ANDRADE, Nívea Cristiane de Sousa de [1]
ANDRADE, Nívea Cristiane de Sousa de. Nursing care the arteriovenous fistulas: literature review. Multidisciplinary Core scientific journal of knowledge. Year 1. Vol. 9. pp. 88-106, October/November 2016. ISSN. 2448-0959
SUMMARY
Hemodialysis for arteriovenous Fistula is a therapeutic modality of greater choice, because it is a vascular access that offers greater durability in the treatment and offering less risks of complications. The nurse plays an important role in the early identification of those complications and in the maintenance of arteriovenous fistula (AVF), through excellence in patient care with AVF. This study had as its main purpose to meet the nursing care of arteriovenous fistulas in patients with chronic renal failure. The methodology adopted was literature review in books, electronic journal and scientific articles that addressed the theme about chronic kidney disease, arteriovenous fistula, hemodialysis, nursing care in FAV. Were accessed in the databases csielo, lilacs, virtual health library, master’s thesis published in the last nine years (2005 to 2014). As for the discussion of results the authors were unanimous with regard to the training of nurses in the care of the patient with AVF. The study made it possible to meet the nursing care to arteriovenous fistula and concludes that the nurse Substititiva Renal Therapy service must be a specialist in Nephrology, endowed with technical and scientific knowledge in relation to the preparation and maintenance of arteriovenous fistula, ensuring durability the FAV and the extension of the life of the patient.
Key words: Hemodialysis; Nursing care; Arteriovenous fistula.
1. INTRODUCTION
According to the Brazilian Society of Nephrology in 2008: in the world about one million and 200,000 people are under under hemodialysis treatment. In Brazil, there are approximately 87,044 patients per year, of which 89.4% are in renal substitutive therapy program (COSTA, 2011).
The Online Diary after report with Sespa, in which informs you that in 2011 in Pará there are about of 1,674 patients in dialysis treatment. Already in the year 2013 the number of chronic kidney patients reaches 2000 people on dialysis treatment in Pará as the President of the Brazilian Society alert of Nephrology-Stop Regional, Luis Claudio Pinto.
Second Prezotto (2014) Chronic Renal failure is being considered a major public health problem, with considerable increase in the number of chronic kidney patients in the brazilian population, these data confirmed by the Census 2011 dialysis Brazilian society of Nephrology, where the number of patients with IRC corresponds to an approximate total of 50,128.
Milk et. Al, (2013) and Delhi (2014) confirm that the chronic kidney failure comes reaching relevant proportions within public health, because of the growing number of people affected by disease requiring hemodialysis.
Given that every year grows the number of cases of patients with chronic renal failure on hemodialysis for arteriovenous fistula, this being the highest mode choice. (Milk, 2013).
Hemodialysis for arteriovenous Fistula is a therapeutic modality of greater choice, being a long-lasting and safe access, MILK (2013). Sharma, (2011) adds that the arteriovenous fistula (AVF) presents a survival adequate and has low rate of complications.
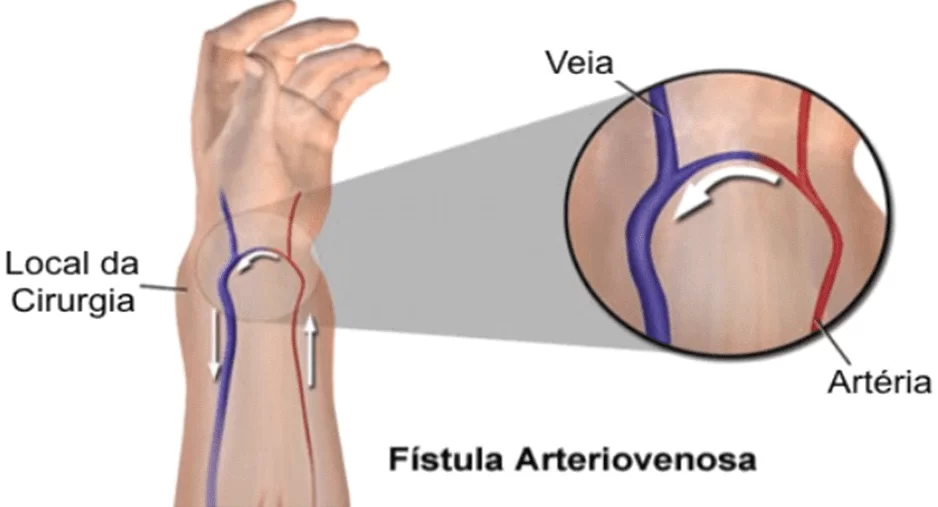
For Daugirdas (2010), hemodialysis is done after the making of an arteriovenous fistula, which is formed by a subcutaneous anastomosis of one artery by a native vein adjacent, allowing the direct flow of the artery to the vein.
