INTEGRATIVE REVIEW
SONG, Berty Ru Ping [1], MANFREDI, Paula [2], SOUZA, Isabel Fernandes de [3]
SONG, Berty Ru Ping. MANFREDI, Paula. SOUZA, Isabel Fernandes de. Nutritional status of children and adolescents with Down Syndrome: Integrative review. Revista Científica Multidisciplinar Núcleo do Conhecimento. Year 05, Ed. 11, Vol. 19, pp. 55-70. November 2020. ISSN: 2448-0959, Access link: https://www.nucleodoconhecimento.com.br/nutrition/nutritional-status
SUMMARY
Introduction: Obesity is a chronic disease defined as abnormal or excessive accumulation of body fat due to positive energy balance. However, the epidemic is little studied in people with Down Syndrome (DS). The population with DS is more susceptible to developing overweight and obesity, reaching one third to half of the population. Objective: To evidence the prevalence of overweight and obesity in children and adolescents with Down Syndrome in a decade (2009-2019). Methodology and results: The articles were searched from August 3 to 28, 2020, consulting the PubMed, Scielo and LILACS databases. Of the 473 documents recovered, 13 studies were included in the review. Final Considerations: Based on the data collected in this study, it was possible to identify an alarming prevalence of overweight and obesity in children and adolescents with DS. This condition affects individuals with healthy DS and comorbidities, of both sexes regardless of age and degree of disability.
Keywords: Down syndrome, obesity, nutritional status.
1. INTRODUCTION
Obesity is a chronic disease that, according to the World Health Organization, can be defined as abnormal or excessive accumulation of body fat due to positive energy balance (WHO, 1998). It can be classified based on body mass index (BMI), body fat percentage (%BF), waist-hip ratio and electrical bioimpedance (BIA) (WRIGHT et al., 2008).
In recent decades, this situation has been increasing alarmingly, compromising the health and well-being of individuals and, for this reason, obesity has become one of the major public health concerns1. However, the epidemic is poorly studied in specific populations, such as people with Down Syndrome (THEODORO; BLASCOVI-ASSIS, 2009).
Down Syndrome (DS) is a genetic condition in which individuals have an extra chromosome on par 21, so it is also known as trisomy 21. It is considered the most frequent abnormality in humans affecting 1 in 700-1000 births (CHAVE; CAMPOS; NAVARRO, 2012).
Studies indicate that children with DS are more susceptible to developing overweight and obesity, reaching one third to half of the population. This condition may lead to other concomitant health problems such as cardiovascular diseases, dyslipidemia, systemic arterial hypertension (SAH), obstructive sleep apnea syndrome (ASAS), among others. In addition, overweight and obese children have an increased risk of becoming obese adults (VAN GAMEREN-OOSTEROM et al., 2012; LORÍA; URRUTIA, 2009; RIMMER et al., 2009).
Children with DS have inherent physical and physiological characteristics such as muscle hypotonia, congenital heart disease, hypothyroidism, auditory and visual dysfunctions, decreased basal metabolic rate, and gastrointestinal changes; in addition to the developmental delay and intellectual disability that limits the practice of physical activities. This set of complications that directly and/or indirectly affect nutritional aspects, added to inadequate eating habits favors weight gain (MOURA et al., 2009; MOREIRA; EL-HANI; GUSMÃO, 2000; BULL, 2011).
Thus, the present project aimed to evidence the prevalence of overweight and obesity in children and adolescents with Down Syndrome in a decade (2009-2019), based on an integrative review of the selected studies.
2. MATERIALS AND METHODS
This is an integrative review of the literature, which is one of the broader methodologies, which consists of conducting a bibliographic survey collecting data from secondary sources, in order to synthesize the knowledge about the same topic (SOUZA; SILVA; CARVALHO, 2010)). Initially, the research theme and the guide question were defined: “What evidences are present in the theoretical framework, of a decade (2009-2019), regarding the prevalence of overweight and obesity in children and adolescents with Down syndrome?” and therefore the descriptors. The hypothesis is that 10% are obese and 30% are overweight.
For the survey of the bibliographic material, the articles were searched from August 3 to 28, 2020, consulting the PubMed, Scielo and Latin American and Caribbean Literature in Health Sciences (LILACS) databases. The following descriptors and their combinations were used in Portuguese and English: “Síndrome de Down”, “Obesidade” and “Estado Nutricional” (“Down Syndrome”, “Obesity” and “Nutritional Status”).
