OLIVEIRA , Gleslei Moraes de [1], SILVA, Rômulo Terminelis da [2]
OLIVEIRA, Gleslei Moraes de; SILVA, Rômulo Terminelis da – Inclusion and literacy of children with ADHD a challenge Multidisciplinary Core Scientific knowledge magazine, year 1, vol. 7, p. 91-108. August 2016. ISSN:0959-2448
SUMMARY
This article discusses the attention deficit hyperactivity disorder (ADHD). ADHD is one of the main concerns in children at school age. The research investigated the child’s ADHD learning during literacy in third grade in school Hall Hafizabad in Flush-Minas Gerais, Brazil. Aiming to clarify about ADHD for education professionals, families and related areas, in order to alleviate the anguish of the students and the aspects that hinder their learning. Interest of training teachers to work with children with ADHD and the participation of humanizing and service monitoring programs for families. Was bibliographical and field, with a quantitative and qualitative approach, the level of descriptive research, correlational and not experimental. The instruments used were questionnaires and observation, having as subject of research students from year 3 ADHD. This study enables discussions and analysis on the teaching practice by the child of the disorder, creating opportunities for reflection and action to resolve difficulties at the stage of literacy for a teaching learning process effective.
Keywords: attention deficit hyperactivity disorder. Difficulties. Interventions. Inclusion. Literacy
1. INTRODUCTION
This article is based on research about the inclusion and literacy of children with ADHD. Aiming to clarify about the disorder to education professionals, families and related areas, in order to alleviate the anguish of students diagnosed with the disorder and the aspects that hinder their learning.
The theme is justified by the fact of this disorder is one of the main concerns presented in school-aged children, especially in the period of literacy.
In this context, considering the impact of the characteristics of ADHD on children’s literacy and learning, this research has a quantitative and qualitative approach, the level is correlational, and descriptive.
This study seeks to provide the overcoming difficulties and development sociocognitivas skills of children with ADHD. Research is experimental, not studying the phenomenon in the natural context in which it occurs, to analyze it, describe it and examine it.
The field research was held at Escola Municipal Conselheiro Lafaiete, Glary – MG/Brazil. The school offers early childhood education first and second periods and primary education from 1st to 5th year in morning and afternoon shifts.
We conducted a survey of students with ADHD in the third grade. The data were collected in order to achieve the objectives proposed making the results more visible and allowing the evidence of the difficulties and possible solutions in the school context, in order to observe the inclusion of students, review the teacher’s action and evaluate the intervention of the teacher in the classroom. Was addressed the importance of clarification to the parents and training programs to professionals of education about the disorder to the identification of learning disabilities, care and follow-up of students and families.
The processing of data was run through bibliographical research, corroborating the data collected and linked to research, analyzed with grounded on relevant theory, gathering information to answer the goals and solution to the problem investigated.
This research is: relevant because it is a problem that affects children of all ages and social classes; It is pertinent for contributing to education and society in the awareness of the existence of ADHD; feasible, because the school offers conditions for the execution of activities directed to students carry the disorder.
Based on studies conducted on the theme of Inclusion and literacy for children with ADHD: a challenge. There are precedents that mention investigations about ADHD. However, in the School field, there’s no history of investigated specific studies as developed in this work.
This study sought to support theoretical us Barkley, Mattos, Rohde, and Vygotsky, among others whose legacies can substantiate this investigation. A questionnaire was applied to ten school teachers on the difficulties encountered in the inclusion and literacy of students with ADHD. As realization are perceptible changes in learning and change in the behavior of children with ADHD through educational procedures, having as tools the psychological and clinical referrals, enabling new possibilities for the construction of knowledge, recognizing the differences and peculiarities in contributing to the effectiveness of learning of students with ADHD.
2. CONCEPTS AND CHARACTERISTICS OF ADHD
2.1 CONCEPT OF ADHD
The attention deficit hyperactivity disorder (ADHD), sometimes called ADD (attention deficit disorder) or SDA (attention deficit syndrome). It is known in English as ADD, ADHD (Attention Deficit/Hyperactivity) Disorder (ADHD) or AD/HD. In the years 60 was defined as a syndrome of conduct.
“Virginia Douglas, a Canadian researcher, in the Decade of 70 began dedicating a comprehensive look at the symptoms associated with ADD (attention deficit disorder) and thanks to his studies from the early 80 this syndrome was renamed with the name of ADHD (attention deficit disorder with Hyperactivity) arousing the interest of many researchers on the subject” (HALLOWEL and RATEY , 1998, p. 27). In the Decade of 80, went on to emphasize cognitive of the syndrome definition especially attention deficit and impulsivity or lack of control.
For Rohde and Benczik (1999, p. 12) ADHD is a mental health problem that is characterized by inattention, restlessness or hyperactivity and impulsivity. Claim they can lead to emotional difficulties, family, school and social.
ADHD is recognized by the who (World Health Organization), and in many countries, law of protection, assistance and help both ADHD patients but also their families.
Goldstein (1998, p. 35), sets the ADHD biopsychosocial Disorder characterized by inattention, hyperactivity and impulsivity, caused by genetic factors, biological, social and existential. Interferes with the ability to maintain attention, his emotions and the activity level, to face consequences and, in the ability to control and inhibition.
According to Barkley (2002, p. 35), (…) A development disorder of self-control that consists of problems with periods of attention, impulse control and the level of activity. (…) These problems are reflected in damage in the will of the child or in their ability to control their own behavior on the passage of time – keep in mind future objectives and consequences. It is not just (…) a question of being inattentive or hyperactive.