Fistulas are made in the arm handle (radiocefálica), in the lower arm (ulnar-Basilica), elbow (brachiocephalic) (DAUGIRDAS, 2010).
Despite being a simple procedure, proper planning of the site of anastomosis, which should be in the preoperative and postoperative and setting the time for the beginning of the clip are fundamental to the success of the surgery (TOREGLANI, 2008).
For this it is necessary to also reduce the problems evidenced with arteriovenous Fistula: thrombosis, lower blood pressure, narrowing of vessel, decreased flow because repeated punctures, bruises, hemorrhages, ischemia in the Member with fistula, these Problems that make patients lose fistulas before five years, this time established by Anvisa. (ANVISA, 2014); (POLIMANTI, 2012).
As described in Barros (apud white, 2005) “the FAV care should be followed in order to increase survival and prevent complications arising from the use.
Patients with chronic kidney failure need to increase survival of fistulas, because they rely on dialysis to survive. Whereas a few manuals and protocols regarding nursing care to patients with CRF patients with arteriovenous Fistula is to formulate the following question: what is the nursing care provided to patients with arteriovenous fistula patients with IRC?
The research is justified by the high rate of individuals with chronic renal failure under hemodialysis treatment in the State of Pará, study this that becomes important to improvement in the quality of nursing care in arteriovenous fistulas in patients with chronic renal failure, establish and maintain a durable and reliable access, offering high rates of blood flow associated with low rates of complications is essential. Whereas the nurse plays an important role in the early identification of those complications in arteriovenous fistula (AVF), through the care provided to the client with chronic renal failure (CRF) with AVF. This study had as its main purpose to meet the nursing care of arteriovenous fistulas in patients with chronic renal failure. The methodology adopted was an exploratory study, by means of bibliographical research in books, electronic journal and scientific articles that addressed the theme about chronic kidney disease, arteriovenous fistula, hemodialysis, nursing care in FAV. Were accessed in the databases csielo, lilacs, virtual health library, master’s thesis published in the last nine years (2005 to 2014).
2. LITERATURE REVIEW
2.1 THIS STUDY ABOUT NURSING CARE FOR THE PATIENT WITH ARTERIOVENOUS FISTULA OF CHRONIC KIDNEY FAILURE
Second Smeltzer, (2009); Daugirdas, (2010) kidney failure results when the kidneys cannot remove metabolic wastes from the body or perform their regulatory functions. The substances usually eliminated in the urine accumulate organic fluids as a result of impaired renal excretion, leading to disruption in the endocrine and metabolic functions, as well as water and electrolyte disorders-basic acid as a result of this disorder that makes the use of hemodialysis to remove liquids and residues urêmicos of the body when the kidneys are not able to do it.
To Brunner & Suddarth, (2009) the dialysis is the process of filtering and purification of the blood which aims to extract nitrogenous toxic substances from the blood and remove excess water by replacing the damaged kidney functions, thus prolonging the life of patients with chronic renal insufficiency.
The arteriovenous Fistula is the permanent vascular access safer and longer-lasting, used in renal patients and consists of a subcutaneous anastomosis of one artery with a vein that takes about 30 days to mature and is usually made of non-dominant arm for not limiting the patient’s activities wing (ANVISA, 2014; Fermi, 2011; DAUGIRDAS, 2010; Milk, 2013).
2.1 TYPES OF ARTERIOVENOUS FISTULAS AND LOCATION
Fistulas are given title according to the connected vessels: Radiocefálica made in the fist is the first choice as a means of access, because it is simple to be created, have low morbidity and preseva a great following of vein to be punctured and enables the creation of other hits on the same Member (FERMI, 2011).