The inclusion criteria for the selection of materials were: studies that contemplate the problem, i.e., overweight and obesity in children and adolescents with DS; published in Portuguese, English and Spanish; publications available in full and free of charge that portrayed the theme addressed and published and indexed in databases between 2009 and 2019. Duplicate articles that presented research outside the scope of the search or treated Down syndrome in adults and the elderly in physical education and psychology were excluded.
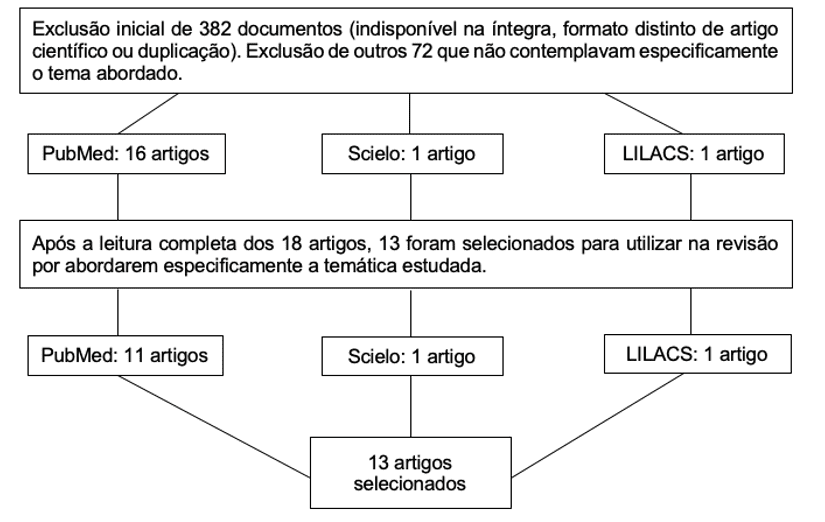
The search of the databases resulted in 473 documents. From the reading of the titles, it was possible to exclude 382 articles that were outside the scope of the search, without access to the material in full and duplicated. Soon, a summary of the remaining articles was read (n = 91). This reading allowed the exclusion of 73 other articles that did not specifically address the theme addressed (Table 1).
Table 1. Articles deleted after reading abstracts
| Article area or theme | Discarded | Article area or theme | Discarded |
| Genetic | 4 | Nutrition (other aspects) | 7 |
| Cancer | 1 | General deficiencies | 9 |
| Hormones | 7 | Autism Spectrum Disorder | 2 |
| Physical Education | 11 | Medicine | 3 |
| Recommendations | 10 | Other subjects | 13 |
| Family | 6 | Total discarded: | 73 |
Source: Berty Ru Ping Song
After the complete reading of the remaining 18 articles, 13 articles were integrated into the review (Figure 1).
Figure 1. Flowchart of the selection process of the articles searched
Source: Berty Ru Ping Song
The evaluations for the selection of articles were made by a single researcher. Of the 13 studies that were included in the review, twelve (12) were based on the descriptors “Down Syndrome” and “obesity” and one (1) in “Down Syndrome” and “nutritional status” as shown in Chart 1.
Table One. Search results
| Terms | Down Syndrome and obesity | Down Syndrome and Pediatric Obesity | Down andnutritional status |
| Database | |||
| PubMed | Found: 214
Excluded: 204 Total: 10 |
Found: 52
Excluded: 52 Total: 0 |
Found: 47
Excluded: 46 Total: 1 |
| Scielo | Found: 41
Excluded: 40 Total: 1 |
Found: 2
Excluded: 2 Total: 0 |
Found: 29
Excluded: 29 Total: 0 |
| LILACS | Found: 63
Excluded: 62 Total: 1 |
Found: 3
Excluded: 3 Total: 0 |
Found: 22
Excluded: 22 Total: 0 |
Source: Berty Ru Ping Song
3. RESULTS
The sample size ranged from 16 to 1,596 participants, totaling 3,231 of the 13 studies included in this review.
In relation to the countries of origin, two were conducted in Brazil, two in Ireland, two in the United States, two in Chile, two in Spain, one in the Netherlands, one in New Zealand and finally one in Costa Rica. The number of authors ranged from 2 to 12.
The articles were organized with their authorship/year, sample/type of study, methodology, objectives and conclusions, according to Chart 2.