According to the DSM-5, the ADHD ranks among the neurodevelopment disorders, which are characterized by difficulties in developing that manifest themselves early and influence the functioning personal, social, academic or personal.
Studies using clinical methodologies agree that ADHD appears to be a disease of multifactorial origin, with genetic and environmental components, where probably several anomalous genes of small effect in combination with a hostile environment, formatariam a brain changes in its chemical structure and anatomical. The brain circuits involved are those related to the control of attention and impulses-fronto-estriatais, limbic and cerebellar and neurochemical structures are the dopaminergic and noradrenergic systems (BARKLEY, 2002).
2.2 CHARACTERISTICS OF ADHD
ADHD is characterized by distinct symptoms that can manifest themselves together or separately in early childhood.
According to ICD-10 (International statistical classification of diseases and Related Health Problems) the main features of ADHD (F00-F99 chapter V: classification of mental and behavioural disorders. USP, 1988, p. 59) are: the lack of persistence in activities involving cognitive, tendency to switch from one activity to another without completing any, along with an excessive activity, disorganized and poorly controlled. These problems usually persist through the school years and even into adulthood, but many affected individuals show a gradual improvement in the activity and attention.
According to Rohde and Benczik (1999, p. 20) the causes of ADHD, namely, ineffective functioning of neurotransmitters can be caused by: heredity when a child inherits a predisposition to the disorder in addition to environmental influences; problems in pregnancy and childbirth and family problems, which can worsen the picture of ADHD more than its cause.
Paulo Mattos (2003, p. 71) States that clinical experience has shown that in some children with ADHD symptoms appear after seven years, causing so many difficulties with regard to children who started having them before that age. The causes of ADHD can be several as: emotional conflicts and or family relationships and other mental health problems. Numerous are the emotional problems that can lead to inattention, hyperactivity or impulsivity.
According to Ratey w Hallowel (1988, p. 7), with respect to the characteristic symptoms are: inattention difficulty paying attention or Miss by mistake; of organization; be distracted, forget and lose things easily; don’t follow instructions and not finish tasks that require constant mental effort. In the case of hyperactivity, the features are: shake hands or feet; rummage and lift the Chair; run too much; difficulty playing quietly; talk too. Symptoms of impulsiveness are: difficulty in wait time; hasty answers before questions have been completed; stop or to interfere in the Affairs of others.
These authors (1998, p. 45), allege that work in an integrated manner parents, teachers and health professionals is of fundamental importance for the correct diagnosis of ADHD.
As Open Topczewski (1999, p. 02), there are two approaches for treating ADHD, psychological and biological, where explains: Medicine corrects the behavior, the individual restructuring requires another approach. The medicine Act so acute in hyperactivity and need long-term psychological treatment, the result will be delayed, and during this period the individual is still inadequate, showing the same problems from the beginning. The medicine can improve the behavioral part, but the psychological treatment is necessary and even mandatory in such cases.
Second Hallowel and Ratey (1999, p. 66), “The most commonly used medications for the control of symptoms of ADHD are Psychostimulants, 70% to 80% of children and adults with ADHD exhibit a positive response”. In the case of the specific problem of children with ADHD medications present a significant improvement with reduction of impulsive and hyperactive behavior and increased attention span.
Rohde and Benczik (1999, p. 66) corroborate the statement of the authors mentioned above, “several careful studies have clearly shown that more than 70% of children and adolescents with ADHD exhibit significant improvement of symptoms of inattention, hyperactivity and impulsivity and/or at school and at home with the proper use of drugs”.
Cypel claims to be used one of the medications of three groups: 1-Stimulants: Ritalin, Dexedrine and Cylert; 2-Antidepressants: Tofranil, Norpramine; 3-(Melleril) Antipsychotic and anticonvulsant (Tegretol). Drug intervention is used for the improvement of the symptoms of ADHD, psychostimulant medication being that most benefits the control of impulsivity and behaviour. Therapeutic approaches assist the bearer of ADHD, but the most important aspect in any disorder treatment strategy is the positive reinforcement of the expected behavior.
3. THE BEARER OF ADHD IN SCHOOL ENVIRONMENT
More and more teachers care about ADHD, because besides causing difficulties in learning, the student presents inappropriate behaviors in the classroom.
As Miguel (1995, p. 25) “demoralization and low self-esteem can be associated with learning difficulties. The child with learning disabilities often is labeled, being called the upset, unable or delayed “. The school has a relevant role in the rescue of self-image and responsibility in uncovering the meaning and direction of learning. Prepare teachers to meet these children through appropriate methodology.
According to Rohde and Benczik, children with ADHD tend to present in General, average or above average intelligence. But present some problems in learning or behavior, associated with deviations from the functions of the central nervous system, causing difficulties in perception, conceptualization, language, memory, attention, motor function and impulsiveness. Education is a social practice that culminates in the education process mediated by the educator that occurs spontaneously, favoring the affective and cognitive development respecting the limitations.
The choice of tasks must be done in order to enable it to be successful. Make interesting tasks and make the reward worth appears to be extremely important for people with ADHD. “First of all, it must be sure you’re dealing with ADHD; the teacher must have the support of the school and the parents; establish rules and guidelines; always look in the eye and be firm; Divide the large tasks into smaller tasks; Leave the classroom for a few moments; Feed the children with ADHD with encouragement and praise “(HALLOWEL and RATEY, 1998, p. 74-75).
According to Fernandez (1990, p. 67) “When the scholastic failure, professionals (Audiologists, psychologists, teachers, educational psychologists) must intervene, helping through appropriate indications”.
The task of the school is relevant with regard to the rescue of the self-image of the child.