Brachiocephalic made in the elbow is the second choice, because its advantage is the high flow compared to the handle and the fact of the cephalic vein easier to puncture, this presents some difficulties fistula in his clothing, as it has a limitation on the elbow and upper limb edema may occur and theft nofenômeno (fistula Member ischemia caused by the siphoning off of circulation) (DAS NEVES JÚNIOR , 2011; Fermi, 2011).
For Daurgirdas, (2010); DAS Neves Júnior, (2011) there are other fistulas less used are: ulnar fistula-Basilica is anastomosis between the Basilic vein with the ulnar artery is located in the forearm; braquiobasílica the Basilic vein anastomosa-if the brachial artery; radiobasílica that anastomosa-if the radial artery with the Basilic vein. Less frequently used options are the Gracz fistula (which uses the vein that puncture veins arterializa Basilica and the cephalic arm) and the cephalic fistula brachial bidirectional (which arterializa the cephalic veins in the arm and forearm). When all the locations in the non-dominant arm were exhausted, the dominant arm can be used.
SHAH, (2009) the nursing has the key role in the care of the patient with arteriovenous fistula in both pre-and post-surgery, as acts with the client watching so humane and capable, with the goal of making the customer get back their normal activities.
2.2 NURSING CARE IN PREOPERATIVE PERIOD OF PATIENTS WITH ARTERIOVENOUS FISTULA
Normally the FAV is built on the dominant member identifies with a bracelet this arm, the nurse should guide the patient and the nursing staff so that they will not be allowed to catheterize, punctures, blood pressure check for making the fistula (SHAH, 2009). White, (2005) affirms the need to direct the customers pre-dialíticos about the importance of his vases, evaluate the early indication of site access, respect the maturation period, avoid do dialysis on the day of surgery, and suggests that the nurses should have knowledge and continuous training on access, know how it works, as puncture as wear and early diagnosis of the complications.
2.3 NURSING CARE IN THE POSTOPERATIVE PERIOD OF ARTERIOVENOUS FISTULA
The care adopted in the period pós-confecção surgical fistula are fundamental to the adequacy of hemodialysis access, and involve: the elevation of the Member in the early days, periodic exchange of dressings for the nurse and perform manual compression exercises with rubber ball to promote the maturation of venous access (MANIVA, 2009).
2.4 FAV CARE OF PATIENTS
The patient must be guided by nursing and need to implement some care with the fistula, among which include: perform daily exercise with rubber ball compression for fifteen minutes three times a day helps keep the fistula; observe any change in the location of the fistula, as heat, pain, Erythema, and swelling, palpation and perception of the thrill (vibration noticeable due to arterial blood mix with deoxygenated blood), any abnormality should be reported medical and nursing teams; avoid venous puncture and check blood pressure in the arm of the fistula; avoid checking blood pressure in this member, sleeping on the arm of access and any compression, should not remove or allow removal of hair and scabs formed in the region of the fistula. (CASSAVA, 2009; Fermi, 2011).
2.5 NURSING BEFORE HEMODIÁLIÁLISE SESSION
In the dialysis unit, before the puncture, patients should wash the Member what are the fistula with soapy water or another antiseptic solution, empty the bladder, check the weight calculating the final weight and initial to stipulate whether the signals going to ultrafiltration (blood pressure, temperature, pulse and respiration), mainly because the blood pressure severe hypotension can lead to total cessation of fistula says Fermi, (2011); observe concentrations and temperature of the solution dialisadora; check the operation of the machine and prepare all the material necessary for the patient to perform hemodialysis; (White, 2005).
2.5.1 ASEPSIS FISTULA
As described by Fermi, (2011) the asepsis of the fistula should be cleaned with antiseptic solution, according to the standardization of control program dede infection prevention and adverse effects (PCPIEA), after asepsis is the arterial puncture should stay away 3 cm of the anastomosis to prevent fistula thrombosis, venipuncture should stay away from the two-inch blood from each other in order to avoid blood recirculation. According to the Handbook of dialysis, (2012) the antiseptic solution before the puncture is the 70% alcohol with cotton balls.