Table two. Characterization of studies regarding authorship/year, sample/type of study, methodology, objectives and conclusions
| Authorship/ Year | Sample/Type of Study | Methodology | Study Objectives/Focus | Conclusions/Main results |
| Pierce M.; Ramsey, K.; Pinter, J.
(2019) |
(n=412) | Obesity and overweight rates by age group were calculated and possible associations with common comorbidities were examined from the databases. The mean percentile of body mass index (BMI) and the change in bmi percentile by age were also examined. | Evaluate trends in obesity and overweight in children with DS from Oregon. | A total of 23% were overweight and 20.6% were obese. The BMI percentile increased with female gender, age and height percentile for age. |
| Amo-Setién; et al.
(2019) |
Cross-sectional study
(n=220) |
The body mass index was used to determine nutritional status, classified into four categories according to the criteria of the International Obesity Task Force (IOTF): low weight; normal weight; overweight; Obesity. | Determine the prevalence and factors associated with overweight and obesity among students from special education schools. | The prevalence of overweight/obesity was 40.9%. Obesity was more frequent in females (26.0%) than in males (9.8%). |
| O’ Shea; et al.
(2018) |
Cross-sectional study
(n=61) |
Height and weight of 61 participants aged between 4 and 16 years were measured. Body mass index (BMI) was calculated and body fat percentage (%BF) was measured using the electrical bioimpedance analysis (BIA). | To determine the prevalence of overweight and obesity among children and young people with DS. | Based on the calculations, 51.6% of men and 40% of women were overweight/obese compared to 32% and 14.8%, respectively, using %BF. |
| De la Piedra, M. J.; et al.
(2017) |
Retrospective study
(n=218) |
The lipid profile of the sample was evaluated, obtained through laboratory tests. Other conditions were obtained from the medical records. The diagnosis of dyslipidemia was considered according to the criteria of the National Institute of Heart, Lungs and Blood of the USA 2011. | Describe the frequency of dyslipidemia in a population of Chilean children and adolescents with DS. | After reviewing the medical records, 58.3% had some type of dyslipidemia. |
| Bertapelli, F; et al.
(2016) |
Literature review
(n=45) |
A search was performed using databases. From a total of 4,280 studies, we included 45 original research papers published between 1988 and 2015. | Review the prevalence of overweight and obesity and its determinants in young people with DS. | The combined prevalence of overweight and obesity ranged from 23% to 70% studies. |
| Basil, J. S.; et al.
(2016) |
Retrospective review
(n=303) |
A total of 303 children aged 2 to 18 years diagnosed with DS were evaluated. | Evaluate whether children with DS in the United States are at increased risk of obesity. | Of the 303 individuals evaluated, 47.8% were obese, significantly higher than the general pediatric population, which had an obesity rate of 12.1% |
| Hoey, E.; et al.
(2016) |
(n=131) | Data were collected through questionnaires; 4-day food survey and measurements of weight, height and waist circumference. | Examine the nutritional intake and anthropometric status of individuals with intellectual disabilities. | The mean BMI of the participants was 29.4 kg/m2 +/- 6.1, where 28.2% were overweight and 46.8% were obese. |
| Jiménez, L.; et al.
(2015) |
Cross-sectional, descriptive study
(n=79) |
The weight was collected height and also calculated their BMI. Nutritional diagnosis was given from BMI. | Determine overweight and obesity rates in students with DS. | Overweight and obesity rates according to SDM/2002, NCHS/2000 and WHO/2007 were 43, 57 and 66% respectively. |
| Bertapelli, F.; et al.
(2013) |
(n=41) | Nine anthropometric measurements were performed, the determination of %BF and statistical treatment. | To evaluate the prevalence of obesity and topography of body fat in children and adolescents of both sexes with DS. | Most individuals had excess body fat, and these were superior in females. It was also verified higher concentration of fat in the thigh and lower deposit in the biceps region. |
| Van Gameren-Oosterom, H.B. M.; et al.
(2012) |
(n=1596) | Longitudinal growth data were collected from Dutch children with DS who were born after 1982. | To evaluate the prevalence rates of overweight and obesity in a national sample of Dutch children with DS. | The evaluation showed that 25.5% of boys and 32.0% of girls were overweight, while 4.2% of boys and 5.1% of girls were obese. |
| Loveday, S. J.; Thompson, J.; Mitchell, E. A.