3.1 ADHD AND LEARNING DISABILITIES
The difficulties found by the inclusion of the student carrying ADHD educational projects of a regular school. In Thailand, in Jomtien in 1990, the United Nations (UN), the United Nations Educational, scientific and Cultural Organization (UNESCO) and other international agencies have initiated a project aimed at solving the problem of discrimination of 1,000,000 children without opportunity of education worldwide.
The inclusion is a social movement in defense of people excluded, were created laws and programmes aimed at guaranteeing the rights, as the policy of inclusive education (BRAZIL, 1994). The law of Guidelines and Bases for national education-LDB (Law No. 9394/96) establishes equal conditions for access and permanence in school and recommends that the education of students with special needs to occur in regular schools.
The assessment carried out by a multidisciplinary team medical, psychological, educational and relational diagnosis of ADHD notes the relevance of social representations in the school environment, because according to the law of Guidelines and Bases of education-LDB (BRAZIL, 1996) “Art 1-education covers the formative processes that develop in family life, in human coexistence, at work, in educational institutions and research , social movements and civil society organizations and in the cultural events “.
The LDB, law No. 9,394 of 1996, in his Art. 58 the term special education, for the purposes of this Act, the school education mode, preferably on regular network offered education for students with special needs. In Art. 59 education systems shall ensure to learners with special needs-item I – curricula, methods, techniques, educational resources and specific organisation, to meet your needs.
The ADHD symptoms manifest themselves noticeably in the school environment. At the beginning of school life the greatest difficulties arise because the child does not adapt to routines and rules to follow, attracts attention negatively causing disorder in the classroom, by agitated, inattentive and impulsive. ADHD can affect the reading, writing and other areas affecting student’s cognitive learning.
For student development in this condition it is necessary that the educator is focused on the potential of children, because as Vygosky (1992) “it is impossible to rely on missing a child, what she is not. It is necessary to have an idea, even if it is vague about what she has and what she is. ”
3.1 FOLLOW-UP TO THE TEACHER
The teacher’s role of mediator of learning and guiding children’s production. The stimulus must be the focus of work, effective monitoring is important to secure the student. The relationship between pupil/teacher is of paramount importance to learning.
According to Rohde and Benczik (1999), there is a need for a pedagogical follow-up carried out by the teacher, in order to prevent gaps in learning. It is observed that the teacher should be aware of the difficulties presented. The disorder affects many aspects of life of the child and may introduce improvements in some symptoms. The meeting of reality brings concepts that can help in the understanding of conflicts, perception, understanding the different, the acceptance of the inclusion.
The use of strategies assists the teacher in control of student behavior in the classroom: appreciation of the strengths, rules, rewards and motivation. The school seeks to develop a consistent work to the reality of the students focused on working together, creating opportunities for interaction with the support of approaches, convivial spaces as tools to assist students and teachers in cognitive processes, in order to promote learning based on valuation and human respect.
“The child develops intelligence for their ability to interact with the environment in which he lives, his intellectual development happens gradually, and can be slow or fast depending on the established Exchange with the environment into which it is inserted” (PIAGET, 1978, p. 29).
The conniving of parental anxieties teacher and child, makes room for the hope and confidence that predispose to the effort to overcome the difficulties. Children are perceptive and need a warm and kind to produce satisfactory results.
3.2 CLINICAL FOLLOW-UP
The Pediatric neurologists became a professional requested recognize children with changes in areas of development as learning and behavior, these referrals are the doubts of parents or teachers about the source of the problem, if it follows a framework that undermines important brain functions organic to the academic and social relations of the child.
ADHD is a neurobiological disease can cause a widespread commitment information processing by the Central Nervous System, it is necessary that children are subjected to a thorough investigation of brain function such as behavior, attention, perception, language, coordination and memory. These evaluations should integrate the opinion of professionals from multidisciplinary areas. The information of family members and teachers, applied the operational criteria of the DSM-IV and carried out specific tests for identification of compromised brain function.
Multidisciplinary assessments procedures solve the difficulties of interpreting the symptoms in most cases. Depending on the needs the investigation should be terminated with the additional exams. The differential diagnosis involves the use of scales of behavior and the application of the criteria of the DSM-IV.
An adequate flow to the diagnosis can be summarized as follows:
- 1-A thorough medical history to determine if suspicions of ADHD are relevant;
- -Data collection with the parents about the child’s history-Pregnancy, Childbirth, disease personal and family background, behavior, cognition, as it establishes links with other people;
- -Data collection with the child about the impression she has of its capabilities and behavior and what it causes in people with whom she relates;
- 2 – physical examination to identify possible signs of systemic diseases;
- 3 – evolutionary neurological exam to identify specific brain deficits;
- 4 – additional tests for differential diagnosis with other pathologies;
- 5-Questionnaires with DSM-IV items answered by parents, teachers and children to operational Diagnostics;
- 6-psicoeducacional-academic skills Assessment, psychometric tests;
- 7-speech-Review language and phonological processing functions;
- 8-integration of diagnosis among professionals;
- 9 – guidance to parents and children about the diagnosis and therapeutic resources available;
- 10-issuing a report for school.
4. METHODOLOGY
This study was carried out by means of bibliographical research and field, with a quantitative and qualitative approach, descriptive, correlational research level and non-experimental. The instruments used were questionnaires and observation, seeking to identify the difficulties of learning and literacy for four students with ADHD from the third grade of elementary school of the Municipal school Hafizabad, flush-MG. Basic education-early childhood education first and second periods and primary education from 1st to 5th grade. The data were collected in order to achieve the proposed objectives. Graphics and Tables statements were executed for analysis and discussion.