2.5.2 CHOOSING THE NEEDLE
Choosing the proper needle for each type of fistula is of extreme importance that the gauge is used in accordance with the prescribed blood flow. For a blood flow less than 250 ml needle gauge (18 g, pink); between 250 and 300 ml (17 g, orange); between 300 and 350 ml (16 g, green); between 350 and 400 ml (15 g, yellow); more than 400 ml/min (14 g, purple). The needles should be well secured to avoid trauma, bleeding, or even the output of the needle (FERMI, 2011). For Daurgirdas, (2010) during the initial use of needles are recommended (paragraph 16 to 17) and low blood flow, in mature access are necessary larger needles (15 gauge) to tolerate blood flow required (> 350 ml/min) for the high-efficiency dialysis.
2.5.3 PUNCTURE TYPE
The type of puncture more choice among the authors as Daurgirdas, (2010) was the buttonhole technique (which consists of repeated punctures in the same location, such as a button that uses the same House several times) that enables the creation of a stable tunnel between the patient’s skin and the native fistula (new or mature) should be carried out in the first 10 punches and by the same trained professional and the same court orders the angle of puncture is contraindicated in patients with flabby skin, for being hard to carry out the repeated punctures, according to Paiva, (2008) punçao arteriovenous access, only trained professional should perform this procedure, and the responsibility of every nurse first punches and the more delicate fistulas. The patient should be instructed to allow the handling of your fistula only by qualified professionals.
2.6 NURSING CARE DURING THE HEMODIALYSIS SESSION
According to Santa et. Al, 2013 during the hemodialysis session the team must be attentive to monitoring of vital signs, anticoagulation, proper operation of the dialysis machines (temperature, roller fairlead, blood flow, the drugs flow), patient comfort, complications, complaints and questions from patients, the physician’s request when needed, and the nurse should carry out supervision of assistants and technicians of the team
As for the machine and its components of hemodialysis Observe the prime, that is the amount of liquid inside the dialyzer; If the levels are elevated, in case you intend to discard partially or totally flush; Bolus-continuous, fractional; Blood flow – 150 to 200 ml/min, and after review after connecting the arterial and venous lines in the patient, the flow of blood dialysis, transmembrane pressure, arterial flow and detectors. Keep track of vitals every 30 minutes, especially the pressure, because hypotension may predispose the clotting; monitor the pressure of the venous sinus, because the increase means that access is with problems such as fistula recirculation that worsens the quality of dialysis and increases the risk of thrombosis; stay tuned as to the operation of the machine and dialisadora solution temperature; provide peaceful surroundings and comfortable leaving the client alone; administer medications as prescription; do not administer medications IM due to heparinization (white, 2005).
Silva and Nunes (2011) complement, if blood extravasation, or hematoma occurs at the moment of puncture, during the session, the needle should be removed, the location must be compressed to hemostasis and perform cold compress on site. As early as the influx (blood pressure) that is characterized by insufficient blood fonecimento to the pump, which can be caused by hypotension due to withdrawal of water and excess products through the process of osmosis, generating flow fall; vessel spasm; needle or clotted access; arterial line and bending the use of needles with incompatible blood flow, you should reposition the needle or perform a new LP, because the needle should be inserted in the vessel wall.
2.7 NURSING CARE IN THE POST PROCESS HEMODIALYSIS
According to Fermi, (2011) after removing the needles, you must exercise the compression until total hemostasis, a bleeding for more than twenty minutes should be aware of the amount of anticoagulant and antihypertensive, the dressing should only be withdrawn after 6 hours of termination of dialysis, guide to be kept dry and clean. Ribeiro already (2009) reports that the dressing should be done with a slight compression and not circular with gauze for about five minutes, with duct tape and gauze after full hemostasis. This care is crucial to avoid the heavy bleeding after hemodialysis. Hemostasis of the fistula must be made by means of direct pressure, followed by removal of the needle to prevent hematoma formation on site, as well as control the bleeding into the skin (P, 2008).
As Santa et. Al, (2013) at the end of the session, when removing the patient from the machine care must be taken so that there is greater return of blood to the patient with a lower amount of serum and avoid gaseous air embolism through the needle to return.