(2012) |
(n=77) | Anthropometric data, electrical bioimpedance analysis (BIA) and dual energy X-ray absorptiometry (DXA) were collected from seventy children with DS to calculate %BF. | Accurately measure body fat in children with DS. | The mean %BF was 30.5% for girls and 22.5% for boys. A total of 38% of girls and 23% of boys were obese according to international criteria. |
| Marín, A. S.; Graupera, J. M. X.
(2011) |
(n=39) | Body composition, physical activity level, nutrient intake, validated questionnaires and biochemical parameters were estimated from 38 people with DS. | Assess nutritional status in young adults with DS. | When classifying BMI, 36.8% were overweight (BMI: 25-29.9 kg/m2) and 36.8% were obese (BMI ≥ 30 kg/m2). |
| Loría, A. M.; Urrutia, A. R. G.
(2009) |
(n=16) | Anthropometric, biochemical and clinical indicators were evaluated. Eating habits, lifestyle and socioeconomic aspects were also considered. | To evaluate the nutritional status of children with DS from 7 to 14 years of age. | Most of them showed signs of obesity. Of the sample evaluated, 80% of the participants had hypertriglyceridemia and 73.33% had low HDL cholesterol levels. In addition, a low level of physical activity has been reported. |
4. DISCUSSION
4.1 PREVALENCE OF OVERWEIGHT AND OBESITY
Down syndrome is significantly associated with higher rates of overweight and obesity, with an average of 26.70% and 32.98%, respectively, in children and adolescents of both sexes. The nutritional status of this population can be determined from BMI, %BF and BIA (WRIGHT et al., 2008).
When compared to the general pediatric population, there is a rate of approximately twice as high as overweight and obesity in the population with DS (DE LA PIEDRA et al., 2017; BERTAPELLI et al., 2013). This clinical picture facilitates the development of other health problems, such as cardiovascular diseases, dyslipidemias, ASAS, compromising the quality of life of individuals (LORÍA; URRUTIA, 2009; RIMMER et al., 2009).
One study evaluated malnutrition due to overweight in 79 students with DS using three distinct BMI standards for age: SDM/2002, NCHS/2000 and WHO/2007. The obesity rates found were 21.5%, 34.2% and 37.9% for SDM/2002, NCHS/2000 and WHO/2007 standards, respectively. In addition, it was also observed that 60.8% of the students evaluated had inadequate nutrition, which is an important factor to explain overweight (JIMÉNEZ et al., 2015).
Although the critical period for the development of overweight and obesity during childhood and adolescence is not yet defined, it is possible to observe the increase in rates of such conditions from 2 years of age (BERTAPELLI et al., 2016).
4.2 FOOD INTAKE AND PHYSICAL ACTIVITY
A diet is considered healthy when there is a balance between all the necessary nutrients, from macronutrients (carbohydrates, lipids and proteins) to micronutrients (vitamins and minerals). Adequate nutrition is essential for the proper functioning of the body and for healthy growth and development, in addition to preventing overweight and other associated comorbidities. Thus, it is fundamental in improving quality of life both for the general population and also for the population with DS (VALLE, 2007).
Individuals with DS presented unbalanced dietary habits, with energy, fiber, calcium, vitamin D, folate and vitamin E consumption below the recommended level. Unlike sugars, lipids and saturated fats, there is an intake above the recommended amount by this population (HOEY et al., 2016; MARÍN; GRAUPERA, 2011).
The most consumed foods are pasta, bread with jam or bologna or butter, milk, industrialized juice, mixed fruits, cookies, desserts, soft drinks, flours and tubers. It is observed that the consumption of meat, fresh fruits, vegetables and vegetables is low which means a low consumption of fibers, phytochemicals, vitamins and minerals (LORIA; URRUTIA, 2009).
In addition, the levels of physical activity for such a group can be considered sedentary, it is not common for children and adolescents to exercise in addition to everyday tasks (walking, running around the house, playing, dancing) (BERTAPELLI et al., 2013; LORIA; URRUTIA, 2009).
The main factor for maintaining a eutrophic nutritional status is adequate nutrition added to at least mild or moderate physical activity. When neither is carried out, the risks of developing overweight and obesity are increased and synchronously the risks of other pathologies as well (HOEY et al., 2016; LORIA; URRUTIA, 2009; VALLE, 2007).