5. RESULTS AND DISCUSSION
This study sought to support theoretical us Barkley, Mattos, Rodhe, and Vygotsky, among others, to substantiate this investigation. A questionnaire was applied to ten school teachers on the difficulties encountered in the inclusion and literacy of students with ADHD.
Chart 1-In his academic training acquired knowledge about Inclusion?
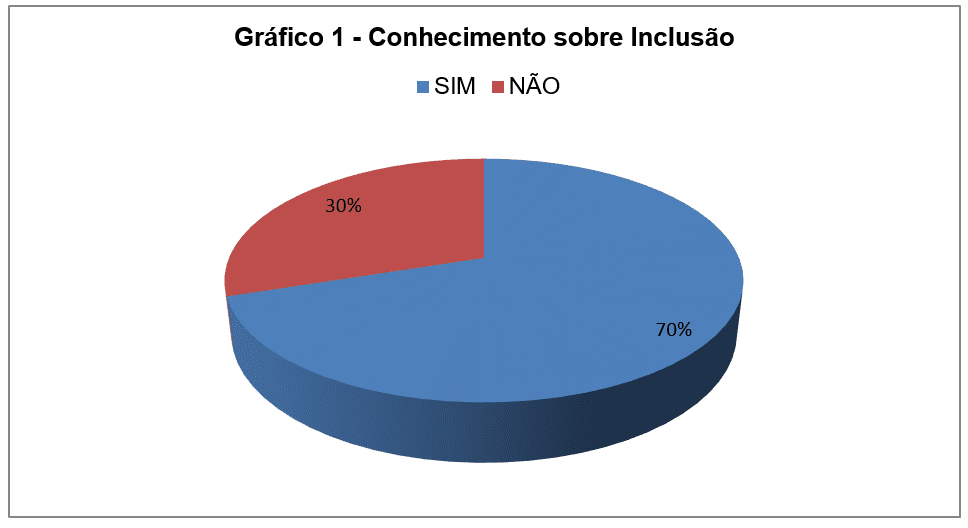
The result shows that the majority of teachers surveyed have knowledge about the inclusion in their academic training.
The inclusion is a reality in educational institutions, as “special education: a right ensured”-Secretary of special education – MEC (1994).
“Inclusion is to give conditions for children with educational need take ownership of knowledge and are able to develop fundamental human structures of thought, through the social interactions in your school environment” (VYGOTSKY, 1996).
Graph 2-what resources are available to the school for inclusion?
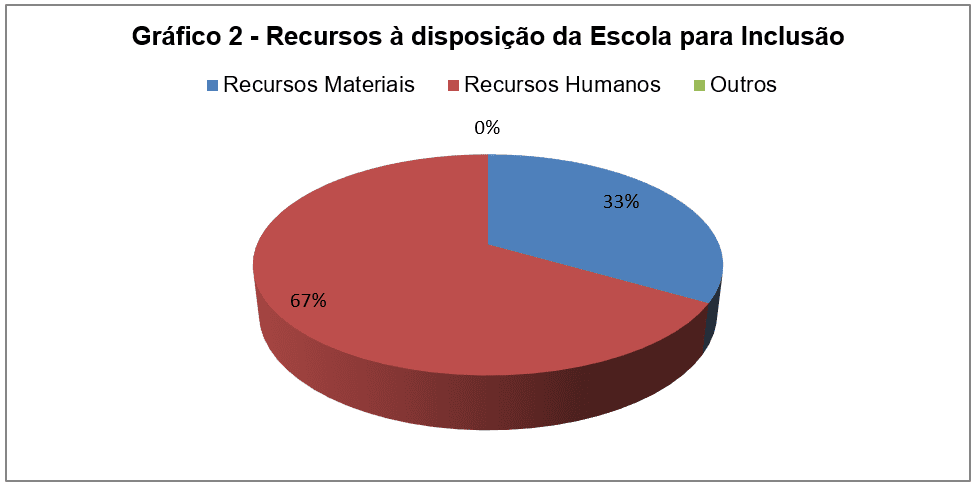
The result shows that the human resources are at the disposal of the school for inclusion.
The Special education curriculum guidelines on basic education, in accordance with the LDB and the national policy of Education (1994), warrant that the services will be offered in schools in the form of material and human equipment capable of pedagogical practice’s performance while ensuring a quality educational response to special educational needs.
Graph 3-the city supports the school administration of inclusive education?
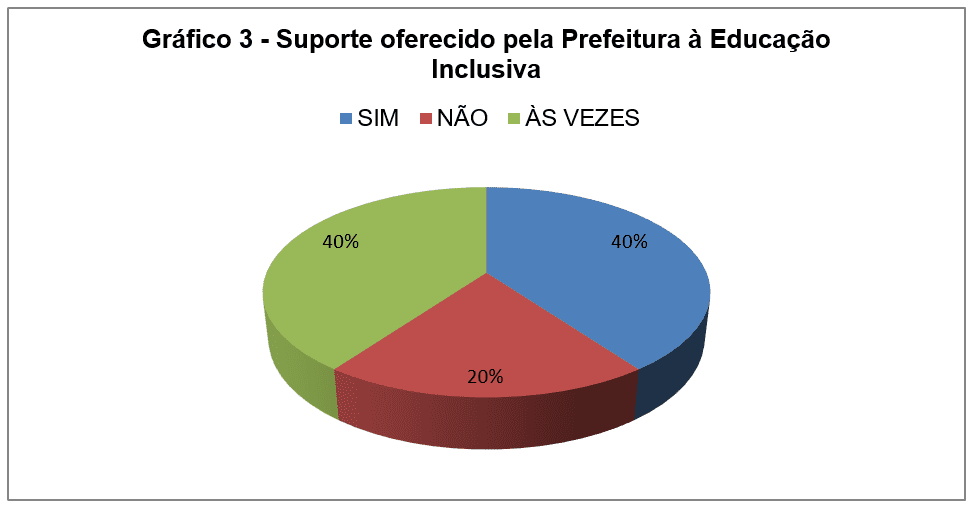
Second result, 40% say the city supports inclusive education, by providing a psychologist and support teachers for special students. 40% claimed that sometimes because a psychologist does not meet the demand of the city schools.