White (2005) describes that if you remove the transmembrane pressure, reinfundir the blood slowly; check for signs of elimination of edema, local conditions of access, the General State of the patient, checking her vital signs and weight (noting signs of loss); walking conditions and you need rest; Guide about the importance of diet and medications, perform machine cleaning and sterilization of the dialyzer with their blood and venous lines and maintain unity in order. Ribeiro, (2009) adds, in the case of bruising applies cold compresses frequent during the 24 hours who succeed hemodialysis, after guiding the patient to warm compresses and ointment antitrombótica on site.
Customer care in haemodialysis should be done by a nurse with specialty and must receive constant training in this area because it is an impaired with low immune resistance and susceptible to several complications of arteriovenous Fistulas (white, 2005).
For Santana et. Al, (2013); The role of the nurse is not restricted in performing techniques or procedures efficiently, but also to plan and implement nursing care, supported by scientific knowledge, use its role as educator to educate patients, stimulating behavior change, thus preventing the potential complications.
2.8 COMPLICATIONS IN ARTERIOVENOUS FISTULAS
2.8.1 LOW FLOW
According to Fermi (2011), Furtado, (2006) when there is a partial obstruction of the venous branch due to the secondary fibrosis to multiple punctures, being this the most common cause. For the angels and Oselame, (2013) is usually caused by lack of blood flow, usually features venous resistance, fibrosis and obstruction. These situations also increase the incidence of blood circulation and, in this case, the infusion of an angiographic contrast that detects where is the lesion to be made to prevent the loss of the venous access.
2.8.2 THROMBOSIS
Second (Fermi, 2011), occurs for low flow in the fistula, dehydration, severe hypotension, or hypercoagulability. In case of obstruction by a blood clot, the fistula can be surgically clear with a Fogarty catheter when it is soon identified the obstruction.
2.8.3 HAND ISCHEMIA
It is more common in patients with previously compromised circulation, such as diabetics and elderly people with atherosclerosis. Is manifested by pain in the Office, or even at rest, and feeling of cold sweat, this happens due to the diversion of circulation (FERMI, 2011).
2.8.3 PSEUDOANEURYSM
The pseudoaneurysm of the venous branch is caused by the constant blood extravasation after dialysis needles, pseudoaneurysms require only observation and that take great care to puncture the fistula venous branch outside the site of injury. When an intense thinning of the skin behind the lesion must be repaired surgically (RIBEIRO, 2009)
2.8.4 INFECTIONS
Are rare, but when they occur staphylococcal origin and signs of inflammation at the site, as heat and hyperemia, and should be treated with antibiotics, according to Paiva, 2008 States that the diagnosis is based on local signs of inflammation.
For white, (2005) should be the collaboration of a multidisciplinary team to reduce the number of infections, and is also of fundamental importance to direct customers and their families how to care at home, and also the infection is closely related to those professionals who provide direct assistance to the client, hand washing should be performed in day to day practice.
Another relevant aspect as complications of AVF adds P, (2008) is the thrill and the presence of collateral veins. Both contribute to the stop of the fistula, if collateral vein is punctured can lead to stagnation of access, because blood flow pumped by AVF and evaluated by the intensity of the fret, both in the proximal region as the distal anastomosis.
The nurse should perform a physical examination of the AVF to be sure it is in good working order through observation of the development of the venous outflow, no irregular areas/dilated or aneurismaticas. Straight vein, with several areas that can be used to puncture. Partial collapse of the vein when the elevation of the limb. On palpation Stirrings in the arterial anastomosis, decreasing along the arterializada vein. Easy to compress. Soft and easy pulse detection in Sounding with stethoscope Low blow (low pitch) diastolic and systolic continuous (SHAH, 2009).
Given these complications Furtado, (2006) corroborates the importance of prevention of the complications of FAVS, and can be avoided if proper care are the they are properly administered.
3. METHODOLOGY
The survey was conducted through literature review, by the analysis of works published between the years 2005 to 2014, in the Portuguese language. Available materials were used in bibliographic databases, LILACS, Scielo and VHL, using key words: hemodialysis, nursing care, chronic kidney disease, arteriovenous fistula.
The data were collected and grouped according to the relevance with the proposed theme, being subsequently analyzed by individual reading.
The result of the research process with the databases were selected 17 (Seventeen) articles published, 03 (three) personal collection books, 01 (a) master’s thesis and 04 (four) electronic items of newspapers employed in the preparation of this study, we sought to identify the nursing care in patients under hemodialysis treatment fistulae.