4.3 MEDIDAS ANTROPOMÉTRICAS
According to the BMI classification, values between 25 and 29.9 kg / m² point to overweight and from 30 kg / m² to obesity (HOEY, 2017). % GC can be obtained from skin folds or BIA (BERTAPELLI et al., 2013; LOVEDAY; THOMPSON; MITCHELL, 2012). The most used skin folds are tricipital (DCT), bicipital (DCB), subscapular (DCSE), supra-iliac (DCSI), abdominal (DCAB), thigh (CX) and leg (PE). The sum of 7 folds (∑ folds) is also used (BERTAPELLI et al., 2013).
While high BMI and %BF increase the risk of obesity, waist circumference determines the risk for metabolic complications (HOEY, 2017; MARÍN; GRAUPERA, 2011).
To determine the prevalence of overweight and obesity, 61 individuals between 4 and 16 years of age participated in a study in which their heights and weights were collected for bmi calculation and body composition using BIA. The BMI classification showed that 35.5% of boys and 30.0% of girls were overweight and 16.1% of boys and 10.0% of girls were obese. The results of the %BF showed that 20.0% of boys and 11.1% of girls were overweight and 12.0% of boys and 3.70% of girls were obese (O’SHEA et al., 2018).
In 2016, Hoey et al. found that the mean male BMI was 28.8 kg/m² and the female bmi was 30.2 kg/m². Categorizing them, it was observed that 2.4% of the sample (n=131) were underweight, 22.6% eutrophic, 28.2% overweight and finally 46.8% obese (HOEY et al., 2016).
Thus, it is presumed that anthropometric measurements are good parameters to evidence the prevalence of overweight and obesity in the population with DS (PIERCE; RAMSEY; PINTER, 2019; HOEY et al., 2016).
4.4 COMORBITIES
Excess body fat is associated with several comorbidities, such as cardiovascular disease, dyslipidemia, OSAS, diabetes, among others (DE LA PIEDRA et al., 2017). Therefore, the population with DS requires extra care due to clinical conditions (DE LA PIEDRA et al., 2017; BERTAPELLI et al., 2013). Some have other pathologies such as hypothyroidism, which influences even more the rates of overweight and obesity (VAN GAMEREN-OOSTEROM et al., 2012).
The amount of body fat is proportional to the levels of total cholesterol, LDL and triglycerides and inversely proportional to HDL levels. It is quite common to note that children and adolescents with DS have HDL below the reference values and simultaneously high levels of triglycerides (DE LA PIEDRA et al., 2017).
ASAS is airway obstruction during sleep, either completely or incompletely. Already aware of the predisposition of the population with DS for obesity, it is important to highlight that this is one of the greatest risk factors for ASAS (PIERCE; RAMSEY; PINTER, 2019; BASIL et al., 2016).
In a study with 303 patients, it was observed that 74.0% had some obstruction, with the majority (38.9%) in a lighter way. However, when it comes to obesity, the risk increases for moderate and severe obstructions (BASIL et al., 2016).
Therefore, it is concluded that the overweight picture increases the risk of developing other clinical manifestations and together may compromise the health and quality of life of children and adolescents with DS.
4.5 GENDER AND AGE
It is known that both sexes are susceptible to overweight, which is the determining factor for the risk of obesity, however, the female group presented higher rates for this (AMO-SETIÉN et al., 2019; MARÍN; GRAUPERA, 2011). The prevalence of obesity ranged from 67.0% and 88.0% for the age groups from 6 to 12 years and 13 to 19 years, and can be justified by the transition from childhood to adolescence (BERTAPELLI et al., 2013).
Although overweight and obesity rates were considered constant until adolescence, a study with 77 families observed that in males there was a higher value of %BF before 12 years of age. Meanwhile, females showed higher values of %BF after 12 years (LOVEDAY; THOMPSON; MITCHELL, 2012).
In view of this, more research is needed to define whether there is in fact a relationship between overweight and obesity and age in children and adolescents with DS (VAN GAMEREN-OOSTEROM et al., 2012; LOVEDAY; THOMPSON; MITCHELL, 2012).
5. FINAL CONSIDERATIONS
Based on the data collected in this study, it was possible to identify a high prevalence of overweight and obesity in children and adolescents with DS. This condition affects individuals with healthy DS and comorbidities, of both sexes regardless of age and degree of disability.
