invader in the body causes failure of the defense system. This can cause other diseases to settle and, as a consequence, reduce the life expectancy of infected humans (Menezes et al., 2019).
One form of virus transmission is called vertical transmission. It occurs when there is a high amount of this microorganism in the maternal blood. Mother-to-child transmission can occur during pregnancy, childbirth and breastfeeding (Goga et al., 2019). The most common form of transmission is by unprotected sexual activity and sharing with used syringes. Contact of blood with HIV to the mucous membranes of a healthy person, such as the vagina, rectum, penis and mouth, can lead to infection of the person (CDC, 2018).
While the carrier is without obvious symptoms (asymptomatic), the virus attacks the body’s defense cells, increasing the individual’s chance of presenting common diseases such as fever, diarrhea, night sweats and weight loss. Also, in the so-called acute infection, flu-like symptoms such as fever and malaise may occur. In the phase called AIDS, opportunistic microorganisms can take advantage of the fragility of the infected individual’s immune system, causing opportunistic diseases or intensifying their clinical conditions, among them: viral hepatitis, tuberculosis and pneumonia (Brazil, 2019).
Treatment of the infected is usually done using drugs called antiretrovirals. They are responsible for controlling the replication of the virus, reducing its amount in the blood, providing an improvement in the health and well-being of the patient. Medication should be started as soon as possible after diagnosis. Some side effects can be expected, such as: nausea, vomiting, diarrhea, difficulty sleeping, headache, itching and dizziness. This treatment can also be used preventively (USA, 2019).
By 2016 there were 36.7 million people infected with the HIV virus in the world. Of these, 19.5 million had access to treatment. The result was a fall in the number of deaths in 900 thousand people. The highest rates of contamination occur in Eastern and Southern Africa (UNAIDS, 2017).
In Brazil, up to June 2017, it was estimated that there were 194,217 cases of HIV infection. In 2016, of the 37,884 reported cases, 3,912 (10.3%) occurred in the brazilian North region, 7,693 (20.3%) in the Northeast region, 15,759 (41.6%) in the Southeast region, 7,688 (20.3%) in the and 2,832 (7.5%) in the Center-West region of the country. In the same year, the number of cases by gender was 131,969 (67.9%) cases in men and 62,198 (32.1%) cases in women (Brazil, 2017).
AIM
Show the frequency of AIDS cases identified in Brazil between 2012 and 2016.
METHOD
The research was carried out in the database DATASUS (http://datasus.saunnde.gov.br/). National data were collected according to the following steps: The item “Acesso à Informação“, followed by “Informações de Saúde (TABNET)“, “Epidemiológicas e Morbidade” was selected. A new page was opened, and in it, “Casos de AIDS – Desde 1980 (SINAN)” was selected. On the open page we selected the item “AIDS – desde 1980“. On the same page a map of the national territory appeared in the upper right corner, and in the selection box under the map, left-clicked and “Brasil por região, UF ou Município” was selected in the list. A new window opened. In the “linha” box was selected “Ano de Notificação“, in the “coluna” box was selected “Região de Residência“, and in the “conteúdo” box was selected “Frequencia“. The data collected between the years 2012 and 2016, selected, one by one, from the “available periods” box. The other data were collected by changing the selection of the “coluna” box and setting the boxes “linha” and “conteúdo“. The other selections made in the “coluna” box were: : “Faixa Etária (SINAN)”, “Sexo”, “Raça/Cor” e “Escolaridade”. The data was compiled into the Excel program component of the Microsoft Office suite.
RESULTS
The average frequency of AIDS cases in Brazil, by region, between 2012 and 2016 can be observed in Figure 1, with the highest values being those of the Southeast region, followed by the South, Northeast, North and Central-West regions of Brazil.
Figure 1 Shows the average frequency of AIDS cases in Brazil, by region, between 2012 and 2016.