We have included works that were directly related to the theme of the study. Were excluded from jobs that did not show relevant subsidies for research and those that have been published outside the scope of this review date.
For analysis and discussion of the results framework was developed with leading Authors that best addressed the proposed theme, being subsequently analyzed according to the relevance to the study.
4. RESULT AND DISCUSSION
FRAME WITH THE TOP AUTHORS WHO CONTRIBUTED TO THIS STUDY
| AUTHOR | ARTICLE TITLE | GOAL | METHODOLOGY | LANGUAGE |
| Santana .2013 et.al | Nursing care provided to patients under hemodialysis Treatment in Nephrology units | Identify the role of the nurse, juntoao patient under hemodialysis in Nephrology unit. | The referential bibliographic descriptive type, in which were found in the existing literature on virtual bases such as Scielo, LILACS and GoogleAcadêmico. | Portuguese |
| Fermi .2011 | Dialysis to nursing: guiaprático | Main purpose of this book is to collaborate on professional training of the nursing staff of the dialysis units. | Second Edition, consisting of 18 chapters, 220 págnas totally rewritten and deeply revised, is a new book, with at least twice as many illustrations of them produced especially for him. | Portuguese |
| Shah, 2009 | Take care of arterio-venous fistula: person of theoretical assumptions are the practical contexts. | Know which nursing care that nurses perform the person with arteriovenous fistula. | Descriptive and exploratory study to meet care practices that nurses direct to the person with chronic kidney failure, terminal with arteriovenous fistula. The sample consisted of 98 nurses from 15 hemodialysis centers, using a questionnaire to collect data. | Portuguese |
| P et.al .2008 | Maintenance of arteriovenous fistulas are made in the Centre of Nephrology of Caucaia-EC | Analyze the factors that led patients who perform hemodialysis losing FAV. | Descriptive study with a qualitative approach, carried out in a hemodialysis clinic located in Caucaia-CE, with the participation of 25pessoas (11mulheres and 14homens) that had a functioning FAV and lost at least once the permanent access. Data collection occurred through an interview, using a Semistructured script, containing identification data and the FAV care related, in order to meet the objectives proposed. | Portuguese |
| Maniva et al. .2009 | The patient in hemodialysis: self-care with arteriovenous fistula | Meet the self-care of hemodialysis patients with arteriovenous fistula (AVF). | This is descriptive study with a qualitative approach, undertaken in hemodialysis clinic in the city of Fortaleza-CE. To investigate 15 patients by means of a semi-structured interview, conducted with a tape recorder during hemodialysis sessions, also used charts. | Portuguese |
| Ribeiro et al. .2009 | Learning needs of nursing professionals in assisting patients with arteriovenous fistula | Identify the learning needs of nursing professionals in the provision of assistance to patients with arteriovenous fistula in hemodialysis, in order to improve the care provided to these patients. | This is a cross-sectional study, with data collection accomplished through semi-structured questionnaire given to nursing professionals operating in the hemodialysis unit of a Hospital Base of the interior of the State of São Paulo. 36 professionals, responded to this questionnaire. | Portuguese |
|
White et al., 2005 |
Nursing care in Chronic Renal Customer Care with vein arteriovenous fistula infection | Identify how have been conducted the nursing care on arteriovenous fistula and analyze the most frequent causes of fistula infection. | Qualitative, descriptive approach, using the ABNT, nurses from Nephrology Clinic of South zone of Rio de Janeiro were interviewed with a tape recorder and the lines being the words transcribed subsequently. |
Portuguese |
Source: authors themselves 2015
Twenty-five jobs used in this study, seven have addressed more satisfactorily the nursing care to FAV. Among which stressed the importance of the qualification of the nursery team Fermi, (2011), and should be scientifically based, trained and qualified to provide the patient a safe assistance.
This qualification not found in search for Shah, (2009) that showed deficits of knowledge of nurses in some specific areas of care for the person with AVF because the nurse nephrologist with scientific expertise relevant to the conservation importance of the FAV and the prevention of complications from specific nursing interventions in the patient with AVF.