The main factor for this tendency of excessive weight gain was inconclusive, because the combinations of metabolic alterations are distinct and individual. Some likely determinants are decreased basal metabolic rate, low physical activity levels, and unfavorable dietary patterns. Early monitoring decreases the risk of developing future medical implications.
The predisposition to weight gain and the associated health risks, combined with the vulnerability of this population, require effective interventions in order to prevent worsening of physical and physiological conditions. Thus, the inclusion of healthy dietary patterns reconciled the practice of physical activity is essential for the health and for a higher quality of life of this population.
With everything, obesity is a risk factor for several other comorbidities that is accentuated in individuals with DS and can be observed from early childhood. Intervention plans are essential to improve nutritional status and restore quality of life.
6. REFERENCES
AMO-SETIÉN, F.; ABAJAS-BUSTILLO, R.; SARABIA-COBO; PARÁS-BRAVO, P.; LEAL COSTA, C., REDONDO-FIGUERO, C., BANDINI, L. (2019). Prevalence and factors associated with overweight and obesity among Spanish students attending special education schools. Journal of Applied Research in Intellectual Disabilities. 33. doi: 10.1111/jar.12679.
BASIL, JS; SANTORO, SL; MARTIN, LJ; HEALY, KW; CHINI, BA; SAAL, HM. Retrospective Study of Obesity in Children with Down Syndrome. J Pediatr. 2016 Jun;173:143-8. doi: 10.1016/j.jpeds.2016.02.046. Epub 2016 Mar 14. PMID: 26987801.
BERTAPELLI, F; PITETTI, K; AGIOVLASITIS, S; GUERRA-JUNIOR, G. Overweight and obesity in children and adolescents with Down syndrome-prevalence, determinants, consequences, and interventions: A literature review. Res Dev Disabil. 2016 Oct;57:181-92. doi: 10.1016/j.ridd.2016.06.018. Epub 2016 Jul 19. PMID: 27448331.
BERTAPELLI, Fabio et al . Prevalence of obesity and the body fat topography in children and teenagers with down syndrome. Rev. bras. crescimento desenvolv. hum., São Paulo , v. 23, n. 1, p. 65-70, 2013.
BULL, MJ; Committee on Genetics. Health supervision for children with Down syndrome. Pediatrics. 2011 Aug;128(2):393-406. doi: 10.1542/peds.2011-1605. Epub 2011 Jul 25. Erratum in: Pediatrics. 2011 Dec;128(6):1212. PMID: 21788214.
CHAVES, Aclesia Lima; CAMPOS, Cíntia Kátia; NAVARRO, Antonio Coppi. Relação da síndrome de down com a obesidade. RBONE-Revista Brasileira de Obesidade, Nutrição e Emagrecimento, v. 2, n. 11, 2012.
HOEY, E; STAINES, A; WALSH, D; CORBY, D; BOWERS, K; BELTON, S; MEEGAN, S; MCVEIGH, T; MCKEON, M; TRÉPEL, D; GRIFFIN, P; SWEENEY, MR. An examination of the nutritional intake and anthropometric status of individuals with intellectual disabilities: Results from the SOPHIE study. J Intellect Disabil. 2017 Dec;21(4):346-365. doi: 10.1177/1744629516657946. Epub 2017 Feb 7. PMID: 27402617.
JIMENEZ, Lily et al . Malnutrición por exceso: alta frecuencia de sobrepeso y obesidad en escolares chilenos con síndrome de Down. Rev. méd. Chile, Santiago, v. 143, n. 4, p. 451-458, abr. 2015.
LOVEDAY, SJ; THOMPSON, JM; MITCHELL, EA. Bioelectrical impedance for measuring percentage body fat in young persons with Down syndrome: validation with dual-energy absorptiometry. Acta Paediatr. 2012 Nov;101(11):e491-5. doi: 10.1111/j.1651-2227.2012.02821.x. Epub 2012 Sep 5. PMID: 22897200.
MADRIGAL LORIA, Alejandra; GONZALEZ URRUTIA, Ana Rocío. Estado nutricional de niños con Síndrome Down del Centro Nacional de Educación Especial de Costa Rica. Rev. costarric. salud pública, San José , v. 18, n. 2, p. 72-78, Dec. 2009.