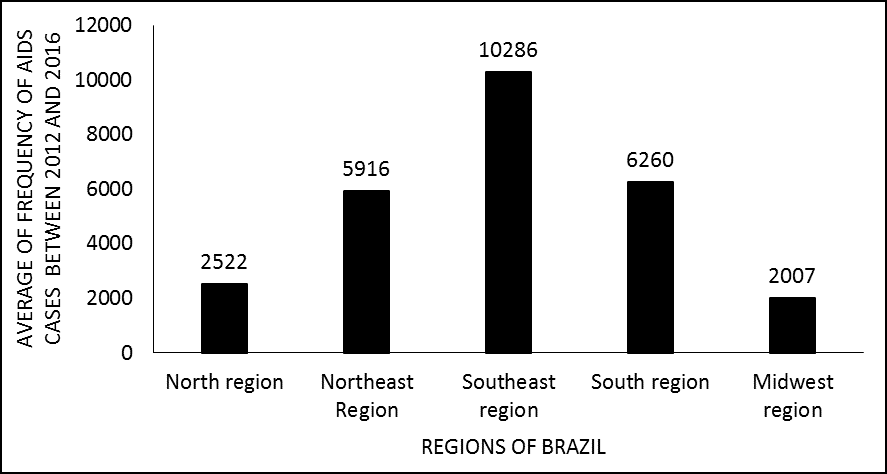
Figure 2 shows the percentage of AIDS cases in Brazil, by age group, between 2012 and 2016. The highest values were in the 20 to 49 years age group, followed by 50 to 64 years, 65 or more years, 15 to 19 years and 0 to 14 years.
Figure 2 Shows the percentage of AIDS cases in Brazil, by age group, between 2012 and 2016.
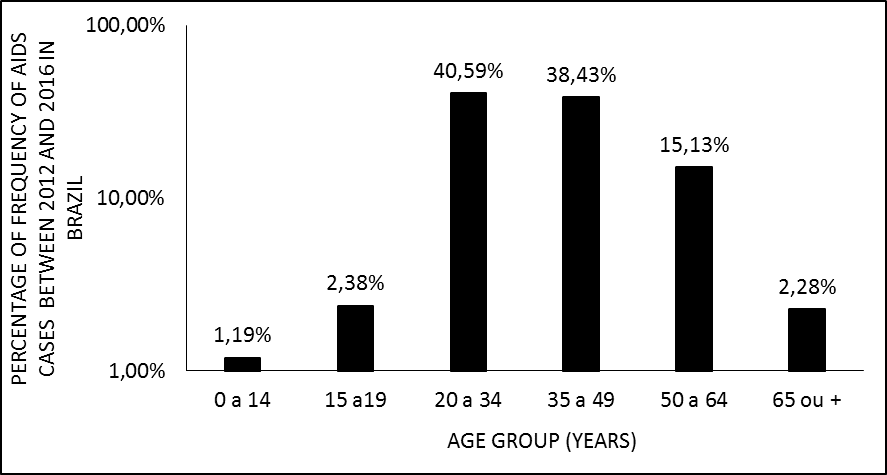
Figure 3 shows the frequency of AIDS cases in Brazil, by gender, between 2012 and 2016. The highest percentage of cases was in the male gender. From 2012 to 2013 there was an increase in the number of cases in the male gender and in the years from 2013 to 2016 there was a decrease. In the female gender there was a decrease from 2012 to 2016, almost half of the initial value of this genre.
Figure 3 Shows the frequency of AIDS cases in Brazil, by gender, between 2012 and 2016.
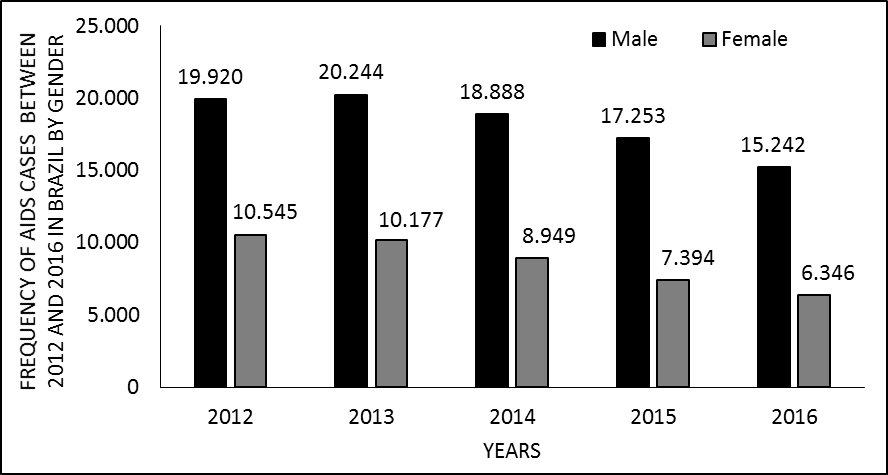
Figure 4 shows the percentage of AIDS cases in Brazil, by ethnicity (race/color), between 2012 and 2016. The ethnic brown group, followed by white, black, yellow and indigenous, had the highest values.
Figure 4 Shows the percentage of the frequency of AIDS cases in Brazil, by ethnicity (race/color), between 2012 and 2016.