Given that the nursing care as Santana et. Al, (2013) involves systematic from the entrance of the patient out of this hemodialysis session. The nurse should use the role of educator to educate patients about AVF, not detected in Cassava research et. Al, (2012) showed patients with knowledge about the production and care with the FAV. Already P et. Al., (2008) found that although patients have knowledge about the care of the AVF, the team of health professionals provides objective information and consisas regarding the preservation of the FAV.
Ribeiro et still stands out. Al, (2009) in its study it was found that the nursing professionals showed difficulties in the assistance provided to the patient with AVF, being touted as the most prevalent the Fav puncture, followed by the guidelines in providing hemostasis of assistance to patients with AVF. Once the first LP after the maturation of FAV’s nurse, hence the importance of having a trained nurse and with expertise in Nephrology, as well as investment in the in-service training in the various dialysis centers, because it is a client immune suppressed susceptible to several complications. (SHAH, 2009; WHITE et. Al, 2005).
Complications and care with the AVF were well described by Fermi, (2011) in his book concerned draw up an appropriate instrument of learning and contribute to nursing professionals perform in a manner determined his work and especially improving the quality of patient care.
White et al. (2005) were also chosen in the preparation of this work, although we do not admire the selection rules of articles for confection of literature review, a survey in relation to the date of this review, addressed to excellent way nursing care with arteriovenous fistula, pre care, trans and pós-hemodiálise. The authors highlighted that to achieve the excellence of care to patients under hemodialysis treatment nurse must be endowed with broad scientific expertise, in agreement with the other authors used in this research.
4. CONCLUSION
The study made it possible to meet the nursing care to arteriovenous fistula, which must be in order to improve the quality of life of patients with chronic renal failure using renal therapy service substitution through the FAV.
We realize that the FAV is the therapeutic modality of greater choice, because it is a longer lasting and secure access by having a higher survival rate and low rates of local complications. We also noticed that although it is a simple procedure, it must be very well planned site for anastomosis and pre care with patient’s self-care guidelines in the handling of your new access, the nurse will have to develop learning strategies that promote better adhesion on the part of the patient to treatment and post-operative nursing team employing a technique suitable tando fistula puncture , and withdrawal of the needle to obtain success in the procedure.
We were able to see though is a challenge for nursing care to patients with IRC and the nurse must be a specialist in Nephrology has a relevant scientific knowledge in relation to the procedure of making, conservation of the FAV. Must identify early problems evidenced with the AVF and act within their technical competence, ensuring the durability of the FAV and the extension of the life of the patient.
It is suggested that there are other works that describe the nursing care for the bearer of IRC in hemodialysis treatment for AVF in Brazil, which are scarce, mainly publications in Pará, because during our study few studies were found that describe the assistance of nursing hemodialysis service or related to arteriovenous fistula. Are also developed protocols for the Renal service Substititiva, for a standardized nursing care aiming at the improvement of care for these patients.
REFERENCES
White, Joyce Malik Arimatea; RANCIARO, Deborah. Nursing care in Chronic Renal customer with Artériovenosa Fistula infection. Nursing magazine, v. 27, n. 3, p. 12-30, 2005.
COSTA, Romanniny Hévillyn Silva et al. Scientific production on nursing in nephrology in Brazil. Journal of Nursing UFPE online[JNUOL/DOI: 10.5205/01012007], v. 5, n. 9, pp. 2276-2281, 2011.
DAS NEVES JUNIOR, Milton Adams et al. Evaluation of early patency of arteriovenous fistulas for hemodialysis. Jornal Vascular Brasileiro, v. 10, n. 2, p. 105-109, 2011.
DAUGIRDAS, John, BLAKE, Peter, TODD, s. Handbook of dialysis. Guanabara koogan, 2010.
DOS ANJOS, Marcela Dalosto; OSELAME, Abinet’s Barrios. Nursing care for elderly patients with arteriovenous fistula in hemodialysis therapy. UNIANDRADE magazine, v. 14, n. 3, p. 251-262, 2013.
DUTRA, Marina. et. Al. Evaluation of renal function in the elderly: a population-based study. J. Bras. Nephrology 2014; 36 (3). 297-303.
FERMI, Márcia Regina Brave. Dialysis to nursing: practical guide. Rio de Janeiro Guanabara Koogan, 2011. 220 p.