MOREIRA, Lília MA; EL-HANI, Charbel N; GUSMAO, Fábio AF. A síndrome de Down e sua patogênese: considerações sobre o determinismo genético. Rev. Bras. Psiquiatr., São Paulo , v. 22, n. 2, p. 96-99, June 2000.
MOURA, A. B.; MENDES, A.; PERI, A.; PASSONI, C. R. M. S. Aspectos nutricionais em portadores da Síndrome de Down. Cadernos da escola de saúde, Curitiba, p.1-11, 2009.
O’ SHEA, M; O’ SHEA, C; GIBSON, L; LEO, J; CARTY, C. The prevalence of obesity in children and young people with Down syndrome. J Appl Res Intellect Disabil. 2018 Nov;31(6):1225-1229. doi: 10.1111/jar.12465. Epub 2018 May 15. PMID: 29761882.
PIEDRA, MJ DE LA,; ALBERTI G, CERDA J, CÁRDENAS A, PAUL MA, LIZAMA M. Alta frecuencia de dislipidemias en niños y adolescentes con Síndrome de Down. Rev. chil. pediatr. Santiago, v. 88, n. 5, p. 595-601, 2017 .
PIERCE, M; RAMSEY, K; PINTER, J. Trends in Obesity and Overweight in Oregon Children With Down Syndrome. Glob Pediatr Health. 2019 Apr 2;6:2333794X19835640. doi: 10.1177/2333794X19835640. PMID: 31044152; PMCID: PMC6446252.
RIMMER, JH; YAMAKI, K; LOWRY, BM; WANG, E; VOGEL, LC. Obesity and obesity-related secondary conditions in adolescents with intellectual/developmental disabilities. J Intellect Disabil Res. 2010 Sep;54(9):787-94. doi: 10.1111/j.1365-2788.2010.01305.x. Epub 2010 Jul 12. PMID: 20630017.
SOLER MARIN, A.; XANDRI GRAUPERA, J. Mª. Nutritional status of intellectual disabled persons with Down syndrome. Nutr. Hosp., Madrid , v. 26, n. 5, p. 1059-1066, oct. 2011 .
SOUZA, Marcela Tavares de; SILVA, Michelly Dias da; CARVALHO, Rachel de. Revisão integrativa: o que é e como fazer. Einstein (São Paulo), São Paulo , v. 8, n. 1, p. 102-106, Mar. 2010 .
THEODORO, Luciana Rodrigues; BLASCOVI-ASSIS, Silvana Maria. Síndrome de Down: associação de fatores clínicos e alimentares em adolescentes com sobrepeso e obesidade. Psicol. teor. prat., São Paulo , v. 11, n.1, p. 189-194, jun. 2009.
VALLE, Janaína Mello Nasser. A formação dos hábitos alimentares na infância: uma revisão de alguns aspectos abordados na literatura nos últimos dez anos. Aps, Juiz de Fora, v. 1, n. 10, p.56-65, jun. 2007.
VAN Gameren-Oosterom, HB; van Dommelen, P; Schönbeck, Y; Oudesluys-Murphy, AM; van Wouwe, JP; Buitendijk, SE. Prevalence of overweight in Dutch children with Down syndrome. Pediatrics. 2012 Dec; 130(6):e1520-6. doi: 10.1542/peds.2012-0886. Epub 2012 Nov 12. PMID: 23147968.
WORLD HEALTH ORGANIZATION. Obesity: preventing and managing the global epidemic. Report of a WHO consultation on obesity in Geneva, 3-5, jun. 1997. Geneva: WHO, 1998.
WRIGHT, C.; SHERRIFF, A.; WARD, S. et al. Development of bioelectrical impedance-derived indices of fat and fat-free mass for assessment of nutritional status in childhood. Eur J Clin Nutr. 62, 210–217 (2008). https://doi.org/10.1038/sj.ejcn.1602714
[1] Undergraduate student in Nutrition at the Centro Universitário União das Américas. Trainee at the Specialized Rehabilitation Center IV (CER IV)
[2] Guidance counselor. Degree in nutrition. Master in Human Aging from the University of Passo Fundo. Professor at the University Center Union of the Americas – Foz do Iguaçu.
[3] PhD in production engineering sciences. Professor of the Physiotherapy Course. Advisor in Scientific Initiation. Union of the Americas University Center.
Submitted: November, 2020.
Approved: November, 2020.