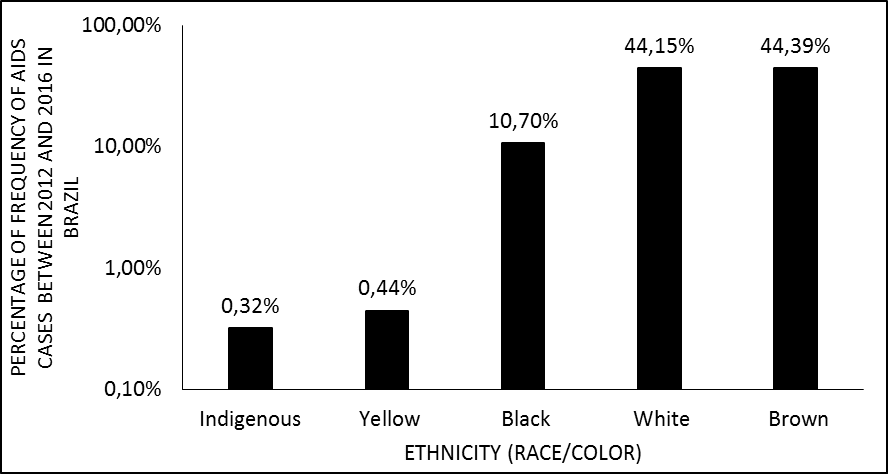
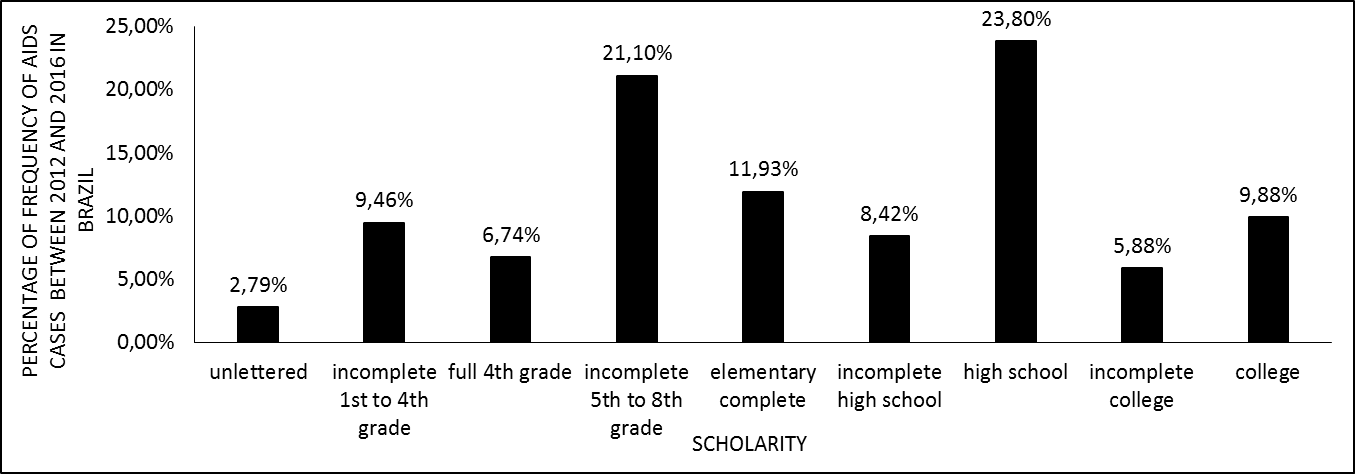
Figure 5 shows the percentage of the frequency of AIDS cases in Brazil, by scholarity, between 2012 and 2016. The highest percentage of case frequency was in high school, followed by incomplete 5th to 8th grade, elementary complete, college, incomplete 1st to 4th grade, incomplete high school, full 4th grade, incomplete college and unlettered.
Figure 5 Shows the percentage of AIDS cases in Brazil, by scholarity, between 2012 and 2016.
DISCUSSION
The 2016 data on people with AIDS by region (Brazil, 2017) accompany data from the Brazilian Institute of Geography and Statistics referring to the regional population in the period (IBGE, 2017). However, the results (figure 1) differ in relation to what concerns the northeast and southeast regions of the country. The difference between regions may be related to factors such as underreporting in some areas, causing errors in the sum of reported cases. It may also be related to lack of communication among health professionals. Professionals who do not communicate tend to infer that another professional has already made the notification, also causing evaluation errors in the number of cases (Baldan et al., 2017). And, since the public policies for drug prevention and distribution are based on this information, there seems to be a compromise in local health action (Magno et al., 2019).