To address the difficulties uncertainty leads to conflicted feelings in order to fulfill the function of education. Special education is delivered, preferably on regular network of education, for students with special needs in accordance with chapter V, article 58 of the LDB committed to offer all students a quality education. However, the proposals and laws formalized and legalized are not always fulfilled.
Graph 4-the school offers educational support to facilitate your work with students suffering from ADHD?
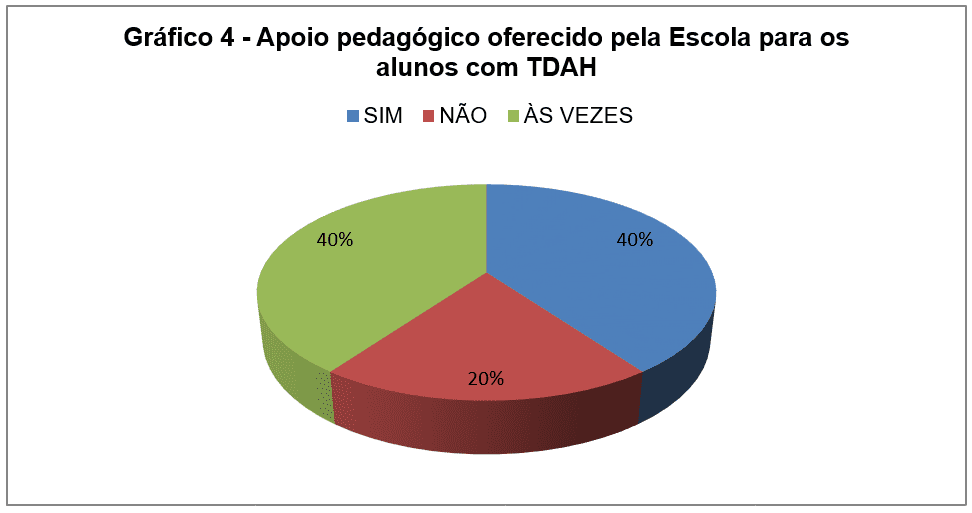
Second result, the school offers educational support to work with students with ADHD and concurrency issues.
According to the Art. 8 The regular schools of education must anticipate and provide in organizing their common classes: I – common classes and teachers of special education, trained and specialize, respectively, to attend the educational needs of the students.
Chart 5-What are the major difficulties for literate students with ADHD?
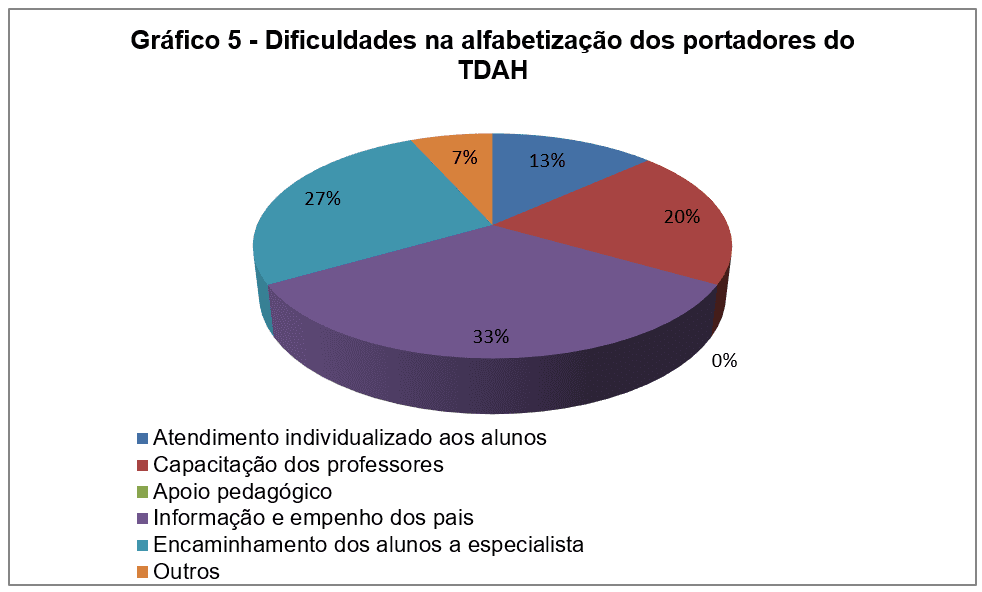
Second result the greatest difficulties are: 33% lack of information and commitment of parents, 27% need the forwarding students 20%, training of specialist teachers 13% individualized customer service to students and 7% other.
The difficulties presented in the learning and literacy of the students with ADHD cause various conflicts. Note the importance of pedagogical intervention to forward these students for a possible diagnosis for the disorder don’t just on suspicion or labels (ROHDE, 1999, p. 65).
Chart 6-In your opinion, the system of inclusion in regular education school has made positive results?