FURTADO, Angelina Masuku; LIMA, Francisca Elisângela Teixeira. Self-care of patients with chronic renal failure with arterio-venous fistula. Gaucho nursing magazine, v. 27, n. 4, p. 532, 2006.
Milk, Douglas squizatto, et. Al. Vascular consequences of using of CDL in patients under hemodialysis: echographic analysis of insertion sites in 2013. Brazilian society of Nephrology (2014; 36 (3): 320-324).
MANIVA, Samia Jardelle Costa de Freitas; FREITAS, Consuelo Elena Aires of. The patient in hemodialysis: self-care with arteriovenous fistula. Journal of Northeast Nursing Network-Rev Rene, v. 11, n. 1, 2012.
Paiva, Jermaine Regina Silva; LIMA, Francisca Elisângela Teixeira. Maintenance of arteriovenous fistulas are made in the Centre of Nephrology of Caucaia-CE. ROW rev. min. nurses, v. 12, n. 3, p. 313-320, 2008.
POLIMANTI, Alfonso Cézar, et. Al. Treatment of arteriovenous fistula theft by the technique of distal revascularization and arterial ligation: report of three cases. J. Vasc. Bras. 2012, vol. 11, no. 2. 158-161.
portal.anvisa.gov.br/wps/wcm/connect/…/manual_tecnovigilancia.pdf? Access date: 09 March 2015 at 1:00 pm.
PREZOTTO, Kelly Holland; ABREU, Izabella chroeder. The Chronic Renal and Patient adherence to treatment who are undergoing hemodialysis. Rev nurses UFPE online. Recife, 8 (3): 600-5, mar., 2014.
RAJA, r. c. h. m., et al. “Learning needs of nursing professionals in assisting patients with arteriovenous fistula.” Paul Nurse Act 22 (2009): 515-8.
SANCHO, Leyla Garcia; DAIN, Sulamis. Cost-effectiveness analysis regarding renal therapies instead: how to think about these interventions studies in Brazil? CAD. Saúde pública, Rio de janeiro, 24 (6): 1279-1290, jun 2008.
SANTANA, Suellen Silva; FONTENELLE, Taynnkelle; MAGALHÃES, Larissa Maciel. Nursing care provided to patients under hemodialysis treatment in Nephrology units. Journal of ITPAC, v. 6, n. 3, p. 1-11, 2013.
SESSO, Ricardo Cintra, et. Al. Report of the Brazilian census 2010 dialysis. J. Bras. Nefro. (2011; 33 (4): 442-447.
SILVA, Kleber Aparecido; Nunes, Zigmar Bannerjee. Nursing interventions more prevalent in a hemodialysis service to complications with arteriovenous fistula during the hemodialysis session. J Health Sci Inst., v. 29, n. 2, p. 110-3, 2011.
SMELTZER SC, Bare BG. Brunner & suddarth, et al. Treaty of Medical-Surgical Nursing. Rio de Janeiro: Guanabara Koogan,, 2009. 4V.
SHAH, Clement Nair. Take care of the person with arteriovenous Fistula: from the theoretical to the practical contexts. 2009. 209f. Dissertation (master of Science degree in nursing)-Abel Salazar Biomedical Sciences Institute of the University of Porto, Portugal, 2009.
Souza, Regina Ahmad; et. Al. Evaluation of vascular access for hemodialysis in children and adolescents: a retrospective cohort study of 10 years. J Bras Nefrol 2011; 33 (4): 422-430.
TOREGEANI, Jeferson Freitas, et. Al. Assessment of the maturation of arteriovenous fistulas for hemodialysis by eco-Doppler colour. J. Vasc. Bras. 2008, vol. 7, no. 3.
www.diarioonline.com.br/noticia-165839-.html. SESPA and SESMA clarify about chronic renal. Friday, 09/09/2011.
www.hgv.pi.gov.br/download/201204/HGV25_43447dbcff.pdf. access date 20 March 2015 at 8:00 pm. Handbook of dialysis/Nephrology 2012 HGV-PI.
www.saude.pa.gov.br. SESPA Portal. Access date: 10 March 2015 at 2:00.
[1] Paper presented to the Graduate Center (CPO ´ ‘s) of the Amazon (ESAMAZ). Lato Sensu graduate studies in nursing in Nephrology and Urology/Nurse.