According to Silva (2016), adults tend to use fewer condoms in sexual intercourse and this behavior possibly increases the risk of exposure and infection by the virus in the age range between 20 and 49 years, and can therefore increase the number of cases (figure 2). People with a sexually active sex life believe that they can not be affected by this disease, even if they have unprotected sex (Silva, 2016). In the elderly, aged between 50 and 64 years, the percentage of cases is increasing. Among the possible reasons is the lack of awareness about prevention and risk factors. This neglect can lead to behaviors that increase the chance of infection and, consequently, the number of cases (Viana et al., 2017).
The higher frequency of cases in the male gender (figure 3) possibly occurs due to risk behaviors. Among them is the low HIV testing, especially with regard to the target population of this epidemic, men who have sex with men. Therefore, this attitude may influence the failure to seek adequate treatment and, consequently, an increase in the number of cases in the male gender (Guimarães et al., 2017). Another risk behavior is the low number of fixed partners and the high practice of unprotected sex, which in the male population is present, and can thus stimulate the largest number of cases in this genus (Pereira et al., 2016). The frequency decreases in the years of the study, possibly due to the decentralization of the HIV-AIDS referral centers, increasing access to medication, support and improved logistics for health actions (Zambenedetti et al., 2016). The free distribution of antiretroviral drugs also appears to have contributed to this decline (Viana et al., 2017).
The highest percentage of cases of brown people (figure 4) is possibly due to the greater vulnerability of this group. Brown people historically have less access to health care and education, which is related to the decline in HIV prevention (Castro et al., 2018). The second highest percentage is white people probably because members of this group are more sexually active. The literature also cites that whites use fewer condoms in their sexual relations (Pinho, 2016).
The highest percentage of case frequency occurs in people with incomplete secondary education (figure 5). This data is possibly influenced by failures in the HIV / AIDS awareness and education process, whether in the school environment or in advertising campaigns. This group was supposed to be well informed (Amaral et al., 2017). The second highest percentage is in the population with incomplete 5th to 8th grade, probably because as schooling time is lower for 8 years, they have difficulty understanding the forms of prevention and adherence to treatment (Remor et al., 2017).
CONCLUSIONS
• If communication between health professionals is well coordinated, there may be more accurate reporting of cases. As the allocation of public resources for prevention and treatment depend on this notification, greater efficiency could lead to improvements in public health.
• Improving health education in public and private education and raising awareness about risk behaviors could reduce the number of new cases of HIV / AIDS.
• The decentralization of outpatient services and the increased use of rapid HIV / AIDS tests would help to broaden and ease access to the general population, which would impact on case reduction.
REFERENCES
AMARAL, R.S.; CARVALHO, S.T.R.F.; Flor de Maria Araújo Mendonça SILVA, F.M.A.M.; DIAS, R.S. Soropositividade para HIV/AIDS e características Sociocomportamentais em adolescentes e adultos jovens. Rev. Pesq. Saúde, 18(2): 108-113, 2017.
BALDAN, S.S; FERRAUDO, A.S; ANDRADE, M. Características clínico-epidemiológicas da coinfecção por tuberculose e HIV e sua relação com o Índice de Desenvolvimento Humano no estado do Mato Grosso do Sul, Brasil. Rev Pan-Amaz Saude ,8(3):59-67, 2017.
BRASIL. Ministério da Saúde. Boletim epidemiológico HIV/AIDS. 2017. Disponível em < http://www.aids.gov.br/pt-br/pub/2017/boletim-epidemiologico-hivaids-2017>. Acesso em 09/04/2019.
BRASIL. Ministério da Saúde. Departamento de Vigilância Prevenção e Controle das IST, do HIV/AIDS e das Hepatites Virais (DIAHV). Sintomas e fases da AIDS. 2019. Disponível em <http://www.aids.gov.br/pt-br/publico-geral/o-que-e-hiv/sintomas-e-fases-da-aids>. Acesso em 09/04/2019.
CASTRO, S.S.; SCATENA, L.M.; MIRANZI, A.; NETO, A.M.; CAMARGO, F.C.; NUNES, A.A. HIV/AIDS case definition criteria and association between sociodemographic and clinical aspects of the disease reported in the State of Minas Gerais from 2007 to 2016. Ver. Soc. Bras. Med. Trop. 51(4):427-435, 2018.
CDC. Centers for Disease Control and Prevention. How is HIV passed from one person to another. 2018. Disponível em <https://www.cdc.gov/hiv/basics/transmission.html>. Acesso em 09/04/2019.
GOGA, A.; SINGH, Y.; JACKSON, D.; MUKUNGUNUGWA, S.; WAFULA, R.; ELIYA, M.; How are countries in sub-Saharan African monitoring the impact of programmes to prevent vertical transmission of HIV? BMJ, p. 1-5, 2019.