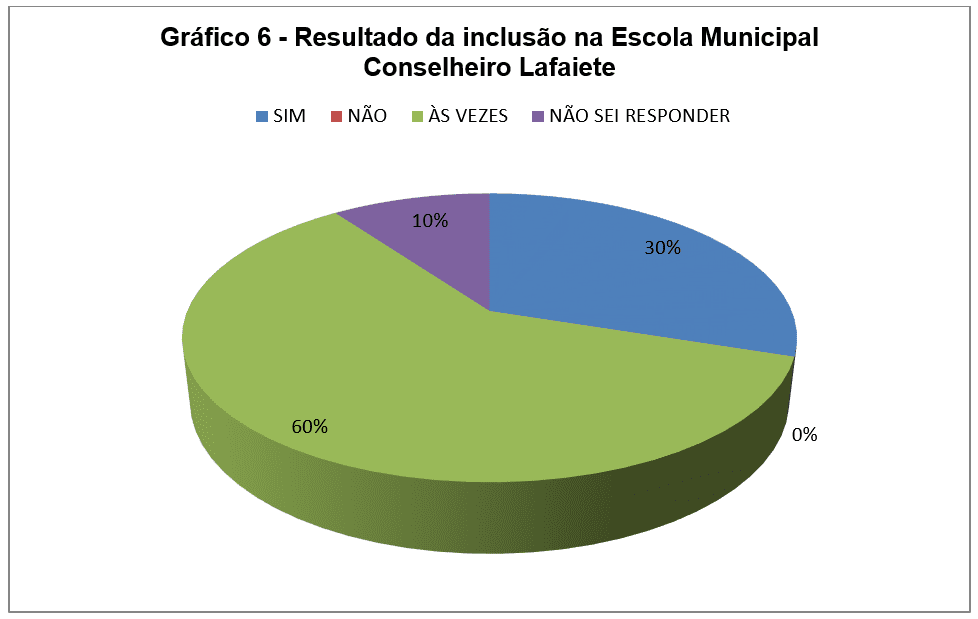
As a result, 60% of the teachers stated that sometimes the system of inclusion in regular education school makes positive results.
“The inclusive education can be considered a new school culture: a design school that aims at developing educational responses that reach all students” (GLAT and BLANCO, 2007, p. 16).
Table 1: intervention actions are used for the inclusion of the student with ADHD?
| PROFESSOR | REPLY |
| P1 | I like to organize the classroom environment separately, moving the children to place each week to socialization. |
| P2 | I try to bring them from other students through games. |
| P3 | Keep the student with difficulty always close to me to avoid turmoil in the room. |
| P4 | Work the inclusion of the child with the other helping to overcome their fears and difficulties. |
| P5 | Put in wallet near my desk and make jokes to socialization of students. |
| P6 | Do activities of doubles for interaction of the students. |
| P7 | Immediately have a conversation to understand what’s going on, after I do a group dynamics for the insertion of all students. |
| P8 | Do the children’s awareness regarding inclusion with stories and short texts. |
| P9 | Work together with the teacher. |
| P10 | Preparation group activities so that there is interaction with the other kids out of the room. |
Source: survey conducted on Escola Municipal Hafizabad
According to the teachers intervention actions for inclusion denotes socialization. Vygotsky (1996) States that social interaction is a fundamental condition for human development.
To Barkley (2002) interventions should be applied consistently, including proactive strategies on how to know to handle events background to prevent challenging behaviors and reactive strategies, providing consequences, for example, giving positive reinforcement to the desired behavior.
“The inclusive education can be considered a new school culture: a design school that aims at developing educational responses that reach all students” (GLAT and BLANCO, 2007, p. 16).
Table 2: you use different methodology in the process of literacy of the students with ADHD?
| PROFESSOR | REPLY |
| P1 | Plan the lessons appropriate to the students ‘ level and use resources to facilitate the learning of the student with ADHD. |
| P2 | I work normal activities with all students. |
| P3 | No, because it has a pedagogical support teacher in the room to monitor students with learning difficulties. |
| P4 | Work with different activities and methodologies that consist of facilitate the resolution of the tasks for the child with ADHD. |
| P5 | Preparation group activities for cognitive, intellectual and affective interaction of students. |
| P6 | Do the lesson plan with attractive activities to attract the attention of the student carrying ADHD by stimulating it to the teaching learning process. |
| P7 | Encourage the ADHD Student through rewards and praise every progress achieved. |
| P8 | The follow-up single of the student with ADHD is accomplished by supporting teacher in the classroom. |
| P9 | Seek always work the contents with different methodology to motivate students with ADHD as their potential. |
| P10 | Seeking to present the contents of playful way for better understanding. |
Source: survey conducted on Escola Municipal Hafizabad
As a result, most teachers presents the contents seeking to reach all students in class, using different methodology in the process of literacy of the students with ADHD.
According to Barkley (2002, p. 244) “students ‘ attention can be improved with a more enthusiastic classroom style, short and active participation of the child”. Learning happens through interaction, activities must be appropriate, the child should be stimulated and clear rules.
“The child develops intelligence for their ability to interact with the environment in which he lives, his intellectual development happens gradually, and can be slow or fast depending on the established Exchange with the environment into which it is inserted” (PIAGET, 1978, p. 29).
Some students present concurrent problems such as hearing impairment and visual committing even more learning. “The literacy process of children with ADHD should be worked to meet its specificity, no highlight your disability, by the absence of necessary stimuli for their psychosocial development” (VYGOTSKY, 1996).
Concrete materials should assist in the teaching-learning process, through the playful is possible to work the attention, concentration, motor skills and memory.
According to Goldstein (1998, p. 45) “need to make interesting tasks and make the reward worth appears to be extremely important for people with ADHD”.