IBGE. Instituto Brasileiro de Geografia e Estatística. Estimativas da População. 2017. Disponível em < https://www.ibge.gov.br/estatisticas-novoportal/sociais/populacao/9103-estimativas-de-populacao.html?edicao=16985&t=resultados>. Acesso em 10/04/2019.
MAGNO, E.S.; SARAIVA, M.G.G.;.MENEZES, C.H.A.B. Causas de óbito relacionadas ao HIV / AIDS em Instituição de referência, Amazonas, 2016. Braz. J. Hea. Rev., v. 2, n. 2, p. 787-799, 2019.
MENEZES, P.D.L.; ALVES, N.R.; DINIZ, J.A.; SOUZA, F.A.F.; CARVALHO, P.M.M.; LEITE, P.I.P. Grau de adesão à terapia tripla combinada antirretroviral em pacientes diagnosticados com HIV/AIDS no Serviço de Atendimento Especializado. Rev. Mult. Psic. V.13, N. 44, p. 811-827, 2019.
PEREIRA, T.G.; ARAÚJO, L.F.; NEGREIROS, F.; NETO, R.N.S.B. Análise do comportamento sexual de risco à infecção pelo hiv em adultos da população em geral. Psico. 47(4), 2016.
PINHO, M.D.G.; BERQUÓ, E.; LOPES, F.; OLIVEIRA, K.A.; LIMA, L.C.A.; PEREIRA, N. Juventudes, Raça e Vulnerabilidades. Associação Brasileira de Estudos Populacionais. 2016. Disponível em <http://www.abep.org.br/publicacoes/index.php/anais/article/view/1119>. Acesso em 10/04/2019.
REMOR, K.V.T.; OGLIARI, L.C.; SAKAE, T.M.; GALATO, D.G. Adherence to antiretrovirals in hiv patients in florianópolis urban área. Arq. Catarin Med., 46(2): 53-64, 2017.
SILVA, R.A.R.; SILVA, R.T.S.; NASCIMENTO, E.G.C.; GONÇALVES, O.P.; REIS, M.M.; SILVA, B.C.O. Perfil clínico-epidemiológico de adultos hiv-positivo atendidos em um hospital de Natal/RN. J. res.: fundam. care. online. 8(3), 2016.
UNAIDS. Joint United Nations Programme on HIV/AIDS. Ending AIDS: Progress towards the 90–90–90 targets. 2017. Disponível em <http://www.unaids.org/en/resources/documents/2017/20170720_Global_AIDS_update_2017 >. Acesso em 09/04/2019.
USA. Department of Health & Human Services and supported. Secretary’s Minority AIDS Initiative Fund (SMAIF). HIV Treatment Overview. 2019. Disponível em <https://www.hiv.gov/hiv-basics/staying-in-hiv-care/hiv-treatment/hiv-treatment-overview>. Acesso em 09/04/2019.
VIANA, P.A.S.; NOVAIS, C.T.; REIS, R.W.C.; FLOR, S.M.C.; ROSA, P.B. Aspectos epidemiológicos, clínicos e evolutivos da AIDS em idosos no norte do Ceará. SANARE, Sobral .V.16 n.02,p.31-36, 2017.
ZAMBENEDETTI, G.; SILVA, R.A.N.S. Descentralização da atenção em HIV-AIDS para a atenção básica: tensões e potencialidades. Physis. 26 (03), 2016
[1] Students of the Medicine Course of Macapá Campus, Federal University of Amapá (UNIFAP).
[2] Students of the Medicine Course of Macapá Campus, Federal University of Amapá (UNIFAP).
[3] Students of the Medicine Course of Macapá Campus, Federal University of Amapá (UNIFAP).
[4] Biomedical, PhD in Topical Diseases, Professor and researcher of the Medicine Course of Macapá Campus, Federal University of Amapá (UNIFAP).
[5] Doctor, preceptor and researcher of the Macapá Campus Medicine Course, Federal University of Amapá (UNIFAP).
[6] Biologist, Doctor of Topical Diseases, Professor and researcher of the Physical Education Course, Federal University of Pará (UFPA).
[7] Theologian, PhD in Psychoanalysis, researcher at the Center for Research and Advanced Studies – CEPA.
[8] Biologist, PhD in Theory and Behavior Research, Professor and researcher of the Chemistry Degree Course at the Basic, Technical and Technological Federal Institute of Amapá (IFAP).
Posted: May, 2019
Approved: May, 2019