DISCUSSION
The results of the research show ADHD as a disorder that affects learning causing difficulties in child literacy, generating insecurity and anxiety. Teachers and parents recognize and blame the ADHD disorder by behaviors presented by students, which can be verified in the intellectual and cognitive development of the same, because “the attention deficit disorder/hyperactivity disorder is a real disorder, a real problem and often a real obstacle” (BARKLEY, 2002, p. 35).
Vygotsky (1996) argues that development depends on family, social and school context in which the child is inserted. Parents are the main agents of socialization of the child, the school and the teacher becomes part of the context of the child and his family.
The observation and analysis of the data allowed better understanding in relation to the learning and development of children with ADHD:
- to the literacy Aspects) of students with ADHD: school phase the lack of attention is manifested most often, when cognitive activity is most required. The impulsivity and hyperactivity are manifested by agitation and precipitation, interruptions and difficulties to wait your turn. ADHD diagnosis is clinical and is considered final only for a mental health professional.
- b) action of the teacher on student behavior ADHD carrier: the cohabitation of children with ADHD and the other is relevant, because to Vygotsky (1996) socializing means establishing bridges of mediation/interaction for knowledge construction and not simply occupy a place in that environment and have to fit pre-established patterns historically without deeper modifications occur in the organizational structure and the pedagogical school environment.
- c) Actions for the inclusion of the student with ADHD: social interaction is a fundamental condition for human development. In this context, teachers and parents are social mediators for the formation of higher psychological functions that are achieved through the social construction, learning is developed in the child when she interacts with people in your environment.
IDENTIFICATION OF PARTICIPANTS
Students with ADHD were identified as: A1, A2, A3 and A4 and supporting teacher as PA.
Table 3:3rd year students with ADHD diagnosis
| STUDENTS | DIAGNOSIS |
| A1 | ADHD, carrier medical report: the A1 has 8 years of age, was diagnosed as a carrier of ADHD, cerebral arrhythmia and delayed mental development, hearing impairment and low vision, makes use of medication (Tegretol). Follow-up: clinical psychologist, ENT, neurologist, ophthalmologist and speech therapist. |
| A2 | ADHD, carrier medical report: the A2 has 8 years of age, diagnosed with ADHD impulsive attitudes, difficulty focusing attention, mental dispersion. Muscle tone with a slight hipotomia that interferes in speech and coordination visomotora. Makes use of medication (Tegretol). The psychologist referred for occupational therapy, speech language pathologist requested neurological care and psychological assessment to verify the level of General Intelligence and linguistic understanding. The neurologist indicated psychological, psychology and teacher support. |
| A3 | ADHD, carrier medical report: the A3 has 8 years of age, was diagnosed with ADHD and requires individualized accompaniment in the classroom. Makes use of medication (Tegretol). The psychologist testified that the student presents mild intellectual disabilities and speech therapist diagnosed tonal audiometry and vocals.
According to the mother’s background, two maternal uncles with psychological problems. A3 was compromised of seizure to 7 months and 6 years requiring oxygen. |
| A4 | ADHD, carrier medical report: the A4 has 8 years of age, was transferred from APAE with diagnosis of the psychologist to attend as current legislation the public school system. According to your right should be accompanied by specialized teachers for there to be progress in their learning. |
Source: survey conducted on Escola Municipal Hafizabad
The survey noted issues that involve learning and cognitive development of children with ADHD in the school environment, the following points were discussed: the inclusion and the difficulties in literacy of the students of the third grade of elementary school.
“The note presents as main advantage, compared to other techniques, that the facts are perceived directly, without any intermediary. Thereby, the subjectivity that permeates the entire process of social research, tends to be reduced “(GIL, 2002, p. 109).
Comorbidities are associated with ADHD. The anguish and anxiety caused by excess of inattention, forgetfulness and hyperactivity in the patient with diagnosis of ADHD can add new symptoms and the appearance of other disorders.
Epidemiological studies performed in children with ADHD documenting a high incidence of comorbid psychiatric disorders (RODHE and BENCZIK, 1999).
The treatment of ADHD becomes most effective when conducted by a multidisciplinary team, including health and education professionals, with a view to improving the quality of life of the child.
Cognitive/Behavioral report of students A1, A2, A3 and A4:
A1-assiduous student and literate. Has poor eyesight and hearing, but that does not compromise the achievement of the basic activities. Visual perception is affected, has difficulty in activities involving the visual memory. The perception and auditory memory require support, to improve hearing, uses the hearing aid, daily, connected to the microphone of Professor Regent. Is restless, rises to communicate with colleagues, demonstrates interest in teaching and carries out the proposed activities in the classroom, ask the teacher to support when you have questions. Presents a good read, good relationship with colleagues and professionals in the school, respecting them and treating everyone with education.
A2-assiduous student, finds it difficult to concentrate on activities in the classroom and follow the rules. Does not perform the tasks in its entirety showing discouragement and fatigue, but soon heads off to play games and other activities. Have difficulty in reading and interpretation.
A3-assiduous student, carries out the activities proposed when monitored by the teacher, has difficulty concentrating. Write words with simple syllables and read short texts. The student needs the aid of teacher support, since it gets distracted easily. This happens daily monitoring and interventions are carried out in accordance with the needs of the student.
A4-assiduous student and live in harmony with colleagues, presents slow development in relation to their age. Not mastered the skills of reading, writing and interpretation. Reveals thin and thick motor skills, logical sequence, inadequate visual perception to his age. The student presents difficulties to hear and understand the command, requiring concentration of look for understanding of the facts. Presents difficulties of diction, which can also be compromising your academic achievement.
The students observed the A1 in spite of the difficulties related to ADHD, in relation to the content, within its limitations, accompanies the level of other students of your living room. The A2 shown inattentive, likes to perform activities paired with the A1 for being protected by the same. A3 the most hyperactive of students surveyed. The A4 demonstrates greater difficulty in learning retention. According to the PA (Teacher support) the evaluation of the students surveyed is accomplished through PDI (individual development plan). Support teacher’s work is of extreme importance and contribution in the process of developing the student with ADHD, accompanying it with the other students in the room. It was found that the support teacher provides students with ADHD a differentiated education in the room.
The note presents as main advantage, compared to other techniques, that the facts are perceived directly, without any intermediary. Thereby, the subjectivity that permeates the entire process of social research, tends to be reduced. (GIL, 2002. p. 109)
CONCLUSION
In view of the above it is concluded that the effects of ADHD and the difficulties presented in the phase of literacy can be softened, enabling children to develop cognitive, affective and emotional methodologies and interventions that enhance their potential and creativity. To this end, it is essential to know the history of the student and their difficulties. The role of the family, school and teacher it is essential to include the child bearer of ADHD. It is essential the applicability of inclusion through the intervention of the teacher, providing opportunities for interaction with the other students in the confrontation of different situations in the classroom as conflicts, dialogues, troubleshooting and limitations.
In this context, the interventions provide the understanding of rules, allow the implementation of activities and stimulate the mutual trust, reinforce positive behaviors and stimulate the participation, by inhibiting the characteristics of ADHD, contributing to the reduction of inattention and impulsivity, strengthening the concentration, persistence and self-confidence.
Access to reality of the child allows the observation of hardships of the student with ADHD, channeling the knowledge of facts and situations manifest in social coexistence offering a satisfactory answer to this question. The information provided by the teacher-student interaction confirms the importance of methodology employed, involving cognitive, behavioral, social and emotional, whereas each student as a social being.
The study enabled elements to respond to the research problem, favored the finding, facilitating the obtaining of data of the objects studied, channeling the knowledge of facts and situations manifest in social coexistence offering a satisfactory answer to this question. The record of information took into account the objectives of the research. Therefore, the contribution to the field school was show that the inclusion is essential in the teaching-learning process, as well as on children’s literacy.
The recovery of the child with ADHD and their education should be prioritized in all segments of life, because it is a training process where the family, school and society are responsible.
REFERENCES
ABDA-Brazilian Association of attention. ADHD LAW Primer (Doctrine-Jurisprudence). Available at: http://www.tdah.org.br/images/stories/site/pdf/cartilha_legislacao.final.pdf. Access in: 27 June 2016.
BARKLEY, Russell a. attention deficit disorder/Hyperactivity. Porto Alegre: NEW HAVEN, 2002.
Brazil. Ministry of education. Guidelines and Bases of education LDB 9,394. Brasilia, 1996.
ICD-10. International statistical classification of diseases and Related Health Problems. F00-F99 chapter V: classification of mental and behavioural disorders. USP, 1988.
CYPEL, Saul. Attention deficit hyperactivity disorder. São Paulo: Read Editorial, 2001.
DSM-IV-TR-diagnostic and Statistical Manual of mental disorders. New Haven, London, 2002.
FERNANDEZ, A. The intelligence trapped: psychopedagogical clinic Approach of your child and your family. Porto Alegre: medical arts, 1990.
GLAT, Rosana; BLANCO, Leila m. v. (org.). Inclusive education: culture and daily life. Rio de Janeiro: 7 Letters, 2007.
GIL, Antonio Carlos. How to write research project. 4 ed. São Paulo: Atlas, 2002.
GOLDSTEIN, s. Hyperactivity: how to develop the ability of the child. Campinas, SP: Papirus, 1998.
GOLDSTEIN, S.; GOLDSTEIN, m. Hyperactivity – how to develop the ability of the child. 9 ed. São Paulo: Editora Papirus, 2003.
WAR, L. B. The child with learning disabilities. Rio de Janeiro: Ed. Enelivros, 2002.
HALLOWEL, E. & JOHN RATEY (Trad. CARVALHO, Andre) tendency to talk: identification and management of attention deficit disorder from childhood to adult life. Rio de Janeiro: 1998.
MATTOS, P. In the world of the Moon: questions and answers about the disorder and Attention deficit hyperactivity disorder in children, adolescents and adults. São Paulo: Editora Lemos, 2003.
Piaget, Jean. Problems of genetic epistemology. (Translation of Celia and a. Di Piero). In: Piaget/Thinkers. São Paulo: Cultural, April 1978.
ROHDE, l. a. & BENCZIK, and b. p. attention deficit disorder/Hyperactivity. What is it? How can I help? Porto Alegre:/editora New Haven, 1999.
ROHDE, Louis A.; Paulo MATTOS et al. Principles and practice in attention deficit/hyperactivity disorder. Porto Alegre: NEW HAVEN, 2003.
TOPCZEWSKI, Open. ADHD: how to deal? São Paulo: Psychologist’s House, 1999.
UNESCO. Declaration of Salamanca. Salamanca: World Conference on special education, 1994.
VYGOTSKY, l. s. complete works: Foundation of defectologia. Cuba-Havana: Editorial Pueblo and Educación, 1989, v. 5.
VYGOTSKY, L.S. The social formation of mind. 5th Ed. São Paulo: Martins Fontes, 1996.
[1] Graduated in Pedagogy, postgraduate degree in educational psychology, Master in education by Unigrendal. Street Pe. André Colli, 35-Bairro Nossa Sra. de Fátima-Flush/MG, Brazil.
[2] Doctor of education, a professor at The College And University — GCU Grendal